Incidence and impact of urogenital sequelae in women following pelvic-ring injuries: a retrospective cohort study
Chin-Chieh Hsu, Chih-Yang Lai, I-Jung Chen, Yung-Heng Hsu, Ying-Chao Chou, Tsia-Shu Lo, Yi-Hsun Yu

TL;DR
This study finds that many women experience urinary issues after pelvic injuries, with more severe injuries linked to worse outcomes.
Contribution
The study provides new insights into the incidence and risk factors for urinary dysfunction after pelvic-ring injuries in women.
Findings
Nearly half of patients reported urinary symptoms one month post-surgery.
Greater injury severity was independently associated with urinary dysfunction at six months.
Urinary symptoms improved significantly over 12 months postoperatively.
Abstract
Pelvic-ring injuries in women often result in urinary dysfunction owing to the proximity of pelvic organs to the urinary tract, significantly affecting quality of life. However, detailed research on urinary sequelae remains limited. This study aimed to assess the incidence of urinary dysfunction in women after pelvic-ring injuries and to identify risk factors influencing urinary function. We conducted a retrospective cohort study of women who underwent osteosynthesis for pelvic-ring injuries between January 2022 and June 2023 with ≥ 12 months of follow-up. Urinary dysfunction was evaluated using the Questionnaire for Urinary Incontinence Diagnosis and Female Urinary Symptom Score at one, three, six and 12 months postoperatively. Fifty-eight patients (mean age, 43.2 years) were included, with motor-vehicle collisions being the most common cause for pelvic-ring injuries (74.1%). Most…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
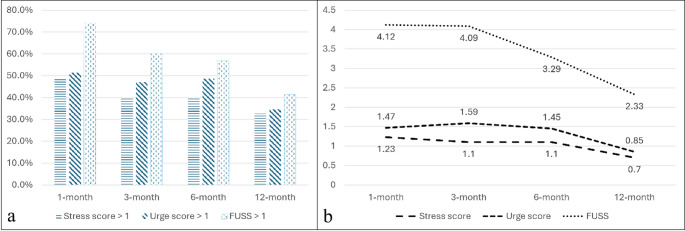 Figure 1
Figure 1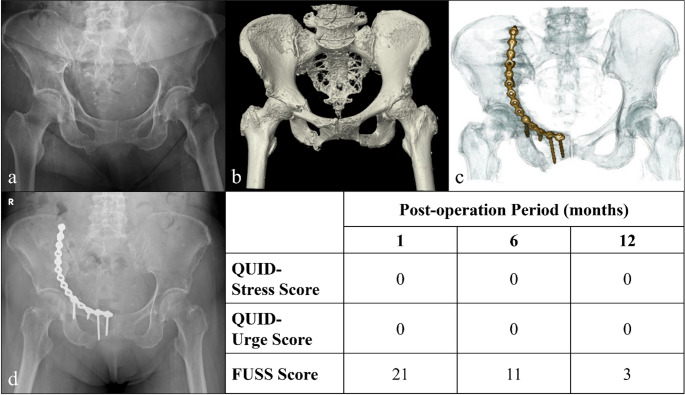 Figure 2
Figure 2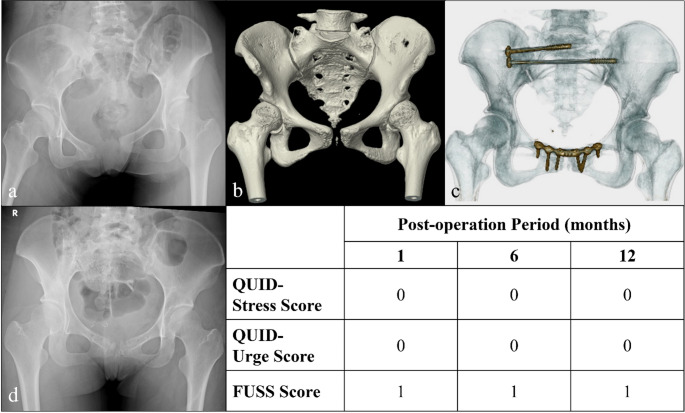 Figure 3
Figure 3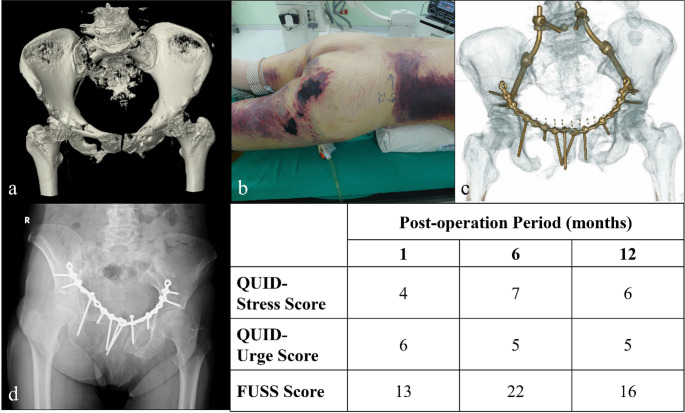 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPelvic and Acetabular Injuries · Ureteral procedures and complications · Pelvic floor disorders treatments
Introduction
The complexity of injury mechanisms in pelvic ring injuries (PRIs) can lead to intricate fracture patterns, necessitating thorough resuscitation before reconstruction [1–3]. However, associated injuries around the pelvic ring can delay rehabilitation owing to the primary injury and related injury or treatment complications [4–7]. In women, the proximity of pelvic organs to the urinary tract causes a heightened risk for urological complications [4, 7, 8].
The abdominal wall and pelvic floor musculature is integral to maintaining urinary continence by providing structural support to the bladder and urethra and facilitating controlled voiding through coordinated contraction and relaxation [9, 10]. Pelvic-ring symmetry and structural integrity are critical for the optimal function of the pelvic floor and associated urogenital systems [10–12]. PRIs may lead to disruption of pelvic-ring continuity, neural compromise, or vascular injury, which can manifest as urinary dysfunction, including incontinence or retention [4]. Moreover, interventions performed during PRI resuscitation and reconstruction phases may contribute to urinary function impairment [13–15].
The impact on urinary sequelae in women post-PRIs is significant, even without urogenital organ traumatic injuries [4, 8]. Urinary sequelae, including bladder dysfunction, urinary incontinence, and recurrent infections, are common yet under-recognised complications of pelvic-ring fractures. These issues can significantly affect a woman’s quality of life and may require extensive urological management during and after recovery [4, 8, 16]. Despite their frequency and impact, detailed studies on urinary consequences in women post-pelvic trauma remain scarce. This study aimed to determine urinary dysfunction incidence in women post-PRIs and identify potential risk factors for damaged urinary function.
Materials and methods
Study design
This is a retrospective cohort analysis of women who underwent osteosynthesis for PRIs at a single medical institute from January 2022 to June 2023. Eligible participants were identified through a review of medical records and included adult women (aged ≥ 18 years) with documented PRIs treated surgically and followed up for at least 12 months. Patients with traumatic urogenital organ injuries, pre-existing urinary conditions, or incomplete follow-up records were excluded.
Demographic data collection
Data were collected from electronic medical records and images, including demographic information (age and comorbidities), injury characteristics (fracture type and mechanism of PRI, Injury Severity Score [ISS], and New Injury Severity Score [NISS]), types of haemostatic procedure (unilateral or bilateral arterial embolisation [AE]), surgical details (type of osteosynthesis, approach, and any additional procedures), and imaging outcomes.
Applied PRI classification
Two classification systems were applied for categorising PRIs. The Young and Burgess classification system classifies PRIs based on the direction of the injury force, which leads to specific patterns of pelvic-ring deformity [17]. It includes lateral compression (LC) types I to III, anteroposterior (AP) compression (APC) types I to III, vertical shear (VS), and combined mechanism (CM) injuries. The second classification used for PRIs was the Arbeitsgemeinschaft für Osteosynthesefragen (AO) classification system, which categorises pelvic injuries based on the anatomical and biomechanical characteristics of the fractures [18].
Combining these two classifications for PRIs offers a more comprehensive diagnostic approach by addressing injury mechanisms and fracture anatomy. This dual system aids in treatment planning by tailoring interventions to specific trauma dynamics and structural stability, enabling a more personalised approach. Additionally, it enhances risk assessment by highlighting both force vectors and stability issues, improving outcome predictions.
Urinary-sequelae assessment
Urinary sequelae were defined as any postoperative urinary dysfunction, including incontinence, urinary retention, and infection. These were assessed during the initial postoperative period and the three month, six month, and one year follow-ups. Data were obtained by adapting the Questionnaire for female Urinary Incontinence Diagnosis (QUID) and the Female Urinary Symptom Score (FUSS) [19, 20].
QUID is a validated, self-administered tool for assessing the type and severity of urinary incontinence in women based on six items that allow distinguishing between stress and urge urinary incontinence according to symptom frequency [19]. FUSS is a brief, self-reported questionnaire for assessing the severity and impact of lower urinary tract symptoms in women based on questions related to symptoms, such as urinary frequency, urgency, incontinence, and nocturia [20].
Perioperative pelvic-image assessment protocol
Prior to a definite surgical procedure, pelvic imaging—including AP, inlet, and outlet X-ray views and multi-planar computed tomography (mpCT)—was performed to classify fracture types and guide surgical planning. Postoperative imaging was conducted the following day to assess reduction quality by examining fracture gap alignment. The quality of reduction post-osteosynthesis for PRIs was evaluated using the Matta/Tornetta and Levaivre criteria to assess pelvic symmetry in both the vertical and horizontal planes [21, 22]. The Matta/Tornetta criteria quantify reduction quality based on residual vertical displacement on postoperative imaging [21], while the Levaivre criteria evaluate horizontal plane residual deformity [22]. Based on these assessments, the reduction quality between the hemipelvises was categorised as anatomical (difference of 0–5 mm), good (6–10 mm), fair (10–20 mm), or poor (>20 mm).
Postoperative rehabilitation protocol and functional assessment protocol
Postoperative rehabilitation was conducted according to our institutional protocol (see Supplementary Methods). Functional outcomes were evaluated in all patients at three, six and 12 months post-injury using the Merle d’Aubigné and Majeed scoring systems. The Merle d’Aubigné score assesses pain, mobility, and walking ability, with each domain rated on a scale from 0 (worst) to 6 (best) [23]. The Majeed score, specifically designed for pelvic injuries, includes seven items with a total score ranging from 0 to 100 points [24].
Statistical analysis
Descriptive statistics were used to summarise the demographic and clinical characteristics of the study population. Continuous variables were reported as median and interquartile range (IQR) or mean and standard deviation (SD), depending on their distribution. Categorical variables were presented as frequencies and percentages. To assess the relationships between continuous variables, Pearson correlation tests were conducted. The Mann–Whitney U test and Kruskal–Wallis test were applied for comparisons between two or more independent groups, respectively.
Univariate and multivariate logistic regression analyses were performed to identify factors associated with urinary dysfunction at six and 12 months, with results expressed as odds ratios (ORs) with 95% confidence intervals (CIs). Linear regression analyses were used to evaluate continuous urinary outcomes (QUID-stress, QUID-urge, and FUSS scores), with results presented as β coefficients and 95% CIs.
For repeated patient-reported outcome (PRO) measures (QUID stress and urge scores and FUSS at 1, 3, 6 and 12 months), a linear mixed-effects model with a random intercept for each patient was used to account for within-subject correlation. Variables with missing 12-month outcomes (Merle d’Aubigné, Majeed, QUID stress and urge, and FUSS scores; five cases each) were handled by complete-case analysis. P < 0.05 was considered statistically significant. All analyses were performed using SPSS version 26.0 (IBM, Armonk, NY, USA).
Results
During the study period, a total of 58 patients were enrolled and analysed. The mean age of the cohort was 43.2 (± 18.7) years. The most frequent cause of PRIs was motor vehicle collisions (74.1%), followed by falls from height (13.8%), pedestrian injuries (5.2%), falls from standing height (5.2%), and crush injuries (1.7%). Extremity fractures were the most common associated injury (39.2%), followed by blunt chest trauma (22.4%) and head injuries (20.7%). Seven patients presented with shock status (systemic blood pressure less than 90 mmHg) during triage. The median ISS was 9 (IQR: 18), while the median NISS was 12.5 (IQR: 18). Emergent AE (emboli material: gelfoam) was performed in eight patients (13.8%) to achieve haemostasis, with six undergoing AE of bilateral internal iliac arteries due to severe hypotension during resuscitation.
The perioperative details of PRIs are summarised in Table 1. According to the Young and Burgess classification system, the LC type was the most prevalent, accounting for 69.0% of cases. Type B PRI under the AO classification system was the most common fracture type (84.5%). Most ventral surgical approaches used the intrapelvic route (78.2%). Open reduction techniques were predominantly used for ventral approaches (87.3%) and closed reduction techniques for dorsal approaches (72.7%). The mean time from injury to surgery was 6.8 ± 9.3 days. The mean duration of Foley catheter placement was 8.5 ± 5.7 days.
Table 1. Perioperative details of the 58 enrolled patientsFracture classification (Young and Burgess)Number (%) Lateral compression40 (69.0) Anteroposterior compression9 (15.5) Vertical shear9 (15.5)Fracture classification (AO) Type B49 (84.5) Type C9 (15.5)Surgical approach Ventral approach25 (43.1) Dorsal approach3 (5.2) Combined ventral and dorsal approach30 (51.7)Ventral surgical approach55 (100) Classified by closed/open reduction Closed reduction6 (10.9) Open reduction48 (87.3) Hybrid1 (1.8) Classified by intra-/extrapelvic route Intrapelvis43 (78.2) Extrapelvis12 (21.8)Dorsal surgical approach33 (100) Classified by closed/open reduction Closed reduction24 (72.7) Open reduction9 (27.3)Surgery related complications4 (7.9)AO: Arbeitsgemeinschaft für Osteosynthesefragen
Nearly half of the patients reported residual urinary symptoms 1 month post-injury, as assessed by QUID (stress score: 48.6%; urge score: 51.4%), and 74.1% of patients exhibited symptoms as assessed by FUSS (Fig. 1a). Notably, symptom severity showed significant improvement over time across all evaluation points at one, three, six and 12 months post-injury (Fig. 1b) as evidenced by the repeated measures analysis of variance results (P = 0.04 for stress score, 0.02 for urge score and 0.005 for FUSS). Figures 2, 3 and 4 illustrate various fracture patterns along with the analyses of their associated urinary symptoms.
Fig. 1. Urinary assessments over time following pelvic-ring injury in women. (a) The proportions of patients with stress incontinence (Stress score > 1), urge incontinence (Urge score > 1), and a composite urinary symptom score (FUSS > 1) at the 1-, 3-, 6-, and 12-month follow-up periods. (b) The mean scores for stress incontinence, urge incontinence, and FUSS during the same intervals. FUSS: Female Urinary Symptom Score
Fig. 2. Case presentation of an 84-year-old woman with a PRI classified as LC II (AO B2.2) resulting from a low-energy fall from standing height with related urinary sequelae assessments. (a) and (b) Preoperative X-ray and CT images. (c) Postoperative CT image. (d) Follow-up image at 1 year postoperatively
Fig. 3. Case presentation of a 21-year-old woman with a PRI classified as APC II (AO B2.3) sustained in a motor vehicle accident with related urinary sequelae assessments. (a) and (b) Preoperative X-ray (without pelvic binder) and CT scan (with pelvic binder). (c) Postoperative CT image. (d) One-year postoperative follow-up image
Fig. 4. Case presentation of a 62-year-old woman with a VS pelvic ring injury (AO C3.3) sustained in a motor vehicle accident with related urinary sequelae evaluations. (a) and (b) Preoperative CT scans showing the injury and a Morel-Lavallée lesion involving the right buttock and the posterior thigh. (c) Postoperative CT image. (d) Follow-up image at 1 year postoperatively
Advanced age, higher ISS and NISS, AE occurrence, ventral approach, intrapelvic approach, and time from injury to surgery were identified as factors contributing to residual urinary symptoms post-osteosynthesis for PRIs (Table 2). Logistic regression analysis revealed that greater injury severity, represented by a higher NISS, was independently associated with urinary symptoms at six months (adjusted OR: 1.05; 95% CI 1.00–1.12; P = 0.049), whereas other factors were not significant after multivariate adjustment (Tables 3 and 4). In the linear regression analyses, Foley catheter duration showed a marginal association with higher urinary symptom scores at six months (β = 0.03, 95% CI 0.00–0.06, P = 0.08) (Supplementary Tables 1 and 2), suggesting a possible short-term influence of prolonged catheterisation on postoperative urinary function. However, this effect was not sustained at 12 months (β = 0.02, 95% CI − 0.01 to 0.05, P = 0.25).
Table 2. Correlation analysis of significant factors influencing urinary dysfunctionQUID questionnaireFUSS questionnaireQUID + FUSSStress scoreUrge score R P-value R P-value R P-value R P-value 1-month assessment Age0.3140.010.280.02Intrapelvic approach0.0360.0210.0020.002Injury-to-surgery time (days)0.2990.024 3-month assessment Age0.3140.0080.2850.017ISS0.3510.0030.3240.006NISS0.3230.0060.310.009Ventral approach0.002AE0.0060.008Intrapelvic approach0.0030.0010.001 6-month assessment Age0.2650.0260.2490.038AE0.0340.030.0150.007Ventral approach0.016Intrapelvic approach0.0210.0020.001< 0.001Injury-to-surgery time (days)0.280.035 12-month assessment AE0.025Ventral approach0.0030.0310.029Intrapelvic approach0.0190.0140.0020.001AE, arterial embolisation; FUSS, Female Urinary Symptom Score; ISS, Injury Severity Score; NISS, New Injury Severity Score; QUID, Questionnaire for Urinary Incontinence Diagnosis
Table 3. Univariate logistic regression analyses for factors associated with urinary dysfunction at 6 and 12 monthsPredictors6-month evaluation12-month evaluationQUID-StressQUID-UrgeFUSSQUID + FUSSQUID-StressQUID-UrgeFUSSQUID + FUSSAge1.04 (1.00-1.08)^a^, P = 0.041.05 (1.01–1.10), P = 0.021.05 (1.01–1.10), P = 0.021.04 (1.00–1.08), P = 0.041.02 (0.97–1.07), P = 0.401.02 (0.97–1.07), P = 0.401.04 (0.99–1.09), P = 0.101.02 (0.97–1.07), P = 0.38NISS1.06 (1.01–1.12), P = 0.031.05 (1.00–1.11), P = 0.0451.05 (1.00–1.11), P = 0.0491.05 (1.00–1.12), P = 0.051.03 (0.98–1.08), P = 0.221.03 (0.98–1.08), P = 0.211.03 (0.98–1.08), P = 0.191.03 (0.98–1.08), P = 0.18AE2.4 (1.1–5.8), P = 0.032.1 (1.0–4.7), P = 0.0463.0 (1.2–7.2), P = 0.022.5 (1.1–6.0), P = 0.041.2 (0.5–3.0), P = 0.621.3 (0.5–3.0), P = 0.581.4 (0.5–3.2), P = 0.551.3 (0.5–3.0), P = 0.60Intrapelvic approach2.0 (1.0–4.3), P = 0.061.9 (0.9–3.9), P = 0.082.8 (1.1–6.9), P = 0.042.0 (1.0–4.3), P = 0.061.5 (0.7–3.3), P = 0.251.5 (0.7–3.2), P = 0.241.6 (0.7–3.6), P = 0.251.6 (0.8–3.4), P = 0.15Combined anterior & posterior approach1.8 (0.9–3.9), P = 0.091.7 (0.8–3.6), P = 0.111.8 (0.8–4.2), P = 0.121.8 (0.9–3.9), P = 0.091.3 (0.6–2.9), P = 0.341.4 (0.7–2.9), P = 0.281.3 (0.6–2.8), P = 0.341.4 (0.7–2.9), P = 0.30Shock1.2 (0.6–2.3), P = 0.601.2 (0.6–2.4), P = 0.581.3 (0.7–2.4), P = 0.541.2 (0.6–2.3), P = 0.601.1 (0.5–2.3), P = 0.801.1 (0.5–2.3), P = 0.801.2 (0.5–2.5), P = 0.761.1 (0.5–2.3), P = 0.80Injury-to-surgery time (days)1.01 (0.96–1.06), P = 0.701.01 (0.96–1.06), P = 0.681.01 (0.97–1.05), P = 0.721.01 (0.96–1.06), P = 0.701.00 (0.95–1.05), P = 0.951.00 (0.95–1.05), P = 0.941.00 (0.95–1.05), P = 0.921.00 (0.95–1.05), P = 0.95Foley catheter duration (days)1.02 (0.99–1.05), P = 0.121.02 (0.99–1.05), P = 0.131.02 (0.99–1.05), P = 0.101.02 (0.99–1.05), P = 0.121.01 (0.98–1.04), P = 0.251.01 (0.98–1.04), P = 0.261.01 (0.98–1.04), P = 0.281.01 (0.98–1.04), P = 0.25Fracture classification: APC vs. LC1.4 (0.7–2.9), P = 0.311.3 (0.6–2.7), P = 0.331.5 (0.7–3.1), P = 0.281.4 (0.7–2.8), P = 0.291.2 (0.6–2.5), P = 0.421.3 (0.6–2.6), P = 0.391.4 (0.6–2.9), P = 0.371.3 (0.6–2.7), P = 0.39Fracture classification: VS vs. LC1.7 (0.7–3.8), P = 0.221.5 (0.6–3.6), P = 0.261.6 (0.7–3.9), P = 0.241.6 (0.7–3.6), P = 0.241.4 (0.6–3.2), P = 0.301.4 (0.6–3.1), P = 0.321.5 (0.7–3.3), P = 0.271.4 (0.6–3.1), P = 0.31^a^Statistical results are shown in odds ratio (95% confidence interval), p value**P* < 0.05 represents statistical significanceAE, arterial embolisation; APC: anteroposterior compression; FUSS, Female Urinary Symptom Score; LC: lateral compression; NISS: new injury severity score; QUID, Questionnaire for Urinary Incontinence Diagnosis; VS: vertical shear
Table 4. Multivariate logistic regression analyses for independent predictors of urinary dysfunction at 6 and 12 monthsPredictors6-month evaluation12-month evaluationQUID-StressQUID-UrgeFUSSQUID + FUSSQUID-StressQUID-UrgeFUSSQUID + FUSSNISS1.05 (1.00–1.12)^a^, P = 0.0491.05 (1.00–1.11), P = 0.0451.05 (1.00–1.11), P = 0.049*1.05 (1.00–1.12), P = 0.051.03 (0.98–1.08), P = 0.221.03 (0.98–1.08), P = 0.211.03 (0.98–1.08), P = 0.191.03 (0.98–1.08), P = 0.18^a^The statistical results are shown in [odds ratio (95% confidence interval), p value]*P < 0.05 represents statistical significanceFUSS, Female Urinary Symptom Score; NISS: new injury severity score; QUID, Questionnaire for Urinary Incontinence Diagnosis
A linear mixed-effects model was applied to analyse repeated FUSS scores at one, three, six and 12 months, with a random intercept for each patient. Fixed effects included time, age, NISS, arterial embolisation, intrapelvic approach, and combined anterior–posterior approach. The model showed a significant improvement in FUSS scores over time (P < 0.001), reflecting progressive recovery of urinary function. Among the covariates, higher NISS was independently associated with worse urinary symptom scores (β=+0.05 per point, 95% CI + 0.01–+0.10, P = 0.03), whereas embolisation and surgical approach were not significantly related after adjustment.
When evaluating the quality of pelvic reduction, 52 cases (89.7%) were classified as excellent (n = 43) or good (n = 9) based on the Matta/Tornetta criteria, while 45 cases (77.9%) were categorised as excellent (n = 28) or good (n = 17). No significant correlation was found between the quality of reduction and urinary dysfunction (Supplementary Table 3). The association between functional performance and urinary symptoms was analysed (Supplementary Table 4), revealing a consistent negative correlation across all evaluation time points. This finding indicates that a reduction in urinary symptoms over time corresponded with progressive improvement in functional outcomes.
Discussion
This study evaluated urinary sequelae in a female cohort following surgical treatment for PRIs. Nearly half of 58 participants exhibited urinary symptoms one month post-injury. However, these symptoms showed progressive improvement over time, aligning with functional status enhancements. In the multivariate analysis, higher NISS was the only factor independently associated with early urinary dysfunction at six months, whereas age, embolisation, and surgical approach were not significant factors. The longitudinal mixed-effects model further confirmed significant time-dependent improvement in urinary function across the first postoperative year.
Healthy urinary function correlates with the abdominal wall muscle and pelvic floor physiological presentation. The pelvic floor is a collection of muscles that span the pelvis base, forming a supportive “sling” working alongside surrounding tissues to hold the pelvic organs in their positions [25, 26]. The bladder should not exhibit involuntary contractions during the filling phase, even when provoked [27]. When urinating, the urethral sphincter should relax, allowing the urethra to open with a consistent urine flow. Meanwhile, abdominal wall muscles also generate intraabdominal pressure supporting urinary function [28]. After the insult from PRI and its related management, normal urination physiology may change, resulting in urinary dysfunction.
AE, a haemostatic intervention frequently used during the resuscitative phase of PRI management, has been identified as a potential contributor to urinary dysfunction post-PRIs [29–31]. AE offers notable advantages, including specificity for arterial bleeding, a minimally invasive approach compared to surgical retroperitoneal gauze packing, and a high haemostasis success rate [32, 33]. However, AE is also associated with complications, including urinary dysfunction [14, 34]. Ramasamy et al. [14] reported that up to 50% of patients undergoing AE experienced urinary dysfunction. Nonselective internal iliac artery embolisation has been proposed as a key factor contributing to this sequela [34]. Although AE was not an independent predictor of urinary dysfunction after multivariate adjustment, the observed tendency toward higher symptom scores among embolised patients suggests that ischemic or neural effects may still contribute to transient urinary disturbances. This finding underscores the importance of adopting selective embolisation techniques whenever feasible to preserve pelvic organ perfusion while achieving haemostasis.
In our cohort, a significant proportion of patients (87.3%) underwent ventral approaches for PRI open reduction and internal fixation. Common ventral approaches, including the ilioinguinal, anterior intrapelvic, and pararectus approaches, were used to address ventral and selected dorsal lesions associated with PRIs [35–37]. These techniques involve varying degrees of abdominal wall muscle manipulation—either detachment of the external oblique in the ilioinguinal approach or incision of the rectus abdominis and external oblique aponeurosis in the anterior intrapelvic and pararectus approaches, respectively. Although these procedures may transiently affect lower abdominal or pelvic floor musculature and potentially alter urinary physiology in the immediate postoperative phase, our multivariate analysis did not identify surgical approach as an independent risk factor for urinary dysfunction. This finding suggests that postoperative urinary symptoms are more likely related to overall injury severity and physiological recovery than to surgical corridor.
Osteosynthesis for PRIs primarily aims to achieve symmetric alignment of the bilateral hemipelvises under rigid fixation, thereby preserving pelvic-ring physiological functions, including protection of internal organs and facilitation of weight-bearing ambulation [38]. PRI-related deformities can lead to external compression or elevation of the bladder, potentially reducing its capacity for urine storage and contributing to stress or urgency-related urinary symptoms [4, 39]. In this study, no significant correlation was identified between PRI reduction quality and urinary sequelae. This may be attributed to the consistent application of standard reduction criteria under modern surgical strategy and internal fixator development, which resulted in anatomically restoring pelvic integrity, maintaining structure stability until fracture union, and allowing early weight-bearing ambulation in most cases. Consequently, the potential impact of post-injury pelvic asymmetry on urinary dysfunction may have been mitigated.
These findings emphasise the importance of precise anatomical reduction during osteosynthesis, not only for improving functional mobility in a reasonable time but also for minimising the urinary complication risk in patients recovering from PRIs.
Some limitations must be acknowledged. First, while the functional and urinary questionnaires were prospectively collected, the study was limited by a relatively small sample size and short follow-up duration with missing data. Second, sexual and urinary functions are closely interrelated in women; however, this study did not analyse sexual function as most patients declined to respond, possibly due to cultural factors. Third, decisions on whether to perform AE, its laterality, and the use of gelfoam were made by the emergency physicians based on acute clinical needs; therefore, a formal dose–response analysis was not feasible. Although AE was not an independent predictor in our multivariate analysis, its potential transient influence on pelvic organ perfusion cannot be excluded. Fourth, selection bias may have occurred, with patients experiencing severe injuries or complications being underrepresented. Reliance on patient-reported outcomes also raised the risk of recall bias or underreporting. Finally, although no patient developed a symptomatic urinary tract infection during the index admission, routine urine testing was not performed after discharge; therefore, postoperative urinary tract infections during follow-up cannot be entirely excluded. Although Foley duration showed no lasting effect, transient urinary irritation from prolonged catheterisation cannot be ruled out. Future studies with larger cohorts, longer follow-ups, and culturally sensitive approaches are needed to address these issues.
Implications for practice and/or policy
Routine assessment using validated instruments such as QUID and FUSS should be integrated into postoperative care. Although surgical or embolisation techniques are not independently associated with dysfunction, greater injury severity warrants closer surveillance and early rehabilitation. Clinicians should emphasise selective embolisation, minimise soft-tissue disruption, and initiate early mobilisation to support recovery. These findings support the development of guidelines for female pelvic trauma management.
Conclusions
Urinary sequelae may occur in women following pelvic-ring injuries even without direct urinary tract damage. Greater injury severity was the only independent predictor of early urinary dysfunction, while most patients showed gradual recovery over time. Careful surgical technique, selective arterial embolisation, and structured rehabilitation remain essential to optimise pelvic stability, functional recovery, and long-term urinary outcomes.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
Supplementary Material 3
Supplementary Material 4
Supplementary Material 5
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1de Carvalho MLAS, Bezerra LO, Oliveira JMP, Oliveira MCE, Micussi MTABC (2024) Pelvic floor muscle training in women with urinary incontinence and pelvic organ prolapse: a protocol study. P Lo S ONE 19:Article e 0308701. 10.1371/journal.pone.030870110.1371/journal.pone.0308701 PMC 1132913539150919 · doi ↗ · pubmed ↗
- 2AO Foundation (2018) AO/OTA Fracture and Dislocation Classification Compendium. Wolters Kluwer. AO Foundaition. https://classification.aoeducation.org. Accessed 6 May 2020
- 3Hsiao P-M, Liao S-C, Chen I-J et al (2023) Incidence of deep vein thrombosis and symptomatic pulmonary embolism in Taiwanese patients with pelvic and/or acetabular fractures: a retrospective study. Sci Rep 13:Article 16352. 10.1038/s 41598-023-43449-410.1038/s 41598-023-43449-4PMC 1053949537770539 · doi ↗ · pubmed ↗