Percutaneous Vegetectomy for Infective Endocarditis in a Nonsurgical Candidate
Giovanni Zlaket, Boris Yushuvayev, Paul Gilbert, Samier Deen, Cece Ibeson, Seema Jain, Azeen Elahi, Danielle Stearns, Joshua Waggoner, Kara Asbury

TL;DR
This paper presents a case where a minimally invasive AngioVac procedure was used to treat infective endocarditis in a patient who could not undergo surgery.
Contribution
The paper introduces percutaneous vegetectomy as a viable alternative for treating infective endocarditis in nonsurgical candidates.
Findings
The AngioVac system was successfully used in a patient with persistent bacteremia and tricuspid valve endocarditis.
Percutaneous aspiration can be a treatment option when surgical intervention is not feasible.
The procedure is suitable for patients with large vegetations and poor surgical candidacy.
Abstract
Surgical management is recommended for infective endocarditis (IE) when there is right heart failure due to severe tricuspid regurgitation, recurrent septic pulmonary emboli, persistent bacteremia, and large tricuspid valve vegetations (≥20 mm). However, sternotomy comes with strict eligibility limitations, including poor functional status, respiratory failure, and recent intravenous drug use. A 55-year-old woman with a history of intravenous drug use was diagnosed with persistent bacteremia in the setting of tricuspid valve endocarditis. Poor surgical candidacy prompted consideration of less invasive alternatives, including percutaneous aspiration. This case highlights the viability of AngioVac vegetectomy as an alternative treatment modality for persistent IE in poor surgical candidates. Surgical intervention is considered for right-sided native valve IE with vegetations ≥20 mm,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1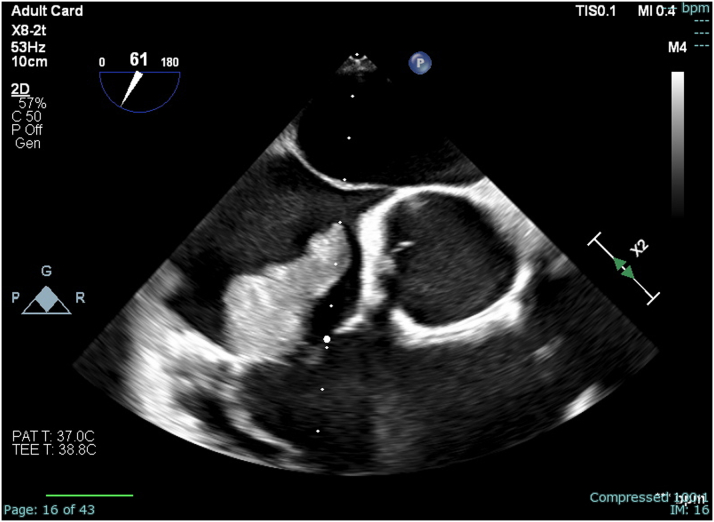 Figure 2
Figure 2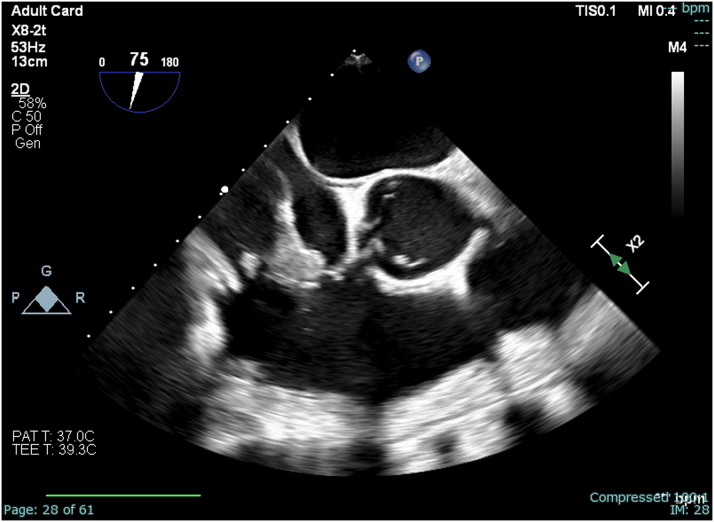 Figure 3
Figure 3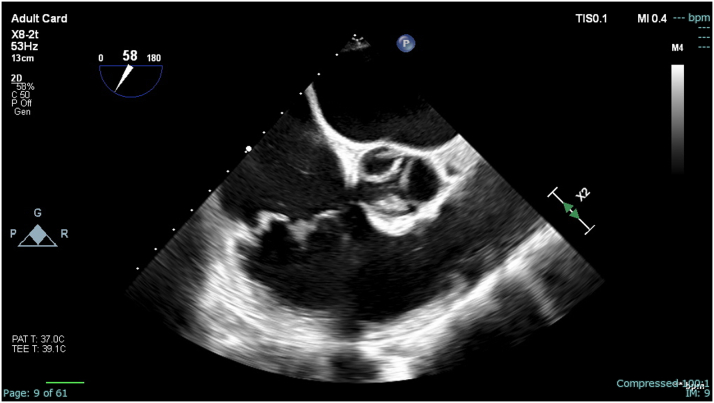 Figure 4
Figure 4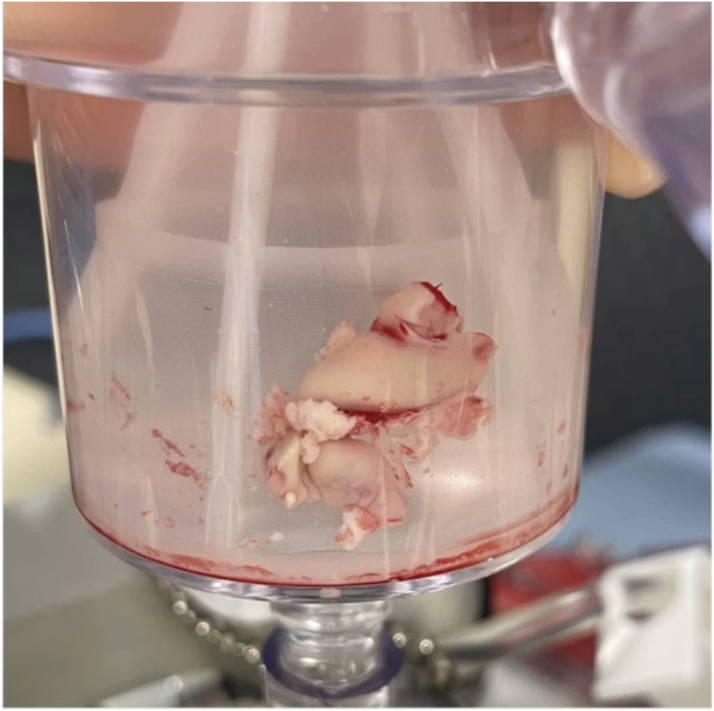 Figure 5
Figure 5 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Infectious Aortic and Vascular Conditions · Orthopedic Infections and Treatments
History of Presentation
A 55-year-old woman presented with 2 weeks of generalized weakness, subjective fevers, and progressively worsening neck and lower back pain. On presentation, she was afebrile and hemodynamically stable. Initial physical examination revealed a grade III/VI holosystolic murmur, worse on inspiration, loudest at the apex, and a gallop loudest at the left sternal border. Motor strength assessment revealed reduced 4/5 strength in the left upper and lower extremities.Take-Home Messages
- •Surgical intervention is considered for right-sided native valve IE with vegetations ≥20 mm, persistent bacteremia, recurrent pulmonary septic emboli, or highly resistant organisms.
- •The AngioVac system provides a minimally invasive treatment strategy for IE in patients who are otherwise ineligible for surgical intervention.
Past Medical History
The patient's past medical history was significant for morbid obesity (body mass index 42 kg/m^2^) and well-controlled asthma. On further questioning, she admitted to recent intravenous methamphetamine use.
Differential Diagnosis
Differential diagnosis based on initial presentation included infective endocarditis (IE) with associated epidural abscess or vertebral osteomyelitis, acute valvulopathy with associated musculoskeletal pain secondary to acute rheumatic fever, spinal cord infarction resulting from emboli secondary to IE, and carcinoid heart disease with metastasis to the spine.
Investigations
Initial investigative work-up with magnetic resonance imaging of the lumbar spine showed discitis and osteomyelitis at L3-L4 with abscesses in the left psoas muscle in addition to an epidural abscess at L1-L4. Further evaluation with transthoracic echocardiography revealed a large vegetation in the anterior leaflet of the tricuspid valve (TV) with mild-to-moderate tricuspid regurgitation (Figure 1).Figure 1. Large Vegetation (>3 cm) Present on the Tricuspid Valve on Midesophageal Right Ventricular Inflow-Outflow Preprocedural Transesophageal Echocardiography
Management (Medical/Interventions)
Concerning her lumbar spine osteomyelitis complicated by abscesses, the patient underwent urgent laminectomy, decompression, lumbar fusion, abscess drainage and was initiated on intravenous vancomycin. Blood cultures grew Enterococcus faecalis, and despite appropriate antibiotic therapy, both bacteremia and TV vegetation persisted for 8 days, prompting evaluation for surgical resection. She was transferred to a higher level of care for cardiothoracic surgery evaluation. However, given her elevated body mass index, poor level of function, and recent intravenous drug use, she was deemed not an appropriate surgical candidate.
Outcome and Follow-Up
Hospitalization was complicated by recurrent septic pulmonary emboli, which further prompted the need for percutaneous intervention. Therefore, the patient underwent aspiration of the large vegetation (>4 cm) using an AngioVac cannula (AngioDynamics, Inc), a percutaneous mechanical suction device, with residual approximately 1 cm vegetation seen on intraprocedural transesophageal echocardiography (Figures 2, 3, 4, and 5). During the procedure, both right and left common femoral veins (CFVs) were accessed via 8-F sheaths. A 26-F DrySeal Flex (W. L. Gore & Associates, Inc) sheath was then inserted via exchange in the right CFV through which the AngioVac suction catheter was introduced, advanced to the right atrium, and positioned over the TV vegetation via transesophageal echocardiography guidance. The circuit was then connected to an extracorporeal tubing system, which allowed for blood filtering before its reinfusion through the left CFV. After several suctioning attempts, the majority of the TV vegetation was successfully evacuated without complications. She remained hemodynamically stable during the procedure. The hospital course was uneventful thereafter, and she was discharged to a skilled nursing facility to complete intravenous antibiotic therapy.Figure 2. Midesophageal Right Ventricular Inflow-Outflow View During Procedural Transesophageal EchocardiographyThrombectomy catheter is engaged with thrombus midaspiration.Figure 3. Residual Vegetation (approximately 1 cm) Present on the Tricuspid Valve on MidEsophageal Right Ventricular Inflow-Outflow Post-ThrombectomyFigure 4Large Vegetation (>4 cm) Extracted Using the AngioVac Cannula SystemFigure 5Large Vegetation (>4 cm) Shown on a Surgical Specimen Tray
Discussion
Current evidence supports surgical management strategies for IE when there is right heart failure due to severe tricuspid regurgitation, recurrent septic pulmonary emboli, persistent bacteremia, and large TV vegetations (≥20 mm).1^,^2 Surgical debridement with cardiopulmonary bypass is considered a primary treatment approach for right-sided IE where source control is required.3 However, patient candidacy restrictions constitute a major barrier to care for an otherwise fatal disease process if inadequately treated.1, 2, 3 This case highlights the viability of AngioVac vegetectomy as an efficacious alternative treatment modality for persistent IE despite appropriate antimicrobial therapy in a poor surgical candidate. Further research should be conducted to characterize the role, safety, and efficacy of percutaneous intervention in IE.
Conclusions
AngioVac-assisted vegetation debulking is a viable therapeutic strategy for treatment-refractory right-sided IE in patients with elevated perioperative risk.2^,^4Visual SummaryTimeline of the CaseTimelineEventsDay 1A 55-year-old woman presented with 2 wk of generalized weakness, subjective fevers, and progressively worsening neck and lower back pain.Magnetic resonance imaging of lumbar spine showed discitis and osteomyelitis at L3-L4 with abscesses in the left psoas muscle in addition to an epidural abscess at L1-L4.She was started on intravenous vancomycin, and spine surgery service was consulted for surgical evaluation.Day 2She underwent urgent laminectomy, decompression, lumbar fusion, and abscess drainage.Further evaluation with transthoracic echocardiography revealed a large vegetation in the anterior leaflet of the tricuspid valve with mild-to-moderate tricuspid regurgitation.Infectious disease and cardiology services were consulted.Day 3Blood cultures grew Enterococcus faecalis, susceptible to vancomycin.Day 9Multiple repeat blood cultures were persistently positive for E. faecalis, susceptible to vancomycin.Given persistent tachycardia, hypoxia, transient hemodynamic instability, chest pain, and shortness of breath, computed tomography angiography of the chest was obtained, which revealed a right lower lobe pulmonary embolism.Bilateral lower extremity venous Doppler ultrasound revealed deep venous thrombosis in the bilateral popliteal veins.She was started on therapeutic enoxaparin.Repeat transthoracic echocardiography was performed, showing no change in tricuspid valve vegetation.Day 11Transferred to a higher level of care for evaluation with cardiothoracic surgery service.Given her elevated body mass index, poor level of function/mobility, and recent intravenous drug use, she was deemed a poor candidate for open heart surgery.The cardiology service discussed proceeding with percutaneous aspiration as an alternative source control strategy.Day 12POD 0Successful percutaneous aspiration of the large vegetation (>4 cm) was achieved using an AngioVac cannula with residual approximately 1 cm vegetation seen on intraprocedural transesophageal echocardiography (Figures 3, 4, and 5).POD 9Subsequent hospital course was uneventful.Patient was discharged to a skilled nursing facility to complete intravenous antibiotic therapy.
Funding Support and Author Disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Baddour L.M.Wilson W.R.Bayer A.S.Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications: a scientific statement for healthcare professionals from the American Heart Association[published correction appears in circulation]Circulation 1321520151435148610.1161/CIR.000000000000029626373316 · doi ↗ · pubmed ↗
- 2Abubakar H.Rashed A.Subahi A.Yassin A.S.Shokr M.Elder M.Angio Vac system used for vegetation debulking in a patient with tricuspid valve endocarditis: a case report and review of the literature Case Rep Cardiol 20172017192350510.1155/2017/1923505 PMC 569712229238620 · doi ↗ · pubmed ↗
- 3Pettersson G.B.Coselli J.S.Hussain S.T.The American Association for Thoracic Surgery (AATS) consensus guidelines: surgical treatment of infective endocarditis: executive summary J Thorac Cardiovasc Surg 153201712411258.e 2910.1016/j.jtcvs.2016.09.06828365016 · doi ↗ · pubmed ↗
- 4Mhanna M.El Sabbagh A.Al-Khadra Y.Angio Vac for vegetation debulking in right-sided infective endocarditis: a systematic review and meta-analysis J Card Surg 3720224489450010.1016/j.cpcardiol.2022.10135335961428 · doi ↗ · pubmed ↗