Surgical strategy for lung transplantation in Kartagener syndrome
Naoki Date, Daisuke Nakajima, Ichiro Sakanoue, Hidenao Kayawake, Satona Tanaka, Hiroshi Date

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
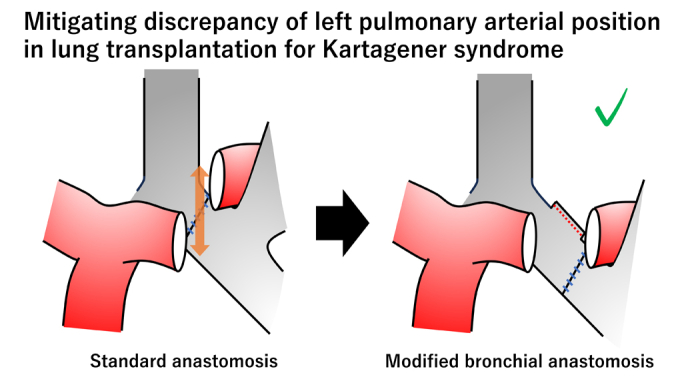 Figure 1
Figure 1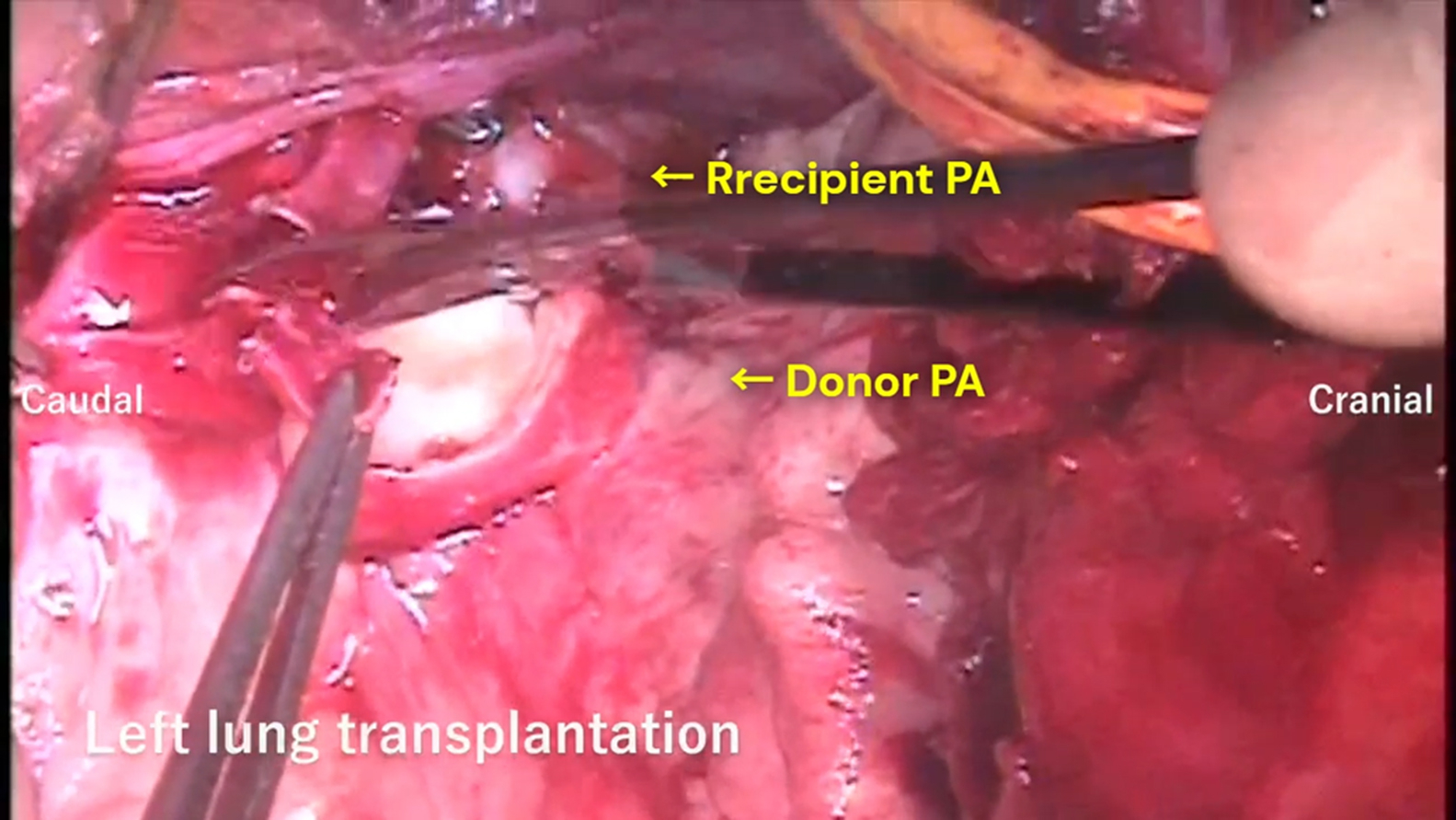 Figure 2
Figure 2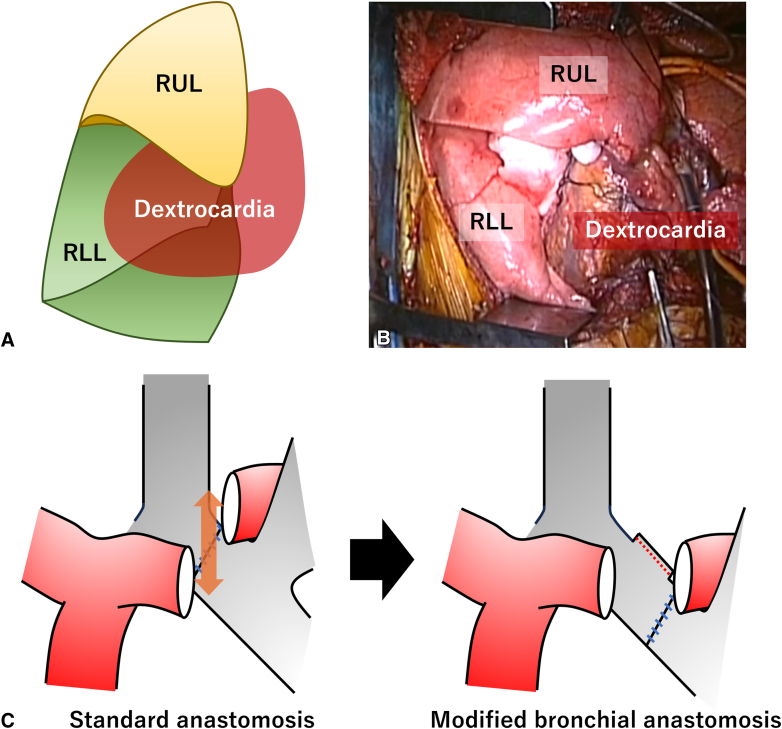 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTransplantation: Methods and Outcomes · Cystic Fibrosis Research Advances · Pulmonary Hypertension Research and Treatments
Modified bronchial anastomosis facilitates vascular anastomoses in Kartagener syndrome. Central MessageRight middle lobectomy of the donor lung graft and bronchial anastomosis of the recipient's left bronchus intermedius enable safe lung transplantation in Kartagener syndrome.
Kartagener syndrome is a rare autosomal-recessive disorder characterized by the triad of situs inversus, bronchiectasis, and sinusitis. Lung transplantation in patients with Kartagener syndrome poses unique surgical challenges because of situs inversus. First, dextrocardia can compress the implanted right lung. In addition, reversed hilar structures complicate bronchus and pulmonary vessels anastomosis. In this study, we present our surgical strategy for lung transplantation in patients with Kartagener syndrome.
Case Series
From January 2017 and December 2024, we performed bilateral lung transplantation in 4 patients with Kartagener syndrome. The cohort included 1 man (42 years) and 3 women (44, 49, and 57 years). All procedures used a clamshell thoracotomy under extracorporeal circulation (1 cardiopulmonary bypass and 3 extracorporeal membrane oxygenation cases). The institutional review board of Kyoto University Hospital approved this study on May 30, 2024 (reference number: R2389), and all patients provided written informed consent for the publication of study data.
The following surgical strategy was applied in all cases. First, during right lung transplantation, the donor's right middle lobe was resected on the back table, with the bronchial stump closed to accommodate the recipient's dextrocardia (Figure 1, A and B). Bronchial and vascular anastomoses were performed on the right side in the standard manner. Second, in left lung transplantation, the graft's left main bronchus was anastomosed to the recipient's left bronchus intermedius, with the recipient's left upper lobe bronchus closed. This modification shifted the hilar structures of the donor lung caudally, thereby minimizing the positional discrepancy between the donor and recipient pulmonary arteries (Figure 1, C). This allowed tension-free anastomoses of the left pulmonary artery and vein. No bronchial stump coverage was performed. After graft reperfusion, all patients were weaned from extracorporeal support intraoperatively in the usual manner (Video 1).Figure 1. Schema (A) and picture (B) of middle lobectomy in the donor lung graft to accommodate dextrocardia. C, In the modified procedure, the donor left main bronchus was anastomosed to the recipient's left bronchus intermedius, which mitigated the positional discrepancy of the donor and recipient pulmonary arteries. RUL, Right upper lobe; RLL, right lower lobe.
The operative and posttransplant outcomes are summarized in Table 1. Severe pleural adhesions were observed in all cases, resulting in prolonged operative time (564-721 minutes) and substantial blood loss (3160-17,000 mL), which was managed through continuous blood transfusion under careful monitoring of the bleeding volume. One patient required delayed chest closure on postoperative day 3. All patients were managed with a tracheostomy for frequent sputum suctioning and required prolonged postoperative mechanical ventilation (13-41 days). No bronchial or vascular anastomotic complications occurred. Regarding long-term survival, 1 patient died of chronic allograft dysfunction 6 years after transplantation, whereas 3 patients survived uneventfully for 1 year, 2 years, and 4 years.Table 1. Operative and posttransplant outcomes of the patientsCaseAge/sexSize matching, %∗ECCECC time, minOperative time, minBlood loss, mLBlood transfusion, mLComplications/notePostoperative ventilation, dICU stay, dHospital stay, dSurvival, yCause of death144/F28.3CPB2605648825RBC: 1960FFP: 2640PLT: 800Pleural effusionPneumonia1391026CLAD249/F−5.2ECMO3406873340RBC: 840FFP: 1920PLT: 200Atelectasis of right lower lobe371163>4−342/M8.7ECMO4637213160RBC: 280FFP: 2640PLT: 400Pneumothorax411771>2−457/F−8.8ECMO29059817,000RBC: 1960FFP: 4650PLT: 600Delayed chest closure at POD3132063>1−ECC, Extracorporeal circulation; ICU, intensive care unit; F, female; CPB, cardiopulmonary bypass; RBC, red blood cell; FFP, red blood cells; PLT, platelets; CLAD, chronic lung allograft dysfunction; ECMO, extracorporeal membrane oxygenation; M, male; POD, postoperative day.∗Size matching = (predicted donor vital capacity/recipient predicted vital capacity − 1) × 100. Based on the Japan Organ Transplant Network criteria, lung transplantation is eligible when the value is between −30% and +30%.
Discussion
In patients with Kartagener syndrome, a small right chest cavity can cause donor right lung graft oversizing, which can lead to atelectasis of the implanted right lung graft.1 Although right lower-lobe resection has been reported as a downsizing strategy,2 we chose right middle-lobe resection. Given its anatomical location in the anteroinferior space of the right chest cavity, right middle lobectomy creates adequate space for the recipient's dextrocardia. In addition, various techniques, such as mobilization of the donor pulmonary artery or elongation of the vascular cuffs, have been reported to treat reverse hilar structures.1^,^3 Our approach uniquely featured bronchial anastomosis at the level of the recipient's left bronchus intermedius to adjust the position of the donor's left hilar vessels. This modified technique facilitates left pulmonary arterial and venous anastomoses without complications.
Our surgical strategy included leaving the bronchial stumps of the recipient's left upper-lobe bronchus and the donor's right middle-lobe bronchus closed. Potential concerns exist regarding bronchopleural fistulas; however, we believe that leaving bronchial stumps closed is considered acceptable. The donor's right middle bronchial stump may have the potential benefit of being covered by the remaining right upper and lower lobes, although there is no strong evidence that this reduces the risk of bronchopleural fistula compared with other types of lobectomies. Careful observation of the bronchial stump is required. We have reported that leaving recipient's bronchial stump is safe.4 The recipient's left upper bronchial stump healed well as a result of maintained bronchial arterial circulation. In conclusion, bilateral lung transplantation for Kartagener syndrome can be performed safely, with favorable outcomes using the presented surgical strategy.
Conflict of Interest Statement
The authors reported no conflicts of interest.
The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yamamoto H.Sugimoto S.Miyoshi K.Otani S.Yamane M.Toyooka S.Lung transplantation for Kartagener syndrome: technical aspects and morphological adaptation of the transplanted lungs Gen Thorac Cardiovasc Surg 693202158859210.1007/s 11748-020-01509-w 33026567 · doi ↗ · pubmed ↗
- 2Brioude G.D’journo X.B.Reynaud-Gaubert M.Thomas P.A.Bronchial fistula after lobar size reduction for bilateral lung transplantation in Kartagener’s syndrome: a surgical challenge Interact Cardiovasc Thorac Surg 171201318418610.1093/icvts/ivt 15623575755 PMC 3686406 · doi ↗ · pubmed ↗
- 3Gauthier J.M.Takahashi T.Bierhals A.J.Technical considerations for lung transplantation in Kartagener's syndrome Ann Thorac Surg 10752019 e 337e 33910.1016/j.athoracsur.2018.08.09530612988 · doi ↗ · pubmed ↗
- 4Kayawake H.Chen-Yoshikawa T.F.Aoyama A.Surgical management of bronchial stumps in lobar lung transplantation J Thorac Cardiovasc Surg 1561201845146010.1016/j.jtcvs.2017.10.15029730119 · doi ↗ · pubmed ↗