The Efficacy of Spirulina on Cognitive Function, Psychological and Clinical Indicators in Men Patients Under Methadone Therapy (a Randomized Trial)
Morteza Zamani Asadolah‐poor‐kashi, Peyman Mamsharifi, Freshteh Haerifar, Mehrdad Simani, Amir Ghaderi, Fateme Mehrzad

TL;DR
A 12-week study found that Spirulina reduced anxiety and stress in men on methadone therapy, but had no effect on depression, sexual function, or cognitive performance.
Contribution
This is the first randomized trial to show Spirulina's potential in reducing anxiety and stress in methadone-maintained patients.
Findings
Spirulina significantly reduced anxiety and stress scores compared to placebo.
No significant changes were observed in depression, sexual function, craving, or cognitive performance.
Spirulina may serve as a supportive intervention for anxiety and stress in MMT patients.
Abstract
Patients undergoing methadone maintenance therapy (MMT) often experience psychological issues and clinical dysfunctions, which can negatively impact the effectiveness of the treatment. Addressing these challenges is crucial for improving patient outcomes. This clinical trials aimed to evaluate the effectiveness of Spirulina (SP) supplementation on craving, psychological distress, sexual performance, and cognitive functions in male receiving methadone. In this double‐blind randomized clinical trial, 50 male patients undergoing MMT were randomly assigned to receive either the SP (500 mg twice daily, n = 25) or the placebo (n = 25) for 12 weeks. Assessments were conducted at baseline and at the end of the intervention. Psychological indicators were measured using the Depression, Anxiety, and Stress Scale‐21 (DASS‐21); sexual function was evaluated with the International Index for Erectile…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
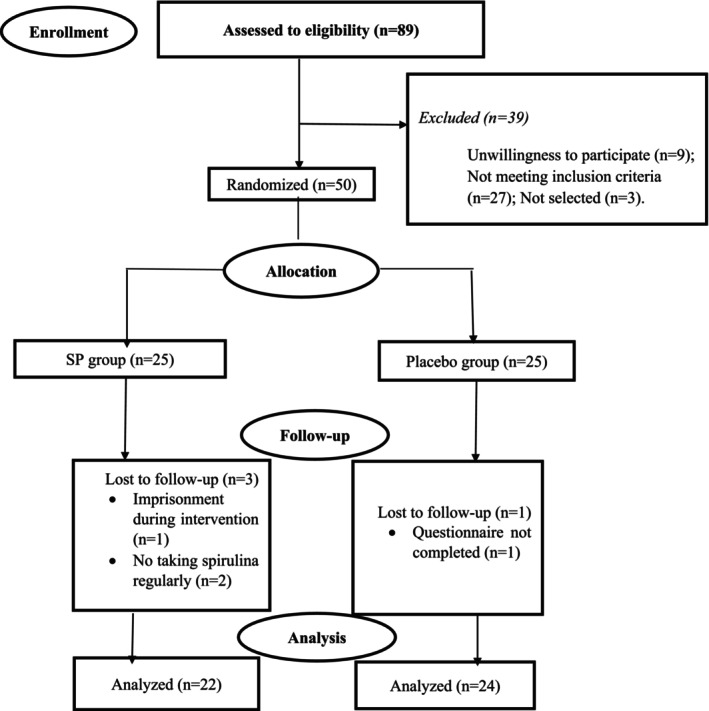 FIGURE 1
FIGURE 1| Variables | Placebo group ( | SP group ( |
|
|---|---|---|---|
| Age (years) | 44.20 ± 4.88 | 42.81 ± 4.47 | 0.32 |
| Age of first drug abuse experience (years) | 19.50 ± 2.08 | 19.04 ± 2.12 | 0.46 |
| Duration MMTPs (years) | 11.66 ± 4.07 | 10.86 ± 3.56 | 0.48 |
| Methadone dose (mL/d) | 27.08 ± 6.90 | 25.90 ± 8.11 | 0.59 |
| Education Level (%) | |||
| Elementary | 8 (33.3) | 6 (27.3) | 0.58 |
| Intermediate | 9 (37.5) | 8 (36.4) | |
| Diploma | 3 (12.5) | 6 (27.3) | |
| University education | 4 (16.7) | 2 (9.1) | |
| Marital status (%) | |||
| Single | 8 (33.3) | 6 (27.3) | 0.84 |
| Married | 11 (45.8) | 10 (45.5) | |
| Widow/Divorced | 5 (20.8) | 6 (27.3) | |
| Other medications used (%) | |||
| None | 20 (83.3) | 14 (63.6) | 0.23 |
| Anti‐depressant | 1 (4.2) | 4 (18.2) | |
| Sedative‐Hypnotic | 3 (12.5) | 4 (18.2) | |
| Variables | Placebo group ( | SP group ( | β (95% CI) | Effect size |
| ||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | End‐of‐trial | Change | Baseline | End‐of‐trial | Change | ||||
| Mental health (DASS‐21) | |||||||||
| Depression | 20.70 ± 2.72 | 20.54 ± 2.91 | −0.16 ± 1.09 | 21.09 ± 2.63 | 20.27 ± 2.58 | −0.81 ± 1.36 | −0.70 (−1.46, 0.05) | 0.081 | 0.06 |
| Anxiety | 17.16 ± 1.90 | 17.12 ± 1.75 | −0.04 ± 1.23 | 17.09 ± 2.02 | 16.04 ± 2.31 | −1.04 ± 1.32 | −0.81 (−1.52, −0.10) | 0.118 | 0.02 |
| Stress | 22.62 ± 3.22 | 22.29 ± 3.45 | −0.33 ± 1.52 | 23.40 ± 4.00 | 21.81 ± 3.88 | −1.59 ± 2.23 | −1.22 (−2.36, −0.08) | 0.105 | 0.03 |
| Sexual function (IIEF) | 24.83 ± 4.65 | 25.0 ± 4.61 | 0.16 ± 1.80 | 22.81 ± 5.26 | 22.86 ± 5.17 | 0.04 ± 1.17 | −0.08 (−1.04, 0.86) | 0.001 | 0.85 |
| Variables | Placebo group ( | SP group ( | β (95% CI) | Effect size |
| ||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | End‐of‐trial | Change | Baseline | End‐of‐trial | Change | ||||
| DDQ (craving) | 30.58 ± 4.90 | 30.50 ± 4.76 | −0.08 ± 1.05 | 29.36 ± 4.43 | 29.04 ± 4.41 | −0.31 ± 1.35 | −0.08 (−0.76, 0.58) | 0.002 | 0.79 |
| FAS‐test (Numbers total word) | 33.41 ± 3.09 | 33.20 ± 2.57 | −0.20 ± 2.02 | 34.45 ± 2.98 | 34.13 ± 2.83 | −0.31 ± 2.76 | 0.14 (−1.08, 1.37) | 0.001 | 0.81 |
| IGT (Iowa Gambling Task) | 25.08 ± 1.99 | 25.41 ± 1.81 | 0.33 ± 1.27 | 25.72 ± 1.83 | 25.63 ± 1.83 | −0.09 ± 1.15 | −0.37 (−1.10, 0.35) | 0.026 | 0.30 |
| TMT (Trail Making Test) | |||||||||
| TMT‐A | 30.20 ± 4.07 | 30.33 ± 4.21 | 0.12 ± 1.32 | 30.27 ± 3.16 | 29.81 ± 3.50 | −0.45 ± 1.94 | −0.54 (−1.56, 0.48) | 0.028 | 0.29 |
| TMT‐B | 84.87 ± 12.04 | 85.29 ± 12.57 | 0.41 ± 2.44 | 83.22 ± 11.64 | 82.50 ± 11.90 | −0.72 ± 2.14 | −1.20 (−2.60, 0.19) | 0.070 | 0.09 |
- —Kashan University of Medical Sciences10.13039/501100004048
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Bladder and Prostate Research · Hormonal and reproductive studies · Pharmacogenetics and Drug Metabolism
Introduction
1
Substance use disorder (SUD) remains a significant public health challenge, affecting millions of individuals across the globe. According to the 2021 World Drug Report by the United Nations Office on Drugs and Crime (UNODC), over 275 million people worldwide engaged in the use of controlled substances in the previous year, with more than 36 million individuals meeting the clinical criteria for SUD (Crime UNOoDa 2021). Among the substances contributing most significantly to the global burden of disease, opioids stand out as the leading cause of drug‐related fatalities, accounting for nearly 69% of all deaths associated with drug use (Lee et al. 2024).
In response to this crisis, methadone maintenance treatment programs (MMTPs) have emerged as a cornerstone in the management of opioid use disorder (OUD) (Ma et al. 2019; Chalabianloo et al. 2024). These programs are pivotal in mitigating opioid cravings and alleviating withdrawal symptoms, offering individuals a structured pathway toward recovery. However, despite its efficacy, methadone therapy is not without its complexities. Patients undergoing treatment often report a range of side effects, including sexual dysfunction, psychological challenges (Anxiety, stress and depression), and broader health concerns (Sanborn et al. 2022; Motazedian et al. 2021; Yee et al. 2014; Cheng et al. 2017). Also, the quality of life of these patients may be affected by various factors, including impaired cognitive functions, craving, social stigma, and financial difficulties (Dalili et al. 2025). Psychologically, it can be triggered by a range of internal and external cues (e.g., stress, physical withdrawal symptoms, and negative emotions) (Ilgen et al. 2008). Furthermore, ongoing struggles with cravings and co‐occurring mental health conditions can undermine the therapeutic benefits of methadone, complicating recovery and diminishing overall quality of life (Wen et al. 2023). These challenges underscore the need for comprehensive, multifaceted approaches to addiction treatment, addressing both the physiological and psychological dimensions of opioid dependence.
Spirulina (Arthrospira platensis) is a nutrient‐dense alga that has garnered recognition for its exceptional protein, vitamin, and mineral content, which exceeds that of many commonly consumed foods like soybeans. Recognized by the United Nations for its nutritional value, Spirulina (SP) is widely used as a dietary supplement due to its powerful antioxidant, antibacterial, antiviral, anti‐inflammatory, and antidiabetic properties (Jung et al. 2019). Studies suggest that SP can enhance the body‘s antioxidant defense systems and has shown potential in improving cognitive function, especially in individuals with neurological disorders (Abd Elkader et al. 2024). Recently, SP supplementation was suggested in subjects with mild to moderately severe depression. This may be due to the beneficial effects of SP intake on mental health disorders in these individuals. This study highlights two favorable benefits of SP supplementation [2 g/day of SP (two 1000 mg) for 8 weeks]: improved sleep latency and quality, and reduced anxiety, depression, and stress scores (Phansuea et al. 2025). Additionally, in an evidence involving multiple sclerosis patients received SP (1 g/day) for 12 weeks exerts anti‐inflammatory effects (IL‐6 and IL‐1β levels), statistically significant also improves physical health, including sexual performance and energy, and potentially mental health compared to placebo (Karimi et al. 2025). In 2025 a systematic review studies suggest that SP may help preserve or improve memory, cognitive performance, and mood by reducing inflammation and oxidative stress (Kumar et al. 2025). In addition to the anti‐inflammatory and antioxidant properties, SP might increase mental health status in MMT patients through many neurobiological mechanisms. SP administration can enhance levels of tryptophan, a precursor of serotonin, thereby promoting central serotonergic activity, which is closely linked to reduced anxiety, improved mood, and increased hopefulness and feelings of well‐being (Demelash 2018). Moreover, SP has been indicated to enhance brain‐derived neurotrophic factor (BDNF) expression, facilitating neuronal repair and neuroplasticity, which might facilitate to better subjective health status and cognitive‐emotional resilience (Trotta et al. 2022; Moradi‐Kor, Ghanbari, et al. 2020). Totally, these mechanisms, likely underlie SP positive effects on quality of life and mental health in the MMT population.
Despite the promising therapeutic effects of SP, no randomized controlled trials (RCTs) to date has directly evaluated SP supplementation in MMTPs. Existing evidence is largely indirect coming from other clinical populations or preclinical models, so the effects of SP on mental health, cognition, and sexual function specifically in MMTPs patients remain unknown. Conducting focused RCTs of SP in this population would address an important knowledge gap and could clarify whether SP is a useful adjunct to improve quality of life, psychological well‐being, cognitive function, and sexual health among individuals on MMTPs. The results of this investigation could provide valuable insights into the potential of SP as a complementary treatment in patients with SUD.
Methods
2
Study Population
2.1
The present study employed a randomized, double‐blind, parallel‐group experimental design, including a pretest and posttest. Fifty individuals, aged 30–50 years, who were undergoing MMTPs and seeking treatment at the Mehrparvar Substance Abuse Clinic in Kashan, Iran, participated in the RCTs (Figure 1). This trial was conducted following the ethical guidelines of the Declaration of Helsinki and was approved by the Ethics Committee of Kashan University of Medical Sciences (IR.KAUMS.MEDNT.REC.1402.186). The trial was also registered on the Iranian Clinical Trials website (https://irct.behdasht.gov.ir/trial/73743: IRCT20231101059923N2; Registration date: 2023‐12‐16). Before enrollment, participants were thoroughly informed about the study‘s goals, and they were given 1 week to decide whether to participate. Informed written consent was obtained from all participants, ensuring they fully understood the study's purpose and procedures before joining.
Flowchart of the clinical trial.
Inclusion and Exclusion Criteria
2.2
Inclusion Criteria: (A) Voluntary consent and informed willingness to participate, (B) Positive methadone urine test result, (C) Use of methadone for a minimum of 1 year, (D) Male participants aged between 30 to 50 years.
Exclusion Criteria: (A) Presence of chronic physical conditions, including phenylketonuria, autoimmune diseases, AIDS, hepatitis, liver and kidney disorders, or cardiovascular diseases at the time of enrollment, (B) Inability or failure to participate regularly, (C) Adverse side effects such as insomnia, abdominal discomfort, vomiting, or allergic reactions during the intervention.
Intervention
2.3
Participants were randomly assigned to the intervention groups using a block randomization method. First, the SP group was assigned the code “A” and the placebo group was assigned the code “B”. A randomization list was then generated using the website www.sealedenvelope.com/simple‐randomiser/v1/lists, selecting a sample size of 50 participants (with 25 in each group) and applying the permuted block randomization method (block size = 4). Based on this randomization list, subjects were assigned to one of the two groups (A or B). The randomization and group allocation process was concealed from the researchers and participants until the final analysis was completed. A third party, who was not involved in the clinical trial and was unaware of the randomization sequences, assigned the participants to numbered bottles of the corresponding supplements. The intervention group (n = 25) received 500 mg of SP capsules twice daily for 12 weeks, the timing and dosage were chosen based on prior evidence to ensure safety and potential therapeutic effects on psychological and clinical parameters (Moradi et al. 2021; Tamtaji et al. 2023). These capsules were provided by Reyhan Naghsh Jahan Pharmaceutical Company, Isfahan, Iran (Product registration code: 9080218987590713). The placebo group (n = 25) received two capsules daily, also from Reyhan Naghsh Jahan Company, which contained starch as a control. The placebo capsules were identical in appearance, shape, color, packaging, smell, and taste to the SP capsules. Participants were instructed not to use any additional vitamin or mineral supplements during the 3‐month intervention period and to maintain their regular diet and physical activity levels. Adherence to the intervention was monitored by counting the empty supplement containers at regular intervals. To encourage compliance, all participants received weekly reminders via text‐message on their mobile phones to ensure they took the SP or placebo as prescribed.
Measurements of Outcomes
2.4
The primary outcome measures included mental health indicators (depression, anxiety, and stress) and erectile function. Secondary outcome measures focused on craving and cognitive function, assessed using the IGT (Iowa Gambling Task), FAS (FAS‐test), TMT‐A (Trail Making Test Part A), and TMT‐B (Trail Making Test Part B).
Clinical Assessments
2.5
Participants enrolled in the MMTPs were asked to complete the study assessments at the clinic (e.g., demographic information). Additionally, all participants were evaluated for psychological indicators, cognitive function parameters, and clinical manifestations (using the DDQ) both before and after the intervention with SP or placebo.
(A) Psychological Measures: The Depression, Anxiety, and Stress Scale‐21 (DASS‐21) are a shortened version of the original DASS, containing 42‐items. The DASS‐21 includes 21 items: seven questions assess depression, seven items measure anxiety, and the remaining items focus on stress. Participants are asked to rate the presence of symptoms experienced in the past week, using a 4‐point Likert scale ranging (0–3). To calculate the final DASS‐21 score, the score for each subscale (depression, anxiety, and stress) is multiplied by two. The Persian version of the DASS‐21 has been validated by Sahebi et al. The internal consistency of the subscales is high, with Cronbach's alpha coefficients of 0.91 (depression), 0.87 (anxiety), and 0.90 (stress) (Lovibond and Lovibond 1995; Yazdi et al. 2019; Sahebi et al. 2005).
(B) Erectile Function: Sexual performance was evaluated using the International Index of Erectile Function (IIEF), a 15‐item questionnaire covering sexual desire, orgasmic, erection, satisfaction, and overall sexual well‐being. Total scores range between 0 and 75, with higher values indicating better sexual functioning. Scores ≤ 25 indicate varying degrees of sexual dysfunction, while 26–30 represent normal function (Rosen et al. 1997).
(C) Drug Craving: The original Drug Desire Questionnaire (DDQ) consists of 13 items designed to assess three key components of drug cravings: desire and intention to use drugs, negative reinforcement, and perceived control. Participants respond to each question on a seven‐point Likert scale, reflecting their feelings or thoughts. Responses are rated on a seven‐point Likert scale from 1 (not at all) to 7 (nearly complete) (Hassani‐Abharian et al. 2016).
(D) Cognitive Function: (1) FAS‐test: The FAS Test, which is part of the Neurosensory Center Comprehensive Examination for Aphasia. The FAS Test evaluates phonemic verbal fluency by requiring participants to generate as many words as possible beginning with the letters F, A, and S within one minute. This task evaluates their ability to access and produce words based on phonemic cues (Crockett 1977). (2) IGT: The Iowa Gambling Task (IGT) is a valuable tool for examining decision‐making processes in individuals. In this task, subjects are presented with four decks of cards. The first two decks offer higher rewards, but they also come with the risk of occasional negative points. In contrast, the other two decks provide smaller rewards but have a significantly lower risk of loss compared to the first two decks. The task determine participants’ ability to make advantageous decisions by weighing the potential rewards against the risks (Turnbull et al. 2014; Businelle et al. 2008).
(3) TMT: The Trail Making Test (TMT) consists of two subtests (e.g., TMT‐A and TMT‐B), designed to assess processing speed and cognitive flexibility. In TMT‐A, individuals are presented with numbers 1 through 25, randomly arranged in circles on a sheet of paper. They are instructed to connect the numbers in ascending order (i.e., 1‐2‐3) using a pen or pencil. In TMT‐B, the test is slightly more complex: the sheet contains both numbers and letters, and individuals must connect them in alternating ascending order (i.e., 1‐A‐2‐B). The performance on each part is usually measured by the time it takes to complete the task, with TMT‐B typically requiring more time than TMT‐A (Stuss et al. 2001; Lamberty et al. 1994).
Together, these validated instruments provided a comprehensive assessment of participants’ psychological well‐being, cognitive performance, and clinical status before and after SP supplementation.
Statistical Analysis
2.6
The Kolmogorov–Smirnov test was used to evaluate the normality of the data. Demographic, clinical and general features differences are presented as mean (SD), along with the corresponding frequency distributions. Differences in demographic characteristics between the two groups were done by the two‐sample t‐test and Chi‐square test. To evaluate the impact of the treatment intervention on the outcomes of the RCT, the analysis of the covariance (ANCOVA) test was applied, adjusting for baseline values and covariates. Statistical analyses were performed using the SPSS software (version 22, SPSS Inc., Chicago, IL, USA). p values < 0.05 were statistically significant.
Sample Size
2.7
We were unable to find a similar clinical study examining the effects of SP on cognitive function, psychological, and clinical indicators in individuals undergoing MMTPs, which could guide the sample size calculation based on the primary and secondary outcomes. Therefore, the sample size was determined based on previous research evaluating the effects of SP (Arthrospira platensis) supplementation on blood pressure, anthropometric indices, sleep quality, fatigue, mental health, and quality of life in individuals with ulcerative colitis (Moradi et al. 2021). To detect a mean difference (d) of 5.4 in the absolute change in stress scores as the primary variable between the two groups, with SDs of 7.50 and 5.83 for the SP and placebo groups, respectively, a two‐sided significance level of 0.05, and a power of 80% (α = 0.05, β = 0.20), the required sample size was calculated to be 25 individuals per group under MMTPs.
Results
3
A total of 89 individuals under MMTPs were initially screened for eligibility. Based on the study design, 50 patients met the inclusion criteria. These 50 participants were then randomly assigned to receive either SP or a placebo. In the placebo group, one participant did not complete the questionnaire at the end of the treatment period. In the SP group, three participants were excluded for various reasons: two did not adhere to the supplement regimen, and one was incarcerated during the intervention. As a result, 46 patients under MMTPs were included in the final analysis, with 22 in the intervention group and 24 in the placebo group. Figure 1 presents the CONSORT flow diagram for patient enrolment in this RCT.
All participants adhered to the clinical trial protocol and reported no adverse effects from either the SP or placebo supplements. An analysis of demographic and general characteristics revealed that both groups were similar in terms of key variables, including the age at which participants first used drugs, duration of MMTPs, methadone dose, education level, marital status, and other medications used. The mean age in the placebo group was 44.20 ± 4.88 years, while the mean age in the intervention group was 42.81 ± 4.47 years (Table 1).
TABLE 1: Demographic and general characteristics of the study patients (n = 46) a .
The effect of SP on primary outcomes, including mental health and erectile function, in participants under MMTPs is presented in Table 2. After 12 weeks of SP administration, significant improvements were observed in the anxiety scores (p = 0.02). Additionally, significant changes were noted in the stress scores as analyzed by ANCOVA (p = 0.03). However, no significant changes were found in depression scores and erectile function indices between the two groups (p = 0.06 and p = 0.85, respectively).
The secondary outcomes, such as craving and cognitive function, are reported in Table 3. No significant difference in the DDQ was observed between the two groups (p = 0.79). Furthermore, there were no significant differences in the FAS test scores and IGT between the placebo and SP groups when comparing baseline and post‐intervention results (p = 0.81 and p = 0.30, respectively). Additionally, SP supplementation for 12 weeks did not significantly affect TMT‐A and TMT‐B scores (p = 0.29 and p = 0.09, respectively).
Discussion
4
In this clinical trial, we aimed to investigate the effects of SP supplementation on psychological scales, erectile function, cravings, and cognitive performance in patients receiving MMTPs. After 12 weeks of intervention, significant reductions in anxiety and stress were observed in the intervention group, while no significant changes were seen in depression, erectile function, cravings, or cognitive function compared to the placebo group.
These findings are particularly significant given the limited research on the effects of SP in MMTPs patients. SP appears beneficial for reducing stress and anxiety, while the complex and multifactorial nature of SUD, combined with the broad psychological, physiological, and environmental factors, may explain why certain domains such as craving, erectile function and cognitive ability did not significantly improve (Rass et al. 2014). Methadone affects numerous biological systems, mental and physical health, potentially obscuring or interacting with any therapeutic benefits that SP might offer.
Craving in individuals under MMTPs arise from an intricate interaction of environmental, psychological, and neurobiological indicate (Biernacki et al. 2022). In other hand, addictive behaviors are multifaceted and deeply rooted, interventions targeting cravings likely require more comprehensive strategies beyond the anti‐inflammatory and anti‐oxidant effects of SP. However our results shown that SP may alleviate stress and anxiety, its influence on the complex neurobiological mechanisms that underlie craving appears to be minimal. These findings align with earlier reports emphasizing the difficulty of addressing craving and cognitive impairment in individuals maintained on SUD (Lewis et al. 2025; Sorrenti et al. 2021).
Many of evidences have been indicated the relationship between SUD and psychiatric disorders (e.g., depression, stress and anxiety syndromes) (Schuckit 2006). Neuro‐inflammation is an inflammatory response and thought to be connected with a variety of psychiatric disorders (Soytürk et al. 2025). Microalgae including SP exhibit biological activities such as neuroprotective effects, anti‐inflammatory, and antioxidant responses, collectively reducing inflammation‐related depressive behaviors (Bo 2025; Karkos et al. 2011). Our found that MMTPs who were supplemented with SP for 12‐weeks had a significant reduction in anxiety and stress score, but did not significant changes depression symptoms. Prior evidences have suggested that potential anti‐stress and anxiolytic effects of SP via its anti‐oxidant and anti‐inflammatory mechanisms, which help counteract neuro‐inflammation and oxidative stress commonly linked to psychiatric disorders (Sah et al. 2025; Calella et al. 2022). In animal model with exposed to chronic adolescent stress by Moradi‐Kor et al. (Moradi‐Kor, Dadkhah, et al. 2020), SP platensis administration, when combined with enriched environments and voluntary exercise, was shown to attenuate oxidative stress, anxiety and depressive‐like symptoms, additionally can protect biochemical defects. This may occur via interactions with the hypothalamic–pituitary–adrenal axis, leading to reduced oxidative damage. In another animal study indicate that SP has adaptogenic activity, and against a several of physiological, biochemical and histological perturbations induced through restraint stress (Juvekar and Nachankar 2003). In addition, improved quality of life was indicated in ulcerative colitis patients following two 500 mg day SP supplementation for 8 weeks, which could be correlated with improved stress status and sleep disturbances, while no significant changes occurred in fatigue, depression and anxiety scores (Moradi et al. 2021). In contrast, a triple‐blind RCT involving patients with hypertension found no significant differences in anxiety levels after 8‐weeks SP supplementation (2 g/day). The researchers suggested that the concurrent emergence of the COVID‐19 pandemic might have influenced outcomes (Far et al. 2022). The inconsistency of the effect of SP in the results of these studies with our study is probably due to differences in population characteristics, duration and dose of intervention, or disease pathology. The evidence indicated that SP microalgae nutrient might be considered as a preventive or therapeutic agent against brain health and reduce stress and anxiety through several mechanisms, including modulating energy metabolism and metabolic function (Sorrenti et al. 2021), upregulate BDNF expression, anti‐inflammatory, antioxidant, and neuroprotective mechanisms (Moradi‐Kor, Ghanbari, et al. 2020), protect the vascular wall of brain vessels and regulate pressure (Sorrenti et al. 2021), modulate cyclooxygenase‐2 (COX‐2) and protect against neurotoxicity (Reddy et al. 2000; Gaurav et al. 2010). Hence, SP alleviating mental health disorder commonly experienced in SUD, further improving patients’ perceived health and quality of life.
Our RCT shown that taking SP for 12‐weeks in patients under MMTPs, it did not influence on sexual function. Prior studies have indicated higher prevalence of sexual dysfunction in patients with opiate dependence under MMTPs (Zafarghandi et al. 2016). Studies in animal models have demonstrated that SP supplementation significantly improves both reproductive and erectile health. In one study, SP platensis reduced the negative effects of silver nanoparticles on male rats by increasing testosterone levels, enhancing antioxidant capacity, and reducing malondialdehyde levels. These changes were accompanied by improvements in testicular tissue structure and reduced sperm abnormalities (Moghanlo and Shariatzadeh 2022). Similarly, in another study with rats fed a hypercaloric diet, SP supplementation improved erectile function by enhancing nitric oxide availability, reducing inflammation, and promoting the relaxing effects of acetylcholine. SP also helped restore smooth muscle relaxation in cavernous tissue, decreased reactive oxygen species, and improved overall antioxidant capacity (Diniz et al. 2020). The lack of significant improvements in sexual function in our human study, compared to positive results from animal studies, could be attributed to several factors. Animal models typically have more controlled conditions, such as consistent dosage and treatment duration. At the same time human studies often face greater variability due to factors like individual health, lifestyle, and psychological influences. The divergence between physical sexual function and subjective satisfaction highlights the multidimensional nature of sexual health in SUD (Boggiano et al. 2017). While SP improves physiological capacity, psychological and relational factors may require concurrent targeted interventions (Trotta et al. 2022).
Numerous studies suggest that SP may offer positive effects on cognitive function. In particular, ethanolic extracts of SP maxima have been linked to improvements in visual learning, working memory, and vocabulary among older adults with mild cognitive impairment (Choi et al. 2022). Animal studies also show that adding SP to a high‐fat diet can boost spatial memory and learning abilities (Zhou et al. 2021). Clinical research further indicates that SP may enhance cognitive performance, help regulate blood sugar levels, and reduce inflammation in individuals with Alzheimer's disease (Tamtaji et al. 2023). Systematic reviews emphasize the antioxidant and anti‐inflammatory properties of SP, which could play a protective role against neurodegenerative diseases (Kumar et al. 2025). However, the results of this study did not show any significant improvement in cognitive function in the SP group. It's crucial to note that the primary mechanisms through which SP is thought to exert its benefits are its antioxidant and anti‐inflammatory effects. If cognitive decline in the participants is primarily driven by neurotransmitter imbalances, such as dopamine deficiency or disruptions in other neurotransmitter pathways, SP may not directly address these underlying causes (Trotta et al. 2022; Sorrenti et al. 2021). Hence, while SP shows promise in managing inflammation and oxidative stress, its effectiveness in combating cognitive decline tied to neurotransmitter dysfunction remains uncertain.
Our study showed that no significant changes were observed in depression, craving, sexual function, or cognitive performance. This may be due to the short intervention duration, small sample size and the complexity of the conditions being treated. Additionally, relapse, withdrawal symptoms and pain were not assessed, which should be considered in future studies. Previous evidences have linked SP with beneficial microbial shifts, which increase IL‐10 production (Verhoog et al. 2019; Kennedy et al. 2009). Due to the limited budget, this RCT did not include metabolic profiles (Oxidative stress and anti‐inflammatory markers) assessments and gut microbiota analysis, which provided further insight into SP biological effects in MMTPs. Future reports should evaluate microbiome mediated mechanisms and metabolic markers. Furthermore, we did not evaluate the physical activity and dietary intakes in MMTPS; hence, we requested the patients not to change their regular physical activity and dietary intakes.
Conclusion
5
In conclusion, this study suggests that SP supplementation may be particularly beneficial for managing anxiety and stress in individuals undergoing MMTPs. However, further research is necessary to explore its potential in improving craving, depression, sexual function, and cognitive health. Future studies should focus on longer treatment durations, larger sample sizes, and a broader range of outcome measures to gain a deeper understanding of SP effects in SUD.
Author Contributions
Morteza Zamani Asadolah‐poor‐kashi: conceptualization (equal), data curation (equal), investigation (equal), methodology (equal), project administration (equal), validation (equal), visualization (equal), writing – original draft (equal), writing – review and editing (equal). Peyman Mamsharifi: data curation (equal), investigation (equal), methodology (equal), writing – review and editing (equal). Freshteh Haerifar: methodology (equal), validation (equal), visualization (equal), writing – original draft (equal). Mehrdad Simani: conceptualization (equal), funding acquisition (equal), methodology (equal), validation (equal), visualization (equal), writing – original draft (equal), writing – review and editing (equal). Amir Ghaderi: conceptualization (equal), data curation (equal), funding acquisition (equal), methodology (equal), project administration (equal), resources (equal), software (equal), supervision (equal), validation (equal), visualization (equal), writing – original draft (equal), writing – review and editing (equal). Fateme Mehrzad: conceptualization (equal), data curation (equal), funding acquisition (equal), methodology (equal), project administration (equal), resources (equal), software (equal), supervision (equal), validation (equal), visualization (equal), writing – original draft (equal), writing – review and editing (equal).
Funding
This study was financially supported by Kashan University of Medical Sciences (Clinical Research Development Unit‐Matini/Kargarnejad Hospital), Iran, with a grant code [402110].
Ethics Statement
The Ethics Committee of Kashan University of Medical Sciences approved the study protocol under the approval number IR.KAUMS.MEDNT.REC.1402.186 and registered at the Iranian Registry of Clinical Trials (https://irct.behdasht.gov.ir/trial/73743: IRCT20231101059923N2) at 16/12/2023. All methods involving human participants in this study adhered to the ethical standards set by institutional and national research committees and were conducted following the principles outlined in the 1964 Helsinki Declaration and its subsequent amendments. All participants provided their informed consent before beginning the study. Each participant received a thorough explanation of the goals, procedures, potential risks, and benefits of the research before giving their agreement. Volunteers were also given the chance to ask any queries they might have had. Participants were informed that there would be no consequences if they chose to withdraw from the study at any time and that participation was completely optional. Confidentiality and privacy were strictly maintained during the entire trial. The anonymized and safely stored identifying personal data was only accessible to the research team. Data were examined in aggregate form to preserve the anonymity of individual responders. Conclusions were presented without any personally identifiable information to adhere to confidentiality rules.
Consent
The informed consents were completed by all participants.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abd Elkader, H.‐T. A. E. , A. E. Essawy , and A. S. Al‐Shami . 2024. “Bioactive Compounds of the Genus Spirulina Can Prevent the Progression of Neurological Diseases.” Neurochemical Journal 18, no. 1: 47–59.
- 2Biernacki, K. , S. Lopez‐Guzman , J. C. Messinger , et al. 2022. “A Neuroeconomic Signature of Opioid Craving: How Fluctuations in Craving Bias Drug‐Related and Nondrug‐Related Value.” Neuropsychopharmacology 47, no. 8: 1440–1448.34916590 10.1038/s 41386-021-01248-3PMC 9205977 · doi ↗ · pubmed ↗
- 3Bo, X. 2025. “Microalgae and Exercise: From Molecular Mechanisms and Brain Health to Clinical Perspectives in the Context of 3P Medicine.” EPMA Journal 16, no. 2: 351–386.40438495 10.1007/s 13167-025-00405-8PMC 12106266 · doi ↗ · pubmed ↗
- 4Boggiano, V. L. , H. L. T. Nguyen , L. H. Nguyen , et al. 2017. “Sexual Behaviors Among Methadone Maintenance Patients in a Mountainous Area in Northern Vietnam.” Substance Abuse Treatment, Prevention, and Policy 12, no. 1: 39.28841918 10.1186/s 13011-017-0123-4PMC 5574107 · doi ↗ · pubmed ↗
- 5Businelle, M. S. , M. R. Apperson , D. E. Kendzor , M. A. Terlecki , and A. L. Copeland . 2008. “The Relative Impact of Nicotine Dependence, Other Substance Dependence, and Gender on Bechara Gambling Task Performance.” Experimental and Clinical Psychopharmacology 16, no. 6: 513–520.19086772 10.1037/a 0013510 · doi ↗ · pubmed ↗
- 6Calella, P. , G. Cerullo , M. Di Dio , et al. 2022. “Antioxidant, Anti‐Inflammatory and Immunomodulatory Effects of Spirulina in Exercise and Sport: A Systematic Review.” Frontiers in Nutrition 9: 1048258.36590230 10.3389/fnut.2022.1048258 PMC 9795056 · doi ↗ · pubmed ↗
- 7Chalabianloo, F. , L. T. Fadnes , K. A. Johansson , et al. 2024. “Methadone Pharmacokinetics in Opioid Agonist Treatment: Influencing Factors and Clinical Implications.” Basic and Clinical Pharmacology and Toxicology 134, no. 3: 333–344.38124280 10.1111/bcpt.13975 · doi ↗ · pubmed ↗
- 8Cheng, C.‐M. , Y.‐C. Lin , and K.‐C. Chang . 2017. “Psychological Distress Is Correlated With Erectile Dysfunction Among Patients Receiving Methadone Maintenance in Taiwan.” Journal of Dual Diagnosis 13, no. 4: 312–316.29120281 10.1080/15504263.2017.1363449 · doi ↗ · pubmed ↗