Delayed Retrieval of a Patent Foramen Ovale Occluder From the Abdominal Aorta: Management and Challenges
Ruxandra I. Sava, Fabien Doguet, Isabelle Danjon, Igor Platonov, Dominique Fourchy, Davy Huel, Noémie Tence, Eric Durand, Hélène Eltchaninoff, Philippe Garot

TL;DR
A rare case of a heart device moving to the aorta is successfully retrieved, but it caused aortic injury, highlighting the need for careful device sizing.
Contribution
Highlights management strategies and challenges in delayed retrieval of embolized PFO occluders.
Findings
Device embolization into the abdominal aorta occurred 6 months post PFO closure.
Percutaneous retrieval led to type B aortic dissection, managed conservatively.
Use of a larger sheath is recommended for endovascular retrieval to reduce risks.
Abstract
Patent foramen ovale (PFO) closure is an established strategy to prevent recurrent stroke from paradoxical embolism. Occluder embolization is a rare but serious complication. A 55-year-old man presented with abdominal discomfort 6 months post PFO closure. Transthoracic echocardiography failed to visualize the occluder, and a computed tomography scan revealed device embolization into the abdominal aorta. The patient underwent percutaneous retrieval of the device coupled with repeat PFO closure. Although the procedure was technically successful, he developed type B aortic dissection, which was successfully managed conservatively. Delayed retrieval of a PFO occluder embolized into the aorta is associated with significant risk of aortic injury, regardless of endovascular or surgical approach. Adequate PFO sizing is critical to prevent device embolization. When endovascular retrieval is…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
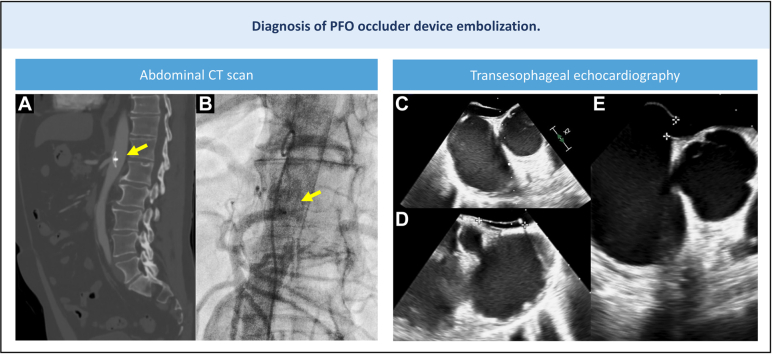 Figure 1
Figure 1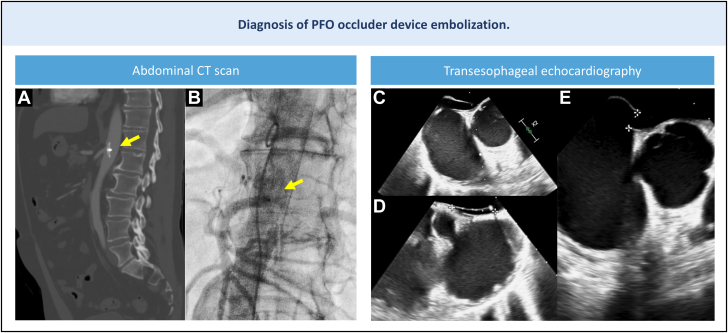 Figure 2
Figure 2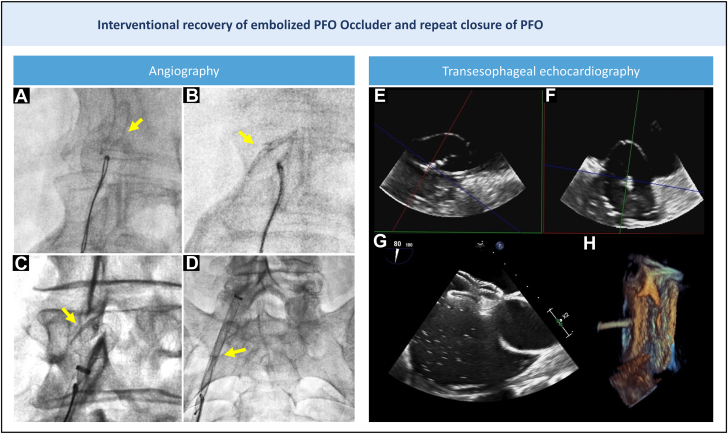 Figure 3
Figure 3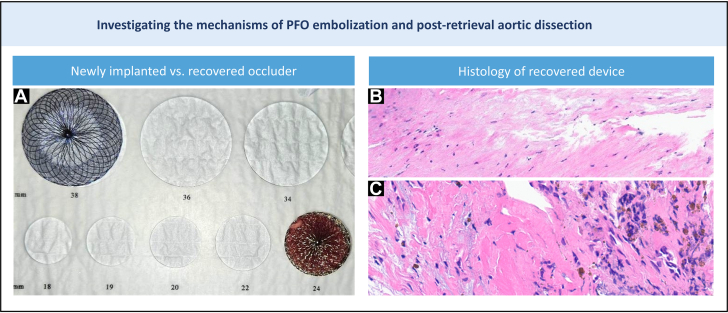 Figure 4
Figure 4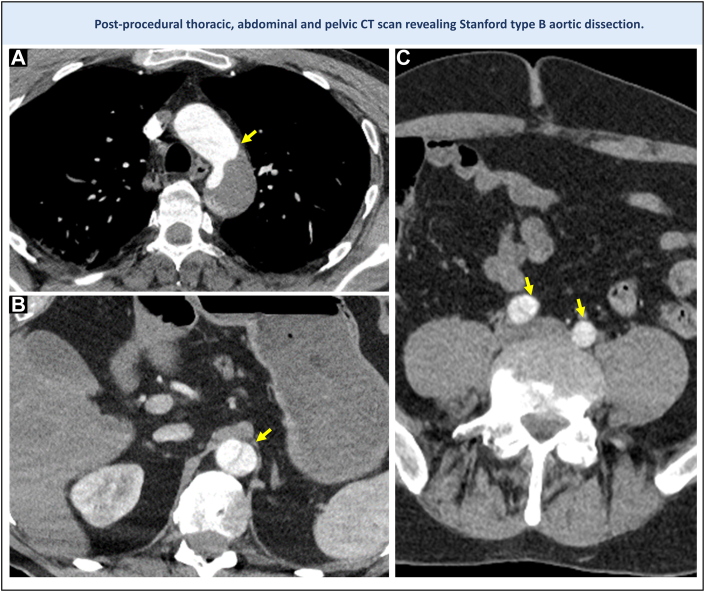 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular and Diving-Related Complications · Aortic aneurysm repair treatments · Cardiovascular Conditions and Treatments
History of Presentation
A 55-year-old man was referred to our center for percutaneous retrieval of a patent foramen ovale (PFO) occluder that embolized into the abdominal aorta. An Occlutech device with a 23-mm left atrial disk and a 25-mm right atrial disk had been implanted without complication. The device was confirmed in place on transthoracic echocardiography 24 hours post procedure; however, at the sixth month of follow-up, the device was no longer visualized, and a significant interatrial shunt was noted. The patient reported vague abdominal discomfort. A thoracoabdominal-pelvic computed tomography (CT) identified the occluder lodged at the level of the celiac trunk, between the T12 and L1 vertebrae (Figures 1A and 1B). Given the patient's symptoms and thrombotic risk, and considering the challenges of surgery, the heart team elected to proceed with percutaneous retrieval.Figure 1. Non-invasive Imaging Demonstrating PFO Occluder Embolization(A and B) PFO device embolized into the abdominal aorta, depicted on CT scan and angiography (arrows). (C to E) TEE showing a large PFO. CT = computed tomography; PFO = patent foramen ovale; TEE = transesophageal echocardiography.
Past Medical History
The patient had a body mass index of 26 kg/m^2^. He had experienced a lateral medullary stroke in July 2023. Apart from a significant PFO with right-to-left shunt, the diagnostic workup was unremarkable. A family history of aortic dissection in the patient's brother was noted.
Differential Diagnosis
The patient's bowel function was normal, and physical examination was unremarkable. Abdominal CT showed no alternative cause for the abdominal discomfort aside from the occluder, which was located near the mesenteric artery and may have been causing transient mesenteric ischemia.
Investigations
The electrocardiogram on admission showed sinus rhythm, without conduction or repolarization abnormalities.
The transthoracic echocardiography demonstrated a hypermobile interatrial septum with severe right-to-left shunting. Left ventricular function and dimensions were normal, as well as valvular function. The aortic valve was tricuspid, and the ascending aorta was mildly dilated at 42 mm.
The transesophageal echocardiogram (Figures 1C to 1E) showed a large PFO (Video 1), with a PFO tunnel length of 20 mm, width of 15 mm, and septal excursion of 16 mm. A bubble study revealed a grade 4 atrial shunt.
Management (Medical/Interventions)
A right femoral arterial approach was used. A 28-mm long, 14-F Sentrant sheath (Medtronic) was positioned in the proximal right iliac artery. Initial attempts to mobilize the device using a pigtail catheter were unsuccessful. A 25-mm Amplatz Goose Neck snare (Medtronic) also failed to secure the device. A Tulip snare (En Snare, Merit Medical) introduced via a 6-F Judkins right catheter finally succeeded in anchoring the occluder. With steady traction applied to the snare-catheter unit, the prosthesis was mobilized (Figures 2A and 2B, Video 2). Hemodynamics remained stable under conscious sedation, and angiography showed no evidence of aortic injury (Video 3). The occluder was safely withdrawn into the sheath and fully externalized (Figures 2C and 2D, Videos 4 and 5).Figure 2. Angiography and TEE Guidance for Embolized Occlude Recovery and Repeat PFO Closure(A to D) Device (arrows) mobilization and retraction into a 14-F sheath by snaring with a tulip snare inside a Judkins right 6-F catheter. (E and F) A stretched diameter of 22 mm was measured by balloon sizing. (G) Complete abolition of right-left shunt as demonstrated by bubble testing. (H) Three-dimensional TEE showing adequate device positioning. PFO = patent foramen ovale; TEE = transesophageal echocardiography.
A repeat PFO closure was then performed. Transesophageal echocardiogram showed a large PFO (Figures 1C to 1E). Balloon sizing (Figures 2E and 2F) revealed a stretched diameter of 22 mm, prompting the selection of a 24-mm Septal Occluder (Abbott), a device typically used for atrial septal defect closure. This was significantly larger than the initial Occlutech Occluder (Figure 3A). The new device showed excellent apposition, and postdeployment bubble testing was negative (Figures 2G and 2H, Video 6).Figure 3. Mechanistic Insights into PFO Occluder Embolization and Aortic Dissection Following Endovascular Retrieval(A) We chose a 24-mm septal occluder ASD-type device (top left corner) for repeat PFO closure, which is much larger than the prior implanted 23 × 25 mm Occlutech PFO Occluder (bottom right corner). (B) H-E stain showing intimal growth on prosthesis. (C) Foreign-body granuloma. ASD = atrial septal defect; H-E = hematoxylin and eosin; PFO = patent foramen ovale.
Outcome and Follow-Up
Four hours after the procedure, the patient developed lower abdominal pain radiating to the chest. CT imaging revealed a type B aortic dissection (Figure 4), extending proximally from the abdominal aorta to the distal thoracic aorta, and distally to the common iliac arteries. In the absence of signs of ischemia, he was managed conservatively. A repeat scan at 1 week showed no progression, and he was discharged on day 10.Figure 4. Computed Tomography Revealing a Serious Complication of Endovascular Occluder Recovery(A) Abdominal computed tomography demonstrating a dissection flap (arrow) at the level of the aortic arch, distal to the subclavian artery. (B) Aortic dissection originating at the site of occluder embolization (arrow). (C) Aortic dissection extending distally to both iliac arteries (arrows). PFO = patent foramen ovale.
Histological examination of the explanted occluder revealed endothelialized fibrous tissue resembling neointima and a granulomatous foreign body reaction (Figures 3B and 3C), but no myocardial elements. These findings suggest the occluder had adhered firmly to the aortic wall, likely having embolized shortly after the initial procedure.
One year later, the patient remained clinically stable. He experienced an episode of symptomatic paroxysmal atrial fibrillation within the first month, successfully managed by bisoprolol (5 mg daily) and a non–vitamin K oral anticoagulant. No arrhythmia was detected on 24-hour electrocardiogram monitoring at 12 months.
Discussion
This case demonstrates that delayed retrieval of an embolized PFO device from the abdominal aorta is feasible but carries substantial risk of aortic injury.
Device embolization is uncommon, with a reported incidence between 0.6% and 1.2%.1 Recognized risk factors include long PFO tunnel length and atrial septal aneurism.1^,^2 A literature search on PubMed using the query [(patent foramen ovale) AND ((prosthesis) OR (occluder) OR (device)) AND ((embolization) OR (dislodge∗) OR (migrat∗))] identified 14 individual case reports and one case series describing PFO device embolization events.
Timing appears critical: PFO occluder embolization discovered shortly after implantation can often be safely managed percutaneously,1^,^3, 4, 5, 6 whereas delayed retrieval may carry a higher risk of aortic injury. This is illustrated both by our case and by a report by Berk TA et al,7 where surgical extraction was similarly complicated by aortic dissection. This is likely due to the development of adhesions between the migrated device and the aortic wall, as demonstrated by our histological study. Additional contributing factors may include subclinical aortopathy, suggested by the mildly dilated ascending aorta and a family history of dissection.
Several reports have described failed attempts to retrieve embolized devices through short sheaths ending in the femoral artery, necessitating surgical cutdown.2^,^4 Davies et al2 described a case where an embolized Amplazer Cribrifrom Septal Occluder could not be retrieved past the iliac bifurcation using a short 20-F sheath and ultimately required surgical removal, complicated by distal embolization. In contrast, our use of a long 14-F sheath facilitated capture within a large-caliber vascular segment, allowing complete percutaneous retrieval.
Multiple reports1^,^3^,^5^,^6^,^8 have highlighted the advantages of using long sheaths, even more so than larger diameters, in reducing both procedural difficulty and risk of vascular trauma. Our 14-F sheath was 5-F larger than the original 9-F sheath, consistent with prior recommendations to use retrieval sheaths 2-F larger.9
In rare cases, conservative management may be a valid alternative. One patient with device embolization detected 12 months post implant remained asymptomatic at 24 months under dual antiplatelet therapy.8
Given the lack of randomized data and the rarity of this complication, the decision to pursue percutaneous, surgical, or conservative treatment should be individualized and guided by a multidisciplinary heart team discussion, with detailed patient counseling being essential.
Conclusions
Endovascular retrieval of a PFO occluder embolized to the abdominal aorta is feasible and can be accomplished using a long sheath 2- to 5-F sizes larger than the original delivery sheath. However, delayed retrieval increases the risk of aortic injury due to device adherence to the vessel wall. Careful sizing, recognition of anatomical risk factors, and early postprocedural imaging may help prevent and detect this complication early on, avoiding the risks associated with delayed recovery.
Funding Support and Author Disclosures
Dr Garot received proctor/consultant fees from Abbott, Boston Scientific, and Edwards Lifesciences. Mr Huel is an employee of Abbott Cardiovascular, France. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.Take-Home Messages
- •Aneurysmal interatrial septum and long patent foramen ovale tunnels are risk factors for patent foramen ovale occluder device embolization.
- •Early follow-up imaging may help identify silent device migration before the development of adhesions between the embolized device and the vessel walls.
- •When endovascular retrieval is necessary, a long sheath 2- to 5-F larger than the original delivery system is recommended to minimize procedural risk.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Goel S.S.Aksoy O.Tuzcu E.M.Krasuski R.A.Kapadia S.R.Embolization of patent foramen ovale closure devices Tex Heart Inst J 404201343944424082375 PMC 3783141 · pubmed ↗
- 2Davies A.J.Collins N.Organ N.Retrieval of embolized amplatzer patent foramen ovale occlusion device: issues related to late recognition Case Rep Cardiol 20172017989421510.1155/2017/9894215 PMC 543924528567311 · doi ↗ · pubmed ↗
- 3Crawford D.A.Naidu S.G.Shah A.A.Davila V.J.Stone W.M.Endovascular retrieval of an embolized atrial septal occluder device from the abdominal aorta Vasc Endovascular Surg 528201866967310.1177/153857441879039330058451 · doi ↗ · pubmed ↗
- 4Aubry P.C.Juliard J.M.Brochet E.Early systemic device embolization after transcatheter patent foramen ovale closure J Invasive Cardiol 1832006 E 111E 11316495605 · pubmed ↗
- 5Yıldırır A.Varan B.Erdoğan I.Boyvat F.Case images: percutaneous retrieval of an embolized occluder device from the aorta using a goose-neck snare Turk Kardiyol Dern Ars 404201239310.5543/tkda.2012.0197922951862 · doi ↗ · pubmed ↗
- 6Khosravi A.Mirdamadi A.Movahed M.R.Successful retrieval of embolized atrial septal defect occluder and patent foramen ovale closure device using novel coronary wire trap technique Catheter Cardiovasc Interv 921201818919210.1002/ccd.2695528603930 · doi ↗ · pubmed ↗
- 7Berk T.A.Kroeze S.Suttorp M.J.Heijmen R.H.Open surgical retrieval of a migrated patent foramen ovale closure device from the descending aorta following failed percutaneous retrieval from the aortic arch: a case report with a word of caution Eur Heart J Case Rep 732023 ytad 09910.1093/ehjcr/ytad 099PMC 1001217636926264 · doi ↗ · pubmed ↗
- 8Basoor A.S.Cotant J.F.Halabi A.R.De Gregorio M.Chughtai H.Patel K.C.Minimally invasive retrieval of patent foramen ovale closure device after device migration to the descending aorta Tex Heart Inst J 394201258258422949785 PMC 3423282 · pubmed ↗