Staged, blood-sparing management of postmyocardial infarction ventricular septal rupture in a Jehovah's Witness
Yuichiro Fukumoto, Chiaki Aichi, Yusuke Imamura, Mototsugu Tamaki, Yasuhide Okawa, Hisao Suda, Hideki Kitamura

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
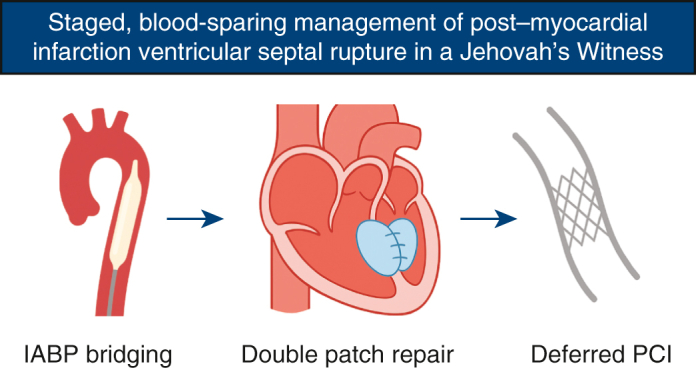 Figure 1
Figure 1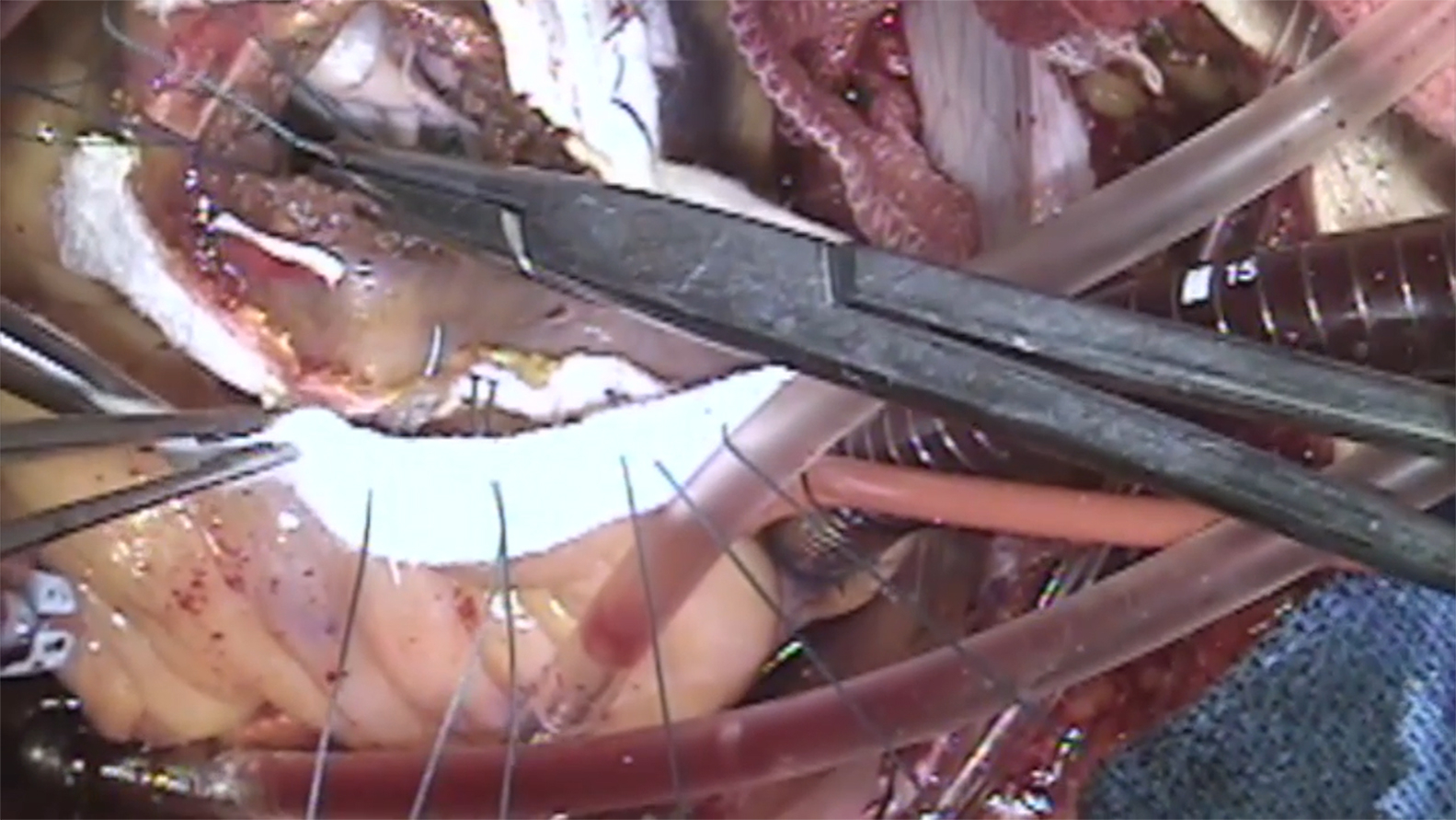 Figure 2
Figure 2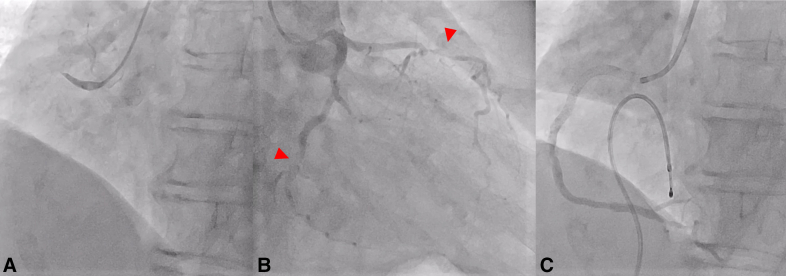 Figure 3
Figure 3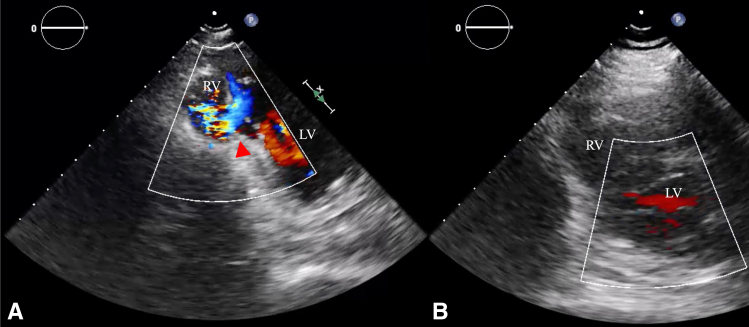 Figure 4
Figure 4 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Structural Anomalies and Repair · Blood transfusion and management · Transplantation: Methods and Outcomes
Blood-sparing VSR repair after MI in a Jehovah's Witness: IABP bridge and deferred PCI. Central MessageIn a Jehovah's Witness with post-MI VSR, IABP bridging, blood-sparing patch repair, and deferred PCI achieved transfusion-free recovery.
Postinfarction ventricular septal rupture (VSR) remains one of the most lethal mechanical complications of acute myocardial infarction (MI), with an incidence ≈0.2% and in-hospital mortality >40% despite reperfusion.1 For patients who are Jehovah's Witness (JW), refusal of transfusion complicates timing and perioperative management. We report transfusion-free repair using intra-aortic balloon pump (IABP) bridging, meticulous blood-sparing conduct, and deferred percutaneous coronary intervention (PCI).
Clinical Summary
A 75-year-old JW woman with hypertension, dyslipidemia, and smoking history presented 4 hours after symptom onset with inferior ST-segment elevation; she was resuscitated after transient ventricular fibrillation. Coronary angiography identified #1 culprit with critical residual disease in the left coronary system (Figure 1, A and B); flow improved to TIMI 2 after primary PCI to the right coronary artery (Figure 1, C).Figure 1. Preoperative coronary angiography shows (A and B) culprit 1 occlusion with severe residual disease in 7 (90%) and 14 (90%) (arrowheads) and (C) restoration of Thrombolysis In Myocardial Infarction 2 flow after primary percutaneous coronary intervention.
On day 6 after PCI, she developed back pain and a new systolic murmur. Echocardiography demonstrated a left-to-right shunt from the mid-septum to the apex (Qp/Qs = 1.8) (Figure 2, A), confirming post-MI VSR. Given transfusion refusal and hemoglobin 9.7 g/dL, we adopted a staged, blood-sparing plan: we optimized erythropoiesis with intravenous iron and erythropoietin, minimized phlebotomy, and proceeded to repair once hemoglobin and organ function improved, deferring residual revascularization. A pulmonary artery catheter was placed, and continuous hemodiafiltration was used for the first 4 days. She remained awake and not intubated. IABP was inserted via the right femoral artery from the onset, precluding ambulation. It was temporarily removed after stabilization to promote hematologic recovery and limit deconditioning but reinserted on day 10 for hemodynamic collapse requiring vasopressors. After a second removal, recurrent circulatory failure occurred, leaving no further opportunity for delay; surgery was performed on day 23 with hemoglobin 11.5 g/dL.Figure 2. Apical short-axis transthoracic echocardiography: (A) preoperative left-to-right shunt across an apical ventricular septal defect (arrowhead); (B) postoperative absence of residual shunt. RV, Right ventricle; LV, left ventricle.
VSR repair was performed via median sternotomy under standard cardiopulmonary bypass. A 3- × 2-cm apical septal defect was closed using a double-patch technique reinforced with felt (Video 1). Bypass and crossclamp times were 97 and 64 minutes, respectively. No blood products were administered.
The patient was extubated 3 hours postoperatively, and IABP was removed on postoperative day (POD) 1 (hemoglobin 8.0 g/dL). Postoperative echocardiography demonstrated complete closure (Figure 2, B). Deferred PCI for 7 and 14 was performed on POD 15 when hemoglobin recovered to 11.9 g/dL and inflammatory markers had subsided (Figure 3). She was transferred to rehabilitation on POD 35 and remains asymptomatic nearly 3 years postoperatively. Institutional review board approval was waived. Written informed consent for publication was obtained.Figure 3. Coronary angiography after deferred percutaneous coronary intervention demonstrates Thrombolysis In Myocardial Infarction 3 flow with 0% residual stenosis in 7 and 14.
Discussion
Once VSR was identified, management shifted to a staged, blood-sparing plan tailored to transfusion refusal. Our JW program uses a structured, multidisciplinary protocol. For elective surgery, based on previous reports,2^,^3 we target preoperative hemoglobin ≥12 g/dL using intravenous iron, erythropoietin, vitamin B12, and folate, combined with hemodilutional autologous transfusion, cell-salvage reinfusion, and meticulous hemostasis. In this case, the same framework was applied pragmatically, proceeding to repair when hemoglobin and tissue integrity were acceptable.
The choice of mechanical support is pivotal. Although Impella (Abiomed) provides active unloading, studies show higher rates of bleeding, hemolysis, and transfusion than with IABP.4^,^5 For patients who JW, IABP offers balanced circulatory support while conserving hemoglobin. To reduce bleeding risk and procedural complexity under severe anemia, the initial operation was deliberately limited to septal repair. Meticulous hemostasis and restrained bypass and clamp times enabled smooth separation and early recovery, and deferred PCI after stabilization completed full revascularization.
Overall, this experience suggests a stepwise strategy—physiologic IABP bridging, blood-sparing surgery, and deferred PCI—may be a feasible option for selected post-MI VSR in JW. At our center, >60 transfusion-free cardiac operations in JW, including urgent cases, have yielded zero operative mortality, supporting the practicality of such an individualized approach.
Conflict of Interest Statement
The authors reported no conflicts of interest.
The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Elbadawi A.Elgendy I.Y.Mahmoud K.Temporal trends and outcomes of mechanical complications in patients with acute myocardial infarction JACC Cardiovasc Interv 121820191825183610.1016/j.jcin.2019.04.03931537282 · doi ↗ · pubmed ↗
- 2Tanaka A.Ota T.Uriel N.Cardiovascular surgery in Jehovah’s witness patients: the role of preoperative optimization J Thorac Cardiovasc Surg 15042015976983.e 1-310.1016/j.jtcvs.2015.06.05926211405 · doi ↗ · pubmed ↗
- 3Spahn D.R.Schoenrath F.Spahn G.H.Effect of ultra-short-term treatment of patients with iron deficiency or anaemia undergoing cardiac surgery: a prospective randomised trial Lancet 3931018720192201221210.1016/S 0140-6736(18)32555-831036337 · doi ↗ · pubmed ↗
- 4Thakkar S.Patel H.P.Kumar A.Outcomes of Impella compared with intra-aortic balloon pump in ST-elevation myocardial infarction complicated by cardiogenic shock Am Heart J Plus 12202110006710.1016/j.ahjo.2021.100067 PMC 1097813438559603 · doi ↗ · pubmed ↗
- 5Ahmed M.Bano S.Asif M.Sidra F.N.U.Ram M.Bibi S.Impella vs intra-aortic balloon pump in patients with acute myocardial infarction complicated with cardiogenic shock: an updated systematic review and meta-analysis Glob Cardiol 312025