Urinary Tract Infection in Neurologic Patients Undergoing Intermittent Catheterization: A Systematic Review and Meta-Analysis of Catheter Type and Technique
Sara Skalli, Ihssane Hmamouchi, Redouane Abouqal, Najia Hajjaj-Hassouni, Samia Karkouri

TL;DR
This study finds that hydrophilic catheters reduce UTI risk in neurologic patients compared to uncoated catheters.
Contribution
The first meta-analysis evaluating catheter types and UTI risk in neurological patients undergoing intermittent catheterization.
Findings
Hydrophilic catheters are associated with a 47% lower risk of symptomatic UTI compared to uncoated catheters.
Moderate heterogeneity (I² = 49%) and substantial publication bias were observed in the meta-analysis.
Abstract
Intermittent urinary catheterization (IUC) is one of the recommended methods for bladder emptying in patients with bladder disorders. To our knowledge, no meta-analysis has yet evaluated the risk of urinary tract infections (UTIs) in adult neurological patients according to the type of catheter and IUC method. To address this knowledge gap, a systematic review of the literature was conducted using the PubMed, Embase, and Cochrane Trials CENTRAL databases, according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommendations. We included randomized clinical trials and cohort studies comparing at least two types of catheters and/or two IUC strategies in adult patients. Only studies published in French or English were considered. Heterogeneity was assessed using the I² statistic. A random-effects model was applied to estimate the pooled effect size…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
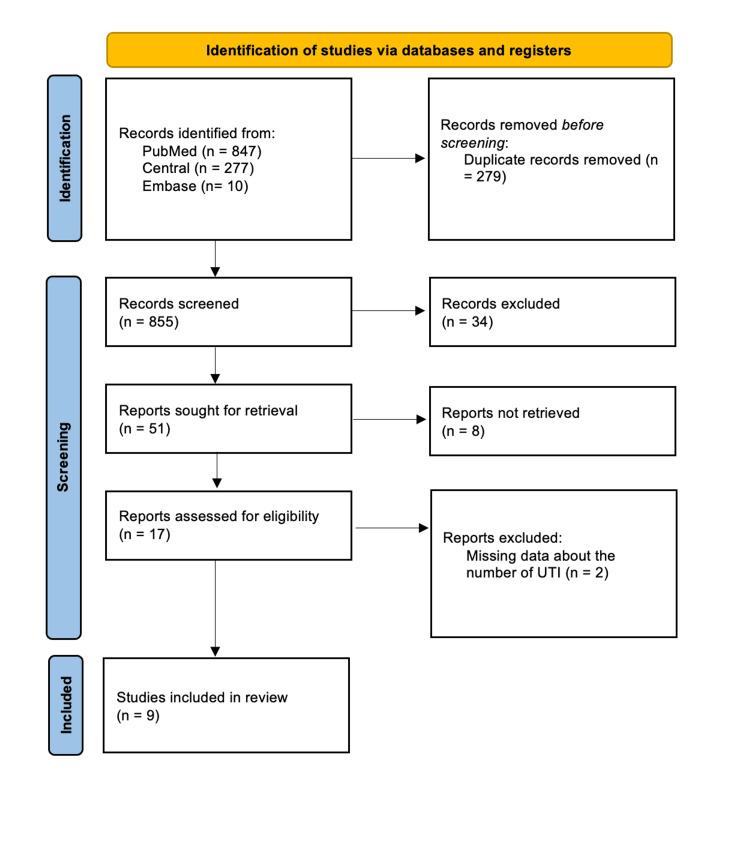 Figure 1
Figure 1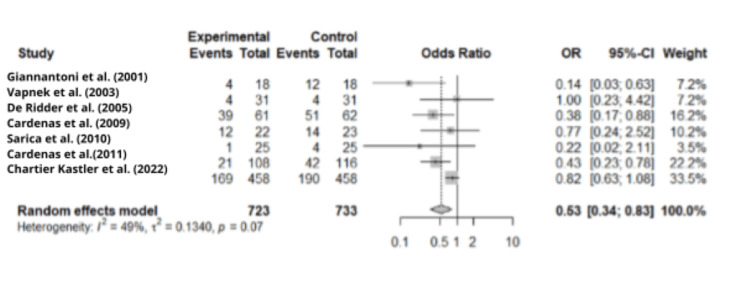 Figure 2
Figure 2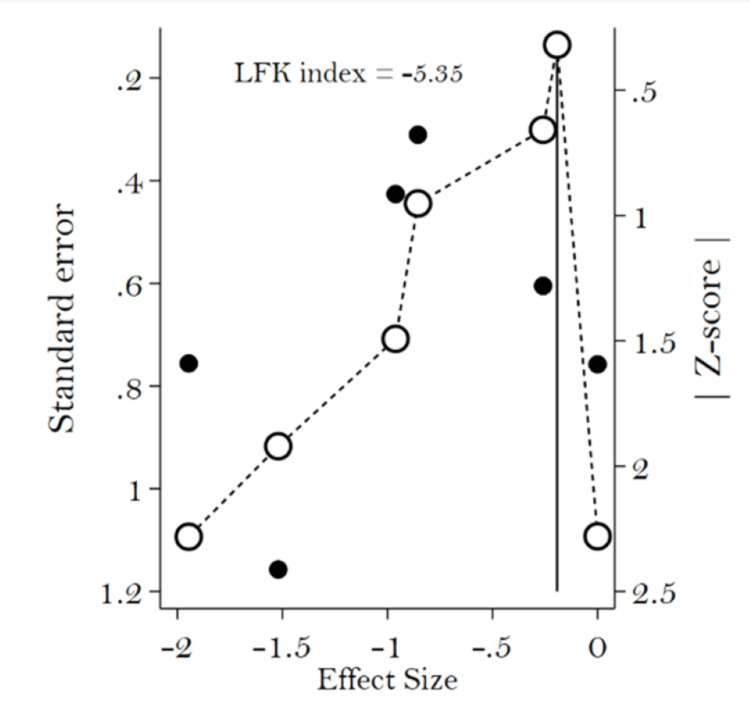 Figure 3
Figure 3| Terms | |
| 1 | (intermittent catheterization) OR (intermittent urinary catheterization) |
| 2 | (urinary tract infection) OR (urinary infection) OR (symptomatic urinary infection) |
| Population (P) | Neurologic adult patients with neurogenic urinary disorders |
| Intervention (I) | Intermittent catheterization |
| Comparison (C) | Type of catheter and/or technique of catheterization |
| Outcomes (O) | Urinary tract infection |
| Author | Study type | Random sequence generation (selection bias) | Allocation concealment (selection bias) | Blinding of participants and personnel (performance bias) | Blinding of outcome assessment (detection bias = self-reported) | Incomplete outcome data (attrition bias) | Selective reporting (reporting bias) | Other bias |
| Giannantoni et al. (2001) [ | Randomized crossover study | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Some concerns |
| Vapnek et al. (2003) [ | RCT | Some concerns | Low risk | Some concerns | Low risk | High risk | Low risk | Low risk |
| De Ridder et al. (2005) [ | RCT | Low risk | Low risk | Some concerns | Low risk | High risk | Low risk | Low risk |
| Moore et al. (2006) [ | RCT | Low risk | Low risk | Some concerns | Low risk | Low risk | Low risk | Low risk |
| Cardenas and Hoffman (2009) [ | RCT | Low risk | Some concerns | High risk | High risk | Low risk | Low risk | Low risk |
| Sarica et al. (2010) [ | RCT | Low risk | Some concerns | High risk | Some concerns | High risk | Low risk | Low risk |
| Cardenas et al. (2011) [ | RCT | Low risk | Low risk | High risk | Some concerns | High risk | Low risk | Low risk |
| Study | Study design | Selection | Comparability | Outcome | ||||||
| Representativeness of the exposed cohort | Selection of the non-exposed cohort | Ascertainment of exposure | Demonstration that the outcome of interest was not present at the start of the study | Comparability of cohorts on the basis of the design or analysis | Assessment of outcome | Was the follow-up long enough for outcomes to occur | Adequacy of follow-up of cohorts | Quality score | ||
| Spinu et al. (2012) [ | Cohort study | 1 | - | - | - | 2 | - | 1 | - | 4 |
| Chartier-Kastler et al. (2022) [ | Cohort study | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 7 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Tract Infections Management · Urinary Bladder and Prostate Research · Bladder and Urothelial Cancer Treatments
Introduction and background
Intermittent urinary catheterization (IUC) is recommended for managing bladder disorders, especially neurological ones [1]. This technique involves briefly inserting a catheter at regular intervals to completely empty the bladder [2]. It ensures clean and complete urination, reducing infections and improving quality of life [3]. Performing IUC requires physical, cognitive, and functional capacities. Self-catheterization occurs when the individual independently performs the procedure, while, in the case of significant impairment, a third party may perform it, known as hetero-catheterization. There are two main types of catheters [4]: uncoated (with or without pre-lubricated systems) and coated (hydrophilic or non-hydrophilic). They can be made from clear plastic polyvinyl chloride (PVC) or PVC-free materials.
IUC can be conducted using three techniques. Firstly, the sterile technique involves sterile gloves, a sterile container, and perineal disinfection with an antiseptic solution. Secondly, the aseptic technique requires a sterile single-use catheter, perineal disinfection with an antiseptic solution, and a no-touch technique avoiding direct manual contact with the catheter. Lastly, the clean technique involves clean hands and a clean container, along with perineal cleaning without an antiseptic solution. Catheters may be used once or reused for multiple subsequent catheterizations. Reused catheters can be cleaned with soap and water, soaked in a disinfectant solution, boiled, heated in a microwave, and stored for the next use [5]. Practices vary around the world, and there is no clear consensus.
Urinary tract infections (UTIs) pose a significant concern for IUC users, especially neurological patients with spinal cord injury (SCI) [6]. The Infectious Diseases Society of America (IDSA) defines catheter-associated UTI as the presence of symptoms or signs consistent with a urinary infection, with no identified source of infection, along with ≥10³ colony-forming units (CFU)/mL of ≥1 bacterial species in urine samples obtained from a catheter [7]. Symptoms may include fever, altered mental status, unexplained fatigue or lethargy, flank pain, acute hematuria, pelvic discomfort, dysuria, urgency, or frequent, painful, or sensitive suprapubic pain, especially in individuals who have had their catheter removed. For persons with SCI, the UTI definition also considers worsening spasticity, autonomic dysreflexia (sweating, bradycardia, increased blood pressure), or general malaise.
Despite scientific advances in catheter design and materials, there is no unanimous consensus regarding IUC practices. This systematic review and meta-analysis aimed to examine data regarding UTIs in adult neurogenic patients undergoing IUC, based on catheter type and catheterization technique.
Review
Methods
Review Design and Registration
This systematic review and meta-analysis were conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [8]. The review protocol was registered with PROSPERO under registration number CRD42023481012.
Search Strategy
A systematic literature search was performed in January 2023 using PubMed, the Excerpta Medica database (Embase), and the Cochrane CENTRAL trials. The search formula incorporated keywords combined with Medical Subject Headings (MeSH) terms: IUC, UTI, and neurogenic urinary disorders (Table 1).
Study Selection
Randomized clinical trials, as well as retrospective and prospective cohort studies, were included if they compared at least two types of catheters and/or two techniques of IUC in adult patients with neurogenic bladder. Participants included adults requiring IUC for neurogenic bladder management.
Selection Criteria
Inclusion criteria were articles published after 2000, up to January 2023, available in full text in French or English, involving neurogenic bladder disorders requiring IUC, and comparing at least two types of catheters and/or two techniques of IUC.
Exclusion criteria included letters to the editor, case reports, posters, recommendations from societies and experts, systematic reviews and meta-analyses, studies involving antiseptic or antibiotic prophylaxis, and studies on the pediatric population.
Outcome
The outcome analyzed was symptomatic UTI. Other outcomes, such as hematuria, patient satisfaction, preferences, quality of life, and economic outcomes, were not analyzed.
Data Extraction
Data collection followed PRISMA recommendations. Two authors (SS and SK) independently identified eligible papers based on title and abstract, and any disagreements were resolved by a third author (IH). Extracted data were entered into a pre-set table, and the manuscript was written according to PRISMA guidelines [8].
Risk of Bias Assessment
For randomized controlled trials, the Revised Cochrane Risk of Bias tool for randomized controlled trials (RoB 2) was employed [9]. For cohort studies, the Newcastle-Ottawa Scale was used [10].
Statistical Analysis
The analysis focused on research methodology, study population, catheter type, technique, UTI definition, and authors' conclusions. The odds ratio was the outcome measure. Statistical heterogeneity among included studies was estimated using I² (I² > 50% indicates significant heterogeneity). Due to expected heterogeneity, a random-effects model was adopted. Doi plots were used to assess publication bias based on the number of studies included in the meta-analysis, with Luis Furuya-Kanamori (LFK) index values outside the range of -1 to +1 indicating asymmetry and, therefore, significant publication bias [11]. Statistical analyses were performed using R software, version 4.3.2 (The R Foundation for Statistical Computing, Vienna, Austria) [12].
Results
Study Selection
The electronic searches identified 1,134 articles, resulting in 855 articles after duplicate removal. Subsequently, 804 articles were screened through title and abstract review based on predefined criteria. Of these, 17 of the 51 studies were eligible for full-text screening, and nine studies were ultimately included in the narrative review. The reasons for exclusion are detailed in Figure 1.
PRISMA flow diagram
For the meta-analysis, seven studies were included, while Spinu et al. (2012) [13] was excluded due to missing UTI data in each group, and Moore et al. (2006) [14] was excluded as it focused solely on the IUC technique. The flow of literature through the review process is illustrated in Figure 1 [8,15].
Study Characteristics
Sample sizes varied, with a median of 50 (36-123). Seven studies involved patients with SCI. Chartier-Kastler et al. (2022) [16] included people with neurogenic bladder without a specified etiology, and in Vapnek et al. (2003) [17], 56 individuals had SCI, while five had an unspecified neurogenic disorder. Age ranged from 22 to 75 years, with gender distribution varying across studies, predominantly including men. There was diversity in the duration of disease and IUC, as summarized in Appendices 1 and 2.
Risk of Bias Assessment
Randomized controlled trials were evaluated using the RoB2 tool, and cohort studies were evaluated using the Newcastle-Ottawa Scale. Consensus findings are presented in Tables 2-3. Most of the included studies used appropriate randomization techniques, but biases in detection and performance were more common. These results suggest that outcomes should be interpreted cautiously. Regarding the cohort studies, they exhibited overall moderate methodological quality, as both studies indicated sufficient representativeness of the exposed group and appropriate measurement of exposure. Nonetheless, constraints concerning the comparability of cohorts decreased confidence in the strength of their results.
Meta-Analysis on UTI and Type of Catheter
Given the limited number of studies comparing catheter insertion techniques, the meta-analysis focused exclusively on catheter types. A total of k = 7 studies were included in the analysis, involving a total sample size of 1,043. Spinu et al. (2012) [13] and Moore et al. (2006) [14] were excluded due to missing data and/or an exclusive focus on the IUC technique, respectively. Due to the limited number of studies, subgroup analysis was not possible.
The odds ratio was 0.53 (95% CI: 0.34-0.83). Analysis of the forest plot revealed heterogeneity among the included studies, with I² = 49%, approaching the threshold of significance (Figure 2). Publication bias, evaluated by the LFK index, was greater than |2|, as shown in the Doi plot (Figure 3).
Forest plot of urinary tract infection according to type of catheter
Bias of publication assessed with Doi plotLFK index, Luis Furuya-Kanamori Index
Discussion
This meta-analysis found that the use of hydrophilic catheters reduces UTI, but the sample size remained limited, studies were at moderate risk of bias, and publication bias was significant.
In terms of the methodology in the selected studies, seven of them were randomized clinical trials [14,17-22], while two were retrospective studies [13,16].
There is heterogeneity in patient characteristics, including age, gender distribution, disease duration, and IUC. This diversity may affect the generalizability of the results and should be considered when interpreting findings. Among the study population, seven studies involved patients with SCI. This focus on SCI reflects the high-risk profile of urinary and renal complications, highlighting the importance of early intervention. Indeed, research was predominantly conducted in hospital and short-term outpatient settings, except for the studies conducted by Spinu et al. (2012) [13] and Chartier-Kastler et al. (2022) [16], which focused on short- to medium-term IUC (within one year).
Regarding comparison based on catheter type: in the comparison of coated non-hydrophilic and uncoated catheters [18], the non-hydrophilic catheter showed superiority, albeit with a small sample size. As for the comparison between hydrophilic and coated non-hydrophilic catheters in Sarica et al. (2010) [21] and Chartier-Kastler et al. (2022) [16], no significant difference was found, although the pre-lubricated catheter demonstrated fewer UTIs. Spinu et al. (2012) [13] reported minimal differences. Finally, coated hydrophilic catheters were superior to uncoated ones in studies by Vapnek et al. (2003) [17], De Ridder et al. (2005) [19], and Cardenas et al. (2011) [22], with Cardenas and Hoffman (2009) [20] revealing no difference in symptomatic UTI numbers. However, the treatment of UTI with antibiotics was significantly reduced in the hydrophilic group.
Regarding IUC techniques, single-use no-touch was found superior to the sterile technique by Giannantoni et al. (2001) [18]. Vapnek et al. (2003) [17] reported no difference in urinary infection rates between single-use and multiple-use catheters, but the reduction was more significant in the single-use (hydrophilic) group. In contrast to hydrophilic catheters, dry catheters can be used multiple times. Moore et al. (2006) [14] revealed that the single-use clean technique resulted in fewer urinary infections compared to the sterile technique.
Several factors are considered when determining the reliability of meta-analysis results. First is the nature of the research. We included clinical trials with varying risk of bias, from low to moderate. The included cohort was of good quality. Second, the effects measured by odds ratios were accurate and had correct confidence intervals. Third, the endpoint definition of symptomatic UTI was clinically and biologically consistent across all studies included in the meta-analysis. However, it is important to note that there was a significant risk of publication bias. Therefore, our meta-analysis shows moderate confidence in the superiority of hydrophilic catheters in reducing UTIs in neurological patients undergoing intermittent catheter therapy.
Regarding catheter insertion technique, results did not support the sterile technique, and multiple use of catheters did not lead to an increase in UTIs. Current clinical trials, including MultiCath ISRCTN42028483 [23] in 520 patients and COMPARE NL8296 [24] in 456 patients, are aiming to evaluate multiple-use versus single-use catheters, with symptomatic UTI as the primary outcome. Notably, cost considerations in two studies indicated that clean catheters were less expensive than sterile ones [14], while hydrophilic and lubricated catheters were more expensive than dry ones [21]. From an ecological and economic perspective, future studies should focus on comparing multiple-use versus single-use catheters, especially in countries where catheters are not reimbursed, and the population has a low economic status.
Conclusions
IUC stands as a recommended technique for ensuring complete and efficient bladder emptying in neurological conditions. Various materials and techniques can be employed. Hydrophilic catheters appear to be associated with a lower risk of symptomatic UTI compared with uncoated ones, although the evidence is limited by a moderate risk of bias and potential publication bias. However, considering economic and environmental issues, forthcoming studies should prioritize the comparison of multiple-use versus single-use clean techniques, ensuring a substantial sample size and a unified definition of UTI.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Intermittent catheterization: Clinical practice guidelines from Association Française d'Urologie (AFU), Groupe de Neuro-urologie de Langue Française (GENULF), Société Française de Médecine Physique et de Réadaptation (SOFMER) and Société Interdisciplinaire Francophone d'Uro Dynamique et de Pelvi-Périnéologie (SIFUD-PP)Prog Urol GaméX PhéV Castel-Lacanal E 2322513020203222057110.1016/j.purol.2020.02.009 · doi ↗ · pubmed ↗
- 2An International Continence Society (ICS) report on the terminology for adult neurogenic lower urinary tract dysfunction (ANLUTD)Neurourol Urodyn Gajewski JB Schurch B Hamid R 115211613720182914950510.1002/nau.23397 · doi ↗ · pubmed ↗
- 3Value of intermittent self-catheterization for urinary retention (Article in French)Prog En Urol - FMC Raibaut P Terrier A Jacq C Hubeaux K Sheikh Ismaël S Amarenco G 2934182008
- 4Intermittent catheterisation for long-term bladder management (abridged Cochrane review)Neurourol Urodyn Prieto JA Murphy C Moore KN Fader MJ 6486533420152605402910.1002/nau.22792 · doi ↗ · pubmed ↗
- 5WITHDRAWN: Intermittent catheterisation for long-term bladder management Cochrane Database Syst Rev Prieto J Murphy CL Moore KN Fader M 08201710.1002/14651858.CD 006008.pub 4PMC 648332328796279 · doi ↗ · pubmed ↗
- 6Management of urinary tract infection in patients with spinal cord injuries Clin Microbiol Infect García Leoni ME Esclarín De Ruz A 780785920031461669710.1046/j.1469-0691.2003.00643.x · doi ↗ · pubmed ↗
- 7Diagnosis, prevention, and treatment of catheter-associated urinary tract infection in adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America Clin Infect Dis Hooton TM Bradley SF Cardenas DD 6256635020102017524710.1086/650482 · doi ↗ · pubmed ↗
- 8The PRISMA 2020 statement: an updated guideline for reporting systematic reviews Syst Rev Page MJ Mc Kenzie JE Bossuyt PM 891020213378134810.1186/s 13643-021-01626-4PMC 8008539 · doi ↗ · pubmed ↗