A Case of Factor XIII Deficiency Identified by Recurrent Postoperative Bleeding After Tonsillectomy
Takanobu Teramura, Akihiro Sakai, Masashi Hamada, Koichiro Wasano, Ai Yamamoto, Hikaru Yamamoto, Kenji Okami

TL;DR
A rare case of Factor XIII deficiency was identified in a patient who experienced repeated bleeding after tonsillectomy despite normal blood tests.
Contribution
Highlights Factor XIII deficiency as a potential cause of postoperative bleeding when routine coagulation tests are normal.
Findings
A 27-year-old man with normal coagulation tests had recurrent postoperative bleeding after tonsillectomy.
Factor XIII activity was found to be reduced at 36%, confirming a deficiency.
Bleeding stopped after administration of Factor XIII concentrate, stabilizing the patient's recovery.
Abstract
Postoperative bleeding is a well‐known complication of tonsillectomy. Although inadequate hemostasis and vascular injury are common causes, occult coagulation disorders may also contribute. Factor XIII deficiency is an extremely rare condition that is particularly difficult to detect preoperatively because PT and APTT typically remain normal. A 27‐year‐old man underwent bilateral tonsillectomy for a recurrent peritonsillar abscess. Despite normal coagulation screening, the patient developed repeated postoperative hemorrhages requiring surgical management. Further evaluation revealed reduced Factor XIII activity (36%). After Factor XIII concentrate administration, bleeding ceased, and the postoperative course stabilized. Factor XIII deficiency should be considered in patients with recurrent postoperative bleeding despite normal routine coagulation tests. Early recognition and timely…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
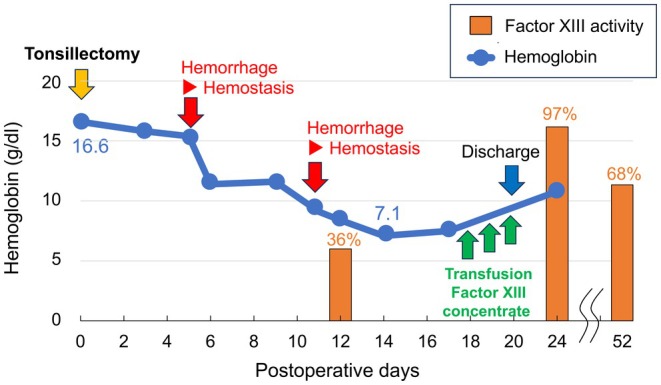 FIGURE 1
FIGURE 1| Test | Result |
|---|---|
| Hematology | |
| WBC | 7000/μL |
| RBC | 5.37 × 106/μL |
| Hb | 16.6 g/dL |
| PLT | 260 × 103/μL |
| Biochemistry | |
| AST | 20 U/L |
| ALT | 33 U/L |
| BUN | 12 mg/dL |
| Cre | 0.7 mg/dL |
| Glu | 106 mg/dL |
| Coagulation tests | |
| APTT | 33 s |
| PT | 11.1 s |
| PT‐INR | 0.97 |
| Test | Result | Reference range |
|---|---|---|
| APTT | 35 s | (25–36 s) |
| PT | 14.2 s | (9.3–13.8 s) |
| PT‐INR | 1.2 | (0.8–1.10) |
| Blood Coagulation Factor VII Activity | 66% | (75%–140%) |
| Blood Coagulation Factor VIII Activity | 67% | (60%–150%) |
| Blood Coagulation Factor IX Activity | 81% | (70%–130%) |
| von Willebrand Factor (vWF) Activity | 103% | (60%–170%) |
| Blood Coagulation Factor XIII Activity | 36% | (70%–140%) |
| Blood Coagulation Factor XIII Antigen | 50% | (> 70%) |
| Total PAI‐1 | 41 ng/mL | (< 50%) |
| Protein C Activity | 151% | (64%–146%) |
| Protein S Activity | 94% | (67%–164%) |
| Protein S Antigen | 92% | (73%–137%) |
| D‐dimer | 0.5 μg/mL | (< 1.0) |
| Fibrin Degradation Products (FDP) | < 2.5 μg/mL | (< 5.0) |
| Diagnostic category | Criteria |
|---|---|
| Possible | Consider AHFXIII/13 if all the following conditions are met: |
| (1) Recent onset of bleeding symptoms mainly in the older adult. | |
| (2) No family history of congenital/inherited deficiency of FXIII or other coagulation factors. | |
| (3) Lack of previous bleeding symptoms especially in association with previous hemostatic challenges (e.g., surgery, invasive tests, trauma, etc.) | |
| (4) Not explained by excessive medication such as anticoagulants and antiplatelet drugs. | |
| (5) Abnormality of FXIII parameter(s) on laboratory testing (FXIII activity and/or antigen < 50%) | |
| Probable | In addition to criteria (1) to (5) above: |
| (6) Presence of FXIII inhibitors* (positive by cross‐mixing tests between patient's and healthy control's plasma using standard functional tests after 2 h incubation at 37°C) | |
| Definite | In addition to criteria (1) to (5) above: |
| (7) Presence of anti‐FXIII autoantibodies (positive by immunological methods) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBlood properties and coagulation · Parathyroid Disorders and Treatments · Hemostasis and retained surgical items
Introduction
1
Postoperative bleeding is a common complication of tonsillectomy. The primary causes include inadequate intraoperative hemostasis or vascular injury, and postoperative vascular damage resulting from scab detachment or infection. However, cases in which postoperative hemorrhage led to the diagnosis of underlying coagulation disorders, such as hemophilia, have been reported [1, 2]. In such conditions, the activated partial thromboplastin time (APTT) is typically prolonged, allowing for the detection of these abnormalities during routine preoperative coagulation screening. When coagulation abnormalities are identified, appropriate factor replacement therapy can be administered before surgery to reduce the risk of bleeding. However, XIII coagulation factor deficiency is critical for final stages of the coagulation cascade and has been reported to cause no abnormalities in prothrombin time (PT) or APTT [3]. Congenital Factor XIII deficiency is a rare genetic bleeding disorder. In the United States, its incidence is estimated to be approximately 1 in 3–5 million live births. By contrast, acquired Factor XIII deficiency is uncommon and may result from autoimmune mechanisms or increased consumption associated with surgery, trauma, or systemic diseases. Because routine coagulation tests remain normal in both forms, the true prevalence is likely to be underestimated.
Here, we describe a case of recurrent postoperative bleeding after tonsillectomy that required hemostasis under general anesthesia. Subsequent coagulation factor testing confirmed reduced Factor XIII levels. After administration of Factor XIII concentrate, no further bleeding occurred, and the patient experienced an uneventful recovery. Here, we present this case along with a review of the relevant literature.
Case History/Examination
2
A 27‐year‐old male patient presented with recurrent episodes of fever and a sore throat. The patient's medical and family histories were unremarkable. The patient had no history of bleeding, delayed wound healing, or hematoma formation. He was a nonsmoker and occasionally consumed alcohol. To date, no drug allergies have been reported.
The patient had experienced four episodes of peritonsillar abscess (PTA) over the past several years (at X‐9, X‐7, X‐6, and X years before presentation). The patient was referred to our department for palatine tonsillectomy due to recurrent PTA. Physical examination revealed that the palatine tonsils were enlarged (Friedman grade II). Preoperative laboratory assessments, including biochemical and coagulation tests, were within normal limits (Table 1).
Investigations and Treatment
3
Clinical Course
3.1
Bilateral tonsillectomy was performed on Y, Z, and X. Both palatine tonsils were excised extracapsular using bipolar cautery. Moderate pericapsular adhesions were observed, consistent with scarring from prior episodes of peritonsillar abscesses. The operative time was 25 min, with minimal intraoperative blood loss. The patient was discharged on postoperative day (POD) Z + 5 without immediate complications. However, on POD Z + 5, the patient experienced postoperative hemorrhage and was readmitted for hemostatic treatment under general anesthesia. On Z + 11, the patient presented with massive postoperative bleeding, necessitating a second hemostatic procedure under general anesthesia. Despite undergoing the usual surgery, the patient experienced multiple episodes of postoperative bleeding and poor granulation tissue formation at the wound site. These findings raised suspicion of an underlying coagulation disorder and prompted additional laboratory evaluations.
Coagulation Function Test
3.2
On POD Z + 12, coagulation tests revealed a 36% decrease in Factor XIII activity. PT was mildly prolonged, whereas APTT remained within normal limits. There was no decrease in the total plasminogen activator inhibitor‐1 (PAI‐1), protein C, or protein S activity, which are factors of the fibrinolytic system, or an increase in FDP or D‐dimer levels. Based on these results, Factor XIII deficiency was diagnosed (Table 2).
Outcome and Follow‐Up
4
Treatment Courses and Outcome
4.1
Following the second hemostatic intervention on POD Z + 12, the patient experienced no further bleeding episodes. Fibrogamin P (Factor XIII concentrate) was administered for 3 days from Z + 18 to Z + 20. The patient was subsequently discharged with Z + 20. At outpatient follow‐up, there were no recurrent bleeding events, and Factor XIII activity increased to 97% with Z + 24. Postoperative wounds showed normal mucosal healing. However, by Z + 52, the Factor XIII activity decreased to 68% in subsequent blood samples (Figure 1).
Postoperative course. Postoperative bleeding occurred on the 5th day after tonsillectomy and stopped under general anesthesia. Furthermore, on the 11th postoperative day, postoperative bleeding recurred, and hemostasis was performed under general anesthesia. Factor XIII activity measured on the 12th postoperative day was as low as 36%. Factor XIII blood transfusion was performed from the 18th to 20th postoperative days. Blood sampling on the 24th postoperative day showed that Factor XIII activity increased to 97%.
Discussion
5
Coagulation Factor XIII plays an important role in hemostasis and wound healing. It belongs to the transglutaminase family, a group of enzymes that crosslink proteins and function as fibrin‐stabilizing factors. Factor XIII circulates as an A2B2 heterotetramer comprising a catalytic A‐subunit dimer and a stabilizing B‐subunit dimer. During the final stage of the coagulation cascade, Factor XIII cross‐links fibrin strands, thereby strengthening and stabilizing the clot. Consequently, Factor XIII deficiency results in reduced clot stability and premature clot dissolution before adequate tissue repair, leading to persistent bleeding and delayed wound healing [4]. Because Factor XIII acts only at the terminal step of the coagulation pathway and is independent of the intrinsic and extrinsic pathway reactions, neither PT nor APTT is affected in cases of Factor XIII deficiency.
Factor XIII deficiency can be broadly classified into congenital and acquired forms. Congenital deficiency results from defects in either the A‐ or B‐subunit and is present at birth, although extremely rare. On the other hand, acquired Factor XIII deficiency is caused by anti‐factor XIII autoantibodies or inhibitors, or by increased consumption of Factor XIII in conditions such as surgery, trauma, malignancy, disseminated intravascular coagulation, sepsis, and liver failure [5, 6, 7]. In both congenital and acquired forms, routine coagulation parameters, including PT, APTT, platelet count, and platelet aggregation, are generally normal, making diagnosis challenging.
The diagnostic criteria for autoimmune Factor XIII deficiency (AHFXIII/13) are summarized in Table 3 [8]. In our case, the patient met criteria (1–5), fulfilling the definition of a possible diagnosis. However, as inhibitor and autoantibody testing were not performed, the diagnostic certainty could not be elevated beyond this level.
The mainstay treatment for Factor XIII deficiency is replacement therapy with highly purified plasma‐derived Factor XIII concentrates (e.g., Corifact/fibrogammin P) or recombinant Factor XIII‐A2 (catridecacog) [9]. In this case, 720 to 1440 units of Fibrogammin P were administered daily for 5 days according to the product guidelines. Although freshly frozen plasma (FFP) contains Factor XIII, its low concentration necessitates large infusion volumes, which increases the risk of volume overload. Therefore, concentrated preparations are preferred for replenishment.
In our patient, both the Factor XIII activity and antigen levels were reduced. Despite successful bleeding control following replacement therapy, Factor XIII activity remained low on follow‐up testing, suggesting possible acquired Factor XIII deficiency due to autoantibodies or inhibitors. In addition, substantial postoperative blood loss (totaling approximately 2300 mL) may have contributed to the increased consumption, further supporting a secondary acquired deficiency.
Associations between recurrent post‐tonsillectomy bleeding and reduced Factor XIII activity have been reported by Albahkaly et al. [3], Windfuhr et al. [10], Jankovic et al. [5], and Altamimi et al. [11]. Across these cases, patients required transfusions of Factor XIII concentrate, FFP, or red blood cells. The reported ages ranged from 4 to 40 years and the number of rebleeding episodes ranged from 2 to 7 years. Factor XIII activity at the time of bleeding ranges from 7% to 58%. Notably, the case described by Albahkaly et al. involved a 4‐year‐old girl who died.
Most of the affected patients demonstrated normal preoperative coagulation profiles [5, 10, 11]. For individuals with a personal or family history suggestive of a bleeding disorder, or when the family history is unknown, preoperative evaluation of specific coagulation factors may be warranted [11]. In addition, clinicians should consider Factor XIII deficiency when postoperative bleeding recurs despite normal coagulation screening, particularly when bleeding is delayed or wound healing is impaired. This suspicion is especially important in adults with no history of bleeding because acquired Factor XIII deficiency often presents for the first time after surgery or trauma. When preoperative Factor XIII activity is < 60%, prophylactic supplementation is recommended to reduce surgical bleeding risk [12].
The long‐term management of congenital Factor XIII deficiency requires regular prophylactic replacement therapy, which significantly reduces the risk of life‐threatening bleeding, including intracranial hemorrhage. In contrast, acquired Factor XIII deficiency has a highly variable prognosis, depending on the underlying cause. Autoimmune forms are associated with high morbidity and mortality and often require immunosuppressive therapy in addition to factor replacement. Because Factor XIII activity may fluctuate over time, periodic monitoring is recommended, even after apparent stabilization [9].
In the present case, reduced Factor XIII activity was identified only after repeated postoperative hemorrhage and was successfully corrected with supplementation. In patients with persistent or recurrent postoperative bleeding, additional evaluation of the coagulation–fibrinolytic system, including Factor XIII activity, anti‐factor XIII antibodies, Factor XIII inhibitors, FDP, and D‐dimer levels, should be performed. On the basis of these findings, timely supplementation should be considered to prevent further complications.
Conclusion
6
In summary, we reported a case of reduced Factor XIII activity in a patient who developed multiple episodes of postoperative hemorrhage after tonsillectomy. Following Factor XIII replacement therapy, the patient had an uneventful course with no further bleeding. This case highlights the possibility that coagulation disorders that are undetectable on routine preoperative screening may still be present. Therefore, when patients experience recurrent postoperative bleeding or repeated complications, it is clinically important to perform additional diagnostic evaluations to identify the potential underlying coagulation abnormalities.
In particular, clinicians should consider evaluating Factor XIII activity when postoperative bleeding recurs despite normal PT and APTT, when bleeding is delayed during the postoperative course, or when wound healing is impaired. Early recognition of Factor XIII deficiency and timely administration of replacement therapy can prevent severe complications and should be incorporated into the differential diagnosis of unexplained postoperative hemorrhage in otolaryngological practice.
Limitation
7
This study has several limitations. First, because inhibitor assays and anti‐factor XIII autoantibody tests were not performed, we were unable to determine whether the reduced Factor XIII activity represented a congenital deficiency, an acquired form, such as autoimmune Factor XIII deficiency, or consumption secondary to surgery. Second, this study describes a single case, which limits the generalizability of the findings. Larger case series and systematic evaluations are required to clarify the clinical characteristics, diagnostic approaches, and optimal management of postoperative bleeding associated with Factor XIII deficiency.
Author Contributions
Takanobu Teramura: conceptualization, investigation, methodology, writing – original draft, writing – review and editing. Akihiro Sakai: investigation, supervision, writing – review and editing. Masashi Hamada: investigation, methodology. Koichiro Wasano: investigation, methodology. Ai Yamamoto: investigation. Hikaru Yamamoto: supervision. Kenji Okami: supervision.
Funding
The authors have nothing to report.
Ethics Statement
All protected health information was withheld from this piece to ensure patient anonymity.
Consent
We have obtained written informed consent from the participant presented in this report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A. Randhawa , D. Bondin , and B. N. Kumar , “A Surgical Presentation for Haemophilia A,” BML Case Reports 2014 (2014): bcr 2014203687, 10.1136/bcr-2014-203687.PMC 406963124939452 · doi ↗ · pubmed ↗
- 2Y. Saikawa , A. Tsunoda , N. Sata , and T. Anzai , “An Incidental Latent Adult Hemophilia Case Found After a Tonsillectomy,” SAGE Open Medical Case Reports 9 (2021): 1–3, 10.1177/2050313 X 20988410.PMC 792400533717485 · doi ↗ · pubmed ↗
- 3S. Albahkaly , A. Alkhunaizi , and F. Makki , “Post‐Tonsillectomy Hemorrhage due to Factor XIII Deficiency,” Egyptian Journal of Otolaryngology 28 (2012): 278–280, 10.7123/01.EJO.0000418068.19559.fa. · doi ↗
- 4C. Kleber , “The Impact of Acquired Coagulation Factor XIII Deficiency on Traumatic Bleeding and Wound Healing,” Critical Care 26 (2022): 69, 10.1186/s 13054-022-03940-2.35331308 PMC 8943792 · doi ↗ · pubmed ↗
- 5M. Jankovic , “Massive Recurrent Post‐Tonsillectomy Bleedings Revealing a Transient Factor XIII Deficiency in a 10‐Year‐Old Boy. A Case Report,” International Journal of Pediatrics and Adolescent Medicine 6 (2019): 55e 57, 10.1016/j.ijpam.2019.05.006.31388547 PMC 6676365 · doi ↗ · pubmed ↗
- 6V. Schroeder , “New Developments in the Area of Factor XIII,” Journal of Thrombosis and Haemostasis 11 (2013): 234–244, 10.1111/jth.12074.23279671 · doi ↗ · pubmed ↗
- 7J. H. Levy and C. S. Greenberg , “Biology of Factor XIII and Clinical Manifestations of Factor XIII Deficiency,” Transfusion 53 (2013): 3865, 10.1111/j.1537-2995.2012.03865.x.22928875 · doi ↗ · pubmed ↗
- 8A. Ichinose , H. P. Kohler , H. Philippou , et al., “Recommendation for ISTH/SSC Criterion 2015 for Autoimmune Acquired Factor XIII/13 Deficiency,” Thrombosis and Haemostasis 116, no. 2016 (2016): 772–774, 10.1160/TH 16-05-0362.27439329 · doi ↗ · pubmed ↗