Pulsed Field Ablation for Ventricular Arrhythmia in Repaired Tetralogy of Fallot
Nili Schamroth Pravda, Lorenzo Caratti di Lanzacco, Rui Shi, Ghada D. Mustafa, Sabine Ernst

TL;DR
Pulsed field ablation is used to treat heart rhythm issues in a repaired Tetralogy of Fallot patient before a valve replacement.
Contribution
This is the first reported use of focal pulsed field ablation for ventricular arrhythmia in repaired Tetralogy of Fallot.
Findings
Focal PFA achieved bidirectional block in a slow conduction zone without complications.
The procedure demonstrated feasibility and short-term safety for arrhythmia management before pulmonary valve replacement.
PFA may serve as a pre-emptive substrate modification strategy in repaired Tetralogy of Fallot patients.
Abstract
Ventricular arrhythmias are a major late complication in patients with repaired Tetralogy of Fallot (TOF), frequently originating from slow conduction zones within surgical isthmuses. Pulmonary valve replacement (PVR) may limit future ablation access, prompting interest in pre-emptive substrate modification. Pulsed field ablation (PFA) is a novel nonthermal ablation modality with potential safety advantages. A 45-year-old man with repaired TOF and severe pulmonary regurgitation underwent a pre-PVR electrophysiology study, which identified a slow conduction zone at isthmus 3, located between the right ventricular outflow tract and the ventricular septal defect patch. Focal PFA achieved bidirectional block without complications. This first reported use of focal PFA for ventricular arrhythmia substrate modification in TOF demonstrates its feasibility and short term safety, supporting its…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
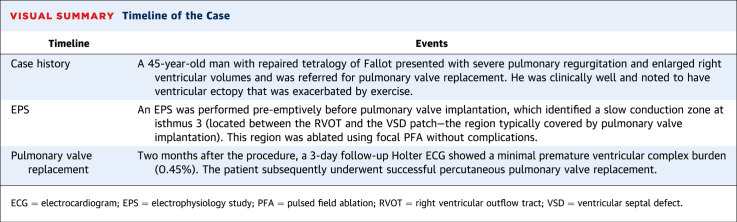 Figure 1
Figure 1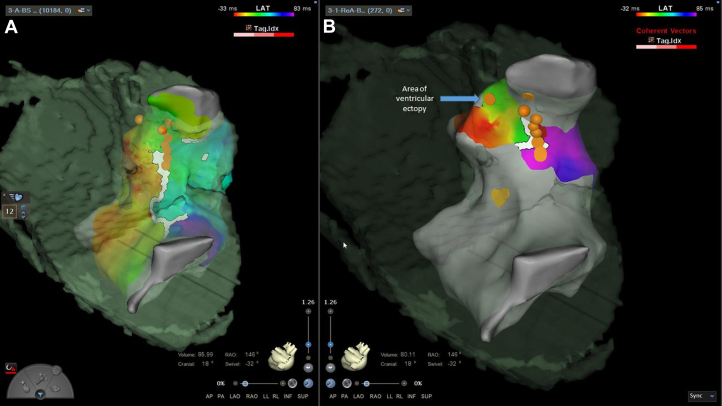 Figure 2
Figure 2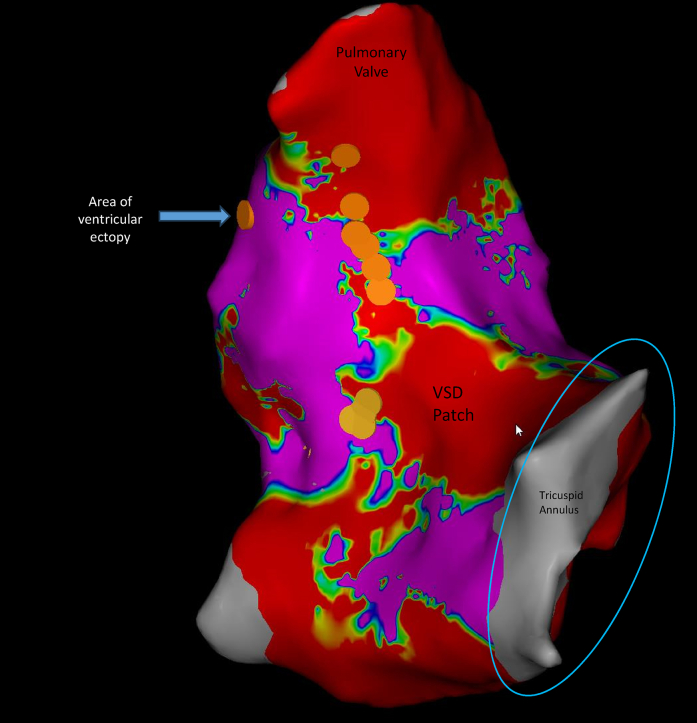 Figure 3
Figure 3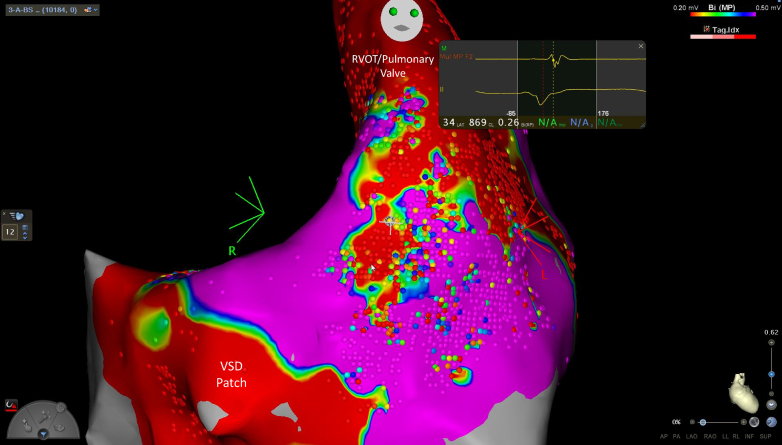 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrhythmias and Treatments · Congenital Heart Disease Studies · Atrial Fibrillation Management and Outcomes
Patient with tetralogy of Fallot (TOF) are at increased risk of sudden cardiac death due to ventricular arrhythmias.1 Recent studies have advanced the understanding of the pathophysiology of ventricular ectopy and ventricular tachycardia (VT) in TOF, particularly emphasizing the role of anatomical re-entry circuits known as electrical isthmuses.1 These isthmuses are regions of slow conduction and can be targeted by arrythmia ablation.
Four distinct isthmuses have been described in TOF. Among these, isthmus 3, located between the right ventricular outflow tract (RVOT) and the ventricular septal defect (VSD) patch, is most frequently implicated.
Its narrow width, thin myocardial wall, and frequent involvement of surgical scar make it highly susceptible to slow conduction and re-entry, explaining its predominant role in VT circuits.2
Importantly, isthmus 3 often becomes inaccessible after pulmonary valve replacement (PVR), further highlighting the rationale for pre-emptive substrate modification in this setting.3
Pulsed field ablation (PFA) is an emerging ablation technology that delivers high-energy pulsed electric fields to induce irreversible electroporation, achieving tissue-selective myocardial ablation without the thermal injury associated with conventional radiofrequency (RF) or cryothermal energy.4 Although PFA has shown early promise in the treatment of ventricular arrhythmias,5 we report the first use of focal PFA for the treatment of ventricular ectopy in a patient with repaired TOF.
History of Case Presentation and Past Medical History
A 45-year-old man with TOF, after surgical repair in childhood with a monocusp reconstruction of the RVOT, presented with severe pulmonary regurgitation and enlarged right ventricular volumes.
Investigations
Cardiac magnetic resonance imaging demonstrated an indexed right ventricular diastolic volume of 152 mL/m^2^, with moderate right ventricular hypertrophy and preserved right ventricular function, with an ejection fraction of 58%. Also noted was a 38-mm region of akinesia below the RVOT, concurred with the region of the transannular patch.
The patient underwent a cardiopulmonary exercise test. He was able to exercise for 12 minutes 54 seconds, achieving a peak oxygen consumption of 24.7 mL/kg/min (66% of predicted), with ventricular ectopy including couplets on exercise with a 7-beat run of nonsustained VT during Bruce stage 5 and a maximum 5-beat nonsustained VT in early recovery. The main morphology was left bundle branch block–like, with transition at lead V_3_/V_4_ and an inferior axis (see baseline electrocardiogram [ECG] in Supplemental Figure 1 and ECG during exercise in Supplemental Figure 2). He was treated with a β-blocker (bisoprolol 2.5 mg once daily) for ventricular ectopy.
The baseline ECG in sinus rhythm showed right bundle branch block (QRS duration 126 ms) with intermittent PR prolongation (250 ms).
Management
The patient was referred for an electrophysiology study and ablation before percutaneous pulmonary valve implantation.
At the outset of the procedure, the patient had frequent ectopy with couplets and triplets, and no pharmacological induction was necessary during the procedure. Activation mapping and voltage mapping were performed in the right ventricle, demonstrating a large scare corresponding to the transannular patch in the anterior RVOT and a slow conduction zone with late potentials between the scar and the region of the VSD patch/tricuspid annulus (Figures 1, 2, and 3). Five linear focal applications of PFA were delivered over this region (22 A for 4 seconds, energy delivery duration 2.4 ms, target contact force >5 g, constant irrigation flow 4 mL/min, biphasic monopolar energy application; CardioFocus Centauri focal PFA system). The standard protocol was used as previously described.6 Preprocedural computer tomography demonstrated the left anterior descending artery posterior and inferior to the pulmonary outflow tract. The ECG was closely inspected for ST-segment changes during the procedure, but intravenous nitrates were not needed. Block over the anatomical isthmus was demonstrated by reperforming activation mapping and pacing on both sides of the ablation line (Figure 1B). A further single application of PFA was delivered to a separate region of ventricular ectopy, with a change in the morphology of the ectopic beats. A right ventricular stimulation protocol was performed without induction of ventricular arrhythmia (3 extrastimuli from the right ventricular apex and outflow tract, with a cycle length of 510 ms for S2 and 440 ms for S3). There were no complications after the procedure.Figure 1. Activation Map of the Right VentriclePosterior projections showing early to late activation mapping, demonstrating isthmus 3 below the pulmonary annulus and the region of ablation. (A) Activation map before ablation with overlying ablation points. (B) Activation map postablation with overlying ablation points.Figure 2. Voltage Map of the Right Ventricle Showing the Regions of AblationVoltage mapping showing the region of slow conduction between the ventricular septal defect (VSD) patch and the pulmonary annulus as well as the area where ablation was delivered.Figure 3. Voltage Map of the Right Ventricle Showing the Region of Slow Conduction Over Isthmus 3Voltage mapping showing the region of slow conduction between the ventricular septal defect (VSD) patch and the pulmonary annulus. RVOT = right ventricular outflow tract.
Follow-Up
There were no postprocedure complications. Two months after the procedure, a 3-day follow-up Holter ECG showed a 0.45% premature ventricular complex burden of different morphologies. The patient subsequently underwent successful percutaneous PVR.
Discussion
To our knowledge, this is the first reported use of PFA for the treatment of ventricular ectopy/VT in a patient with repaired TOF. This case illustrates the convergence of 2 evolving paradigms in congenital electrophysiology: 1) the growing advocacy for pre-emptive VT substrate ablation before PVR; and 2) the emergence of PFA as a tissue-selective, nonthermal energy modality for cardiac ablation.
Ablation prior to PVR: Timing matters
Ventricular arrhythmias remain a significant cause of late morbidity and mortality in patients with repaired TOF, largely because of macro-re-entrant circuits that develop in anatomical and surgical isthmuses—most commonly isthmus 3 (located between the pulmonary valve annulus and the VSD patch).7 As patients survive to older age, degeneration of the pulmonic valve requiring intervention becomes more frequent.8 Importantly, PVR can render the area of isthmus 3 inaccessible from an endocardial approach, potentially precluding future catheter ablation.6 Preoperative electrophysiology study and ablation have been advocated by Bouyer et al3 for risk stratification and targeted ablation, with potential reduction in postoperative arrhythmia burden.
Pulsed field ablation: A new frontier
PFA represents a novel nonthermal ablation modality that uses high-voltage pulsed electric fields to induce irreversible electroporation, resulting in targeted myocardial cell death while minimizing injury to surrounding structures. This stands in contrast to traditional thermal ablation methods, such as RF ablation or cryoablation, which carry a risk of collateral damage to critical adjacent tissues, including coronary arteries, nerves, and cardiac valves.4
Preclinical and early clinical studies suggest that PFA offers several advantages: high tissue selectivity, less dependence on catheter contact force, and the ability to create durable lesions in challenging substrates, such as trabeculated or surgically altered myocardium.4 Although the majority of PFA research to date has focused on pulmonary vein isolation for atrial fibrillation, recent studies have begun exploring its use for VT, with early data reported by Della Rocca et al9 and Lozano-Granero et al.5
Recent developments in point-by-point PFA using energy levels of 22–25 A have further expanded the potential applications of this technology. These protocols allow precise focal lesion delivery without significant temperature elevation, enhancing procedural safety.9 This approach may be particularly well-suited for ablating narrow critical isthmuses, such as those encountered in patients with TOF, where precision and avoidance of collateral damage are paramount. In our experience, PFA was a quicker, more stable, and easier application than traditional RF ablation, in which longer applications in unusual anatomical positions can be challenging.
Despite its promise, PFA remains an emerging technology. Key aspects, including lesion depth, recurrence rates, and long-term safety in ventricular tissue, require further evaluation, especially in younger patients with congenital heart defects.
The present case adds to the limited but growing body of evidence supporting the feasibility of PFA for VT substrate modification in complex congenital heart disease. Specifically, it demonstrates successful PFA delivery in a patient with TOF, highlighting the potential role of this technology in expanding treatment options for arrhythmia management in this unique population.
Funding Support and Author Disclosures
Prof Sabine Ernst is a consultant for Biosense and Stereotaxis. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.Take-Home Messages
- •This case demonstrates the feasibility of using focal pulsed field ablation for the treatment of ventricular tachycardia in patients with tetralogy of Fallot.
- •It highlights the role of pre-emptive substrate modification before pulmonary valve replacement in patients with tetralogy of Fallot.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Krieger E.V.Zeppenfeld K.De Witt E.S.Arrhythmias in repaired tetralogy of Fallot: a scientific statement from the American Heart Association Circ Arrhythm Electrophysiol 15112022 e 00008410.1161/HAE.000000000000008436263773 · doi ↗ · pubmed ↗
- 2Ramdat Misier N.L.de Groot N.M.S.Multimodality assessment of anatomical isthmuses in tetralogy of Fallot: check the weather before setting sail!JACC Clin Electrophysiol 105202486786910.1016/j.jacep.2024.03.01738811069 · doi ↗ · pubmed ↗
- 3Bouyer B.Jalal Z.Daniel Ramirez F.Electrophysiological study prior to planned pulmonary valve replacement in patients with repaired tetralogy of Fallot J Cardiovasc Electrophysiol 3462023139514043723242610.1111/jce.15940 · doi ↗ · pubmed ↗
- 4Chun K.-R.J.MiklavčičD.Vlachos K.State-of-the-art pulsed field ablation for cardiac arrhythmias: ongoing evolution and future perspective Europace 2662024 euae 13410.1093/europace/euae 134PMC 1116050438848447 · doi ↗ · pubmed ↗
- 5Lozano-Granero C.Hirokami J.Franco E.Case series of ventricular tachycardia ablation with pulsed-field ablation: pushing technology further (into the ventricle)JACC Clin Electrophysiol 992023199019943722735810.1016/j.jacep.2023.03.024 · doi ↗ · pubmed ↗
- 6Niu M.C.Pilcher T.A.Etheridge S.P.Before it is too late: pre-emptive ablation strategies in tetralogy of Fallot Europace 2632024 euae 06410.1093/europace/euae 064PMC 1096497838530795 · doi ↗ · pubmed ↗
- 7Moore J.P.Seki A.Shannon K.M.Mandapati R.Tung R.Fishbein M.C.Characterization of anatomic ventricular tachycardia isthmus pathology after surgical repair of tetralogy of Fallot Circ Arrhythm Electrophysiol 6520139059112388419910.1161/CIRCEP.113.000450 · doi ↗ · pubmed ↗
- 8Baumgartner H.De Backer J.Babu-Narayan S.V.2020 ESC guidelines for the management of adult congenital heart disease Eur Heart J 42620215636453286002810.1093/eurheartj/ehaa 554 · doi ↗ · pubmed ↗