Prevalence, Clinical Profile, and Outcomes of Ectopic Pregnancy at a Teaching Hospital in a Low‐Resource Setting, Northern Ethiopia: A 5‐Year Retrospective Chart Review
Hale Teka, Mohamedawel Mohamedniguss Ebrahim, Mohammedtahir Yahya, Bisrat Tesfay Abera, Ephrem Berhe, Hiluf Ebuy Abraha, Fanos Gebru, Awol Yemane

TL;DR
This study examines ectopic pregnancy cases in a low-resource hospital in Ethiopia over five years, highlighting its prevalence, patient characteristics, and treatment outcomes.
Contribution
The study provides a detailed clinical profile and outcomes of ectopic pregnancies in a low-resource setting in Ethiopia.
Findings
Ectopic pregnancy prevalence was 6.58 per 1000 deliveries at the hospital.
Most cases required surgical management, with salpingectomy being the most common procedure.
Early detection and better reproductive health services are recommended to reduce complications.
Abstract
Ectopic pregnancy remains a significant cause of maternal morbidity and mortality worldwide, particularly in low‐resource settings. The aim of this study was to investigate the prevalence, clinical profile, and management outcomes of ectopic pregnancies at Ayder Comprehensive Specialized Hospital (ACSH) in Ethiopia between January 1, 2017 and December 31, 2021. A cross‐sectional study of 152 women diagnosed with ectopic pregnancy and admitted to ACSH between 2017 and 2021 was conducted. Data, including sociodemographic characteristics, obstetric history, clinical presentation, diagnostic methods, intraoperative findings, and management outcomes, were collected retrospectively from medical records. The prevalence of ectopic pregnancy was calculated based on the total number of deliveries during the study period. Descriptive statistics were used to summarize the data. Of 23,090…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
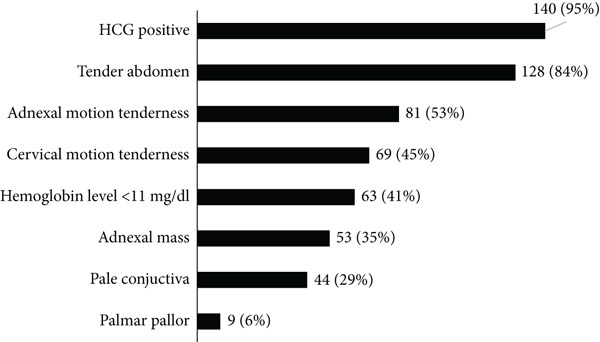 Figure 1
Figure 1|
|
|
|
|---|---|---|
| Region | ||
| Tigray | 146 (96.05) | 91.44–98.23 |
| Others (Afar and Amhara) | 6 (3.95) | 1.77–8.56 |
| Residence | ||
| Rural | 119 (78.3) | 70.97–84.2 |
| Urban | 33 (21.7) | 15.8–29.03 |
| Age category (years) | ||
| ≤ 24 | 35 (23.03) | 16.9–30.45 |
| 25–34 | 89 (55.5) | 50.5–66.17 |
| 35 and above | 28 (18.4) | 12.9–25.4 |
|
|
|
|
|---|---|---|
| Gravidity | ||
| One | 35 (23.03) | 16.97–30.45 |
| 2–4 | 89 (58.55) | 50.5–66.17 |
| 5 and above | 28 (18.42) | 12.99–25.45 |
| Parity | ||
| Zero | 51 (33.55) | 26.45–41.49 |
| One | 40 (26.32) | 19.88–33.95 |
| 2–4 | 53 (34.87) | 27.67–42.84 |
| 5 and above | 8 (5.26) | 2.64–10.22 |
| Abortion | ||
| Yes | 43 (28.29) | 21.65–36.02 |
| No | 109 (71.71) | 63.98–78.35 |
| Prior history of ectopic pregnancy | ||
| Yes | 10 (6.58) | 3.56–11.85 |
| No | 142 (93.42) | 88.15–96.44 |
| Gynecologic surgery | ||
| Yes | 14 (9.27) | 5.54–15.1 |
| No | 137 (90.73) | 84.9–94.46 |
| Type of gynecologic surgery ( | ||
| Salpingectomy | 8 (57.14) | 29.34–81.07 |
| Salpingostomy | 2 (14.29) | 3.1–46.46 |
| Laparotomy | 2 (14.29) | 3.1–46.6 |
| Bilateral tubal ligation | 1 (7.14) | 0.81–41.99 |
| MVA | 1 (7.14) | 0.81–41.99 |
| Abdominal surgery | ||
| Yes | 4 (2.65) | 0.99–6.9 |
| No | 147 (97.35) | 93.1–99.01 |
| Prior history of STD/STI | ||
| Yes | 12 (7.89) | 4.52–13.44 |
| No | 140 (92.11) | 86.56–95.48 |
| Multiple sexual partner | ||
| Yes | 11 (7.24) | 4.03–12.65 |
| No | 141 (92.76) | 87.35–95.97 |
| Contraceptive use | ||
| Yes | 29 (19.08) | 13.56–26.17 |
| No | 123 (80.92) | 73.83–86.44 |
| Type of contraceptive use ( | ||
| OCP | 3 (10.34) | 3.2–28.69 |
| Implant | 4 (13.79) | 5.04–32.53 |
| Injectables | 11 (37.93) | 21.82–57.24 |
| Postpil | 10 (34.48) | 19.12–53.95 |
| BTL | 1 (3.45) | 0.44–22.31 |
| Knew her current pregnancy | ||
| Yes | 81 (53.19) | 45.28–61.13 |
| No | 71 (46.71) | 38.87–54.72 |
| ANC contact | ||
| Yes | 16 (10.53) | 6.52–16.55 |
| No | 136 (89.47) | 83.45–93.48 |
|
|
|
|
|---|---|---|
| Diagnosis method | ||
| Clinical | 7 (4.61) | 1.7–2.2 |
| Ultrasound | 5 (3.29) | 1.45–7.71 |
| Clinical plus ultrasound | 135 (88.82) | 82.69–92.96 |
| Intraoperative diagnosis | 5 (3.29) | 1.37–7.71 |
| Heterotopic pregnancy | ||
| Yes | 7 (4.61) | 2.2–9.4 |
| No | 145 (95.39) | 90.6–97.8 |
| Management | ||
| Medical | 1 (0.66) | 0.09–4.49 |
| Surgical | 140 (92.11) | 86.56–95.48 |
| Medical plus surgical | 11 (7.24) | 4.03–12.65 |
| Site of ectopic pregnancy | ||
| Right tubal | 87 (57.24) | 49.19–64.92 |
| Left tubal | 63 (41.45) | 33.83–49.5 |
| Ovarian | 1 (0.66) | 0.09–4.59 |
| Abdominal | 1 (0.66) | 0.09–4.59 |
| If tubal site | ||
| Ampulla | 103 (68.67) | 60.75–75.63 |
| Isthmus | 8 (5.33) | 2.67–10.36 |
| Fimbriae | 34 (22.67) | 16.62–30.11 |
| Cornual | 5 (3.33) | 1.38–7.81 |
| Pelvic adhesion | ||
| Yes | 59 (38.82) | 31.35–46.85 |
| No | 93 (61.18) | 53.15–68.65 |
| Contralateral tube | ||
| Healthy | 129 (84.87) | 78.20–89.77 |
| Adhered/buried | 23 (15.13) | 10.23–21.8 |
| Ectopic type | ||
| Acute | 121 (79.61) | 72.39–85.32 |
| Chronic | 31 (20.39) | 14.68–27.61 |
| Postoperative complications | ||
| Yes | 2 (1.32) | 0.33–5.19 |
| No | 149 (98.68) | 94.81–99.67 |
| Type of procedure ( | ||
| Salpingectomy | 140 (92.72) | 87.75–96.07 |
| Salpingostomy | 4 (2.65) | 0.90–6.17 |
| Milking | 5 (3.31) | 1.27–7.10 |
| Salpingoopherectomy | 1 (0.66) | 0.07–3.05 |
| Omentectomy | 1 (0.66) | 0.07–3.05 |
| Was she transfused | ||
| Yes | 45 (29.61) | 22.84–37.4 |
| No | 107 (70.39) | 62.6–77.16 |
| Number of blood units | ||
| One | 3 (6.67) | 2.10–19.24 |
| Two | 20 (44.44) | 30.41–59.42 |
| Three and above | 22 (48.69) | 34.4–63.57 |
| ICU admission | ||
| Yes | 2 (1.32) | 0.33–5.16 |
| No | 150 (98.68) | 94.84–99.67 |
| Length of stay in hospital | ||
| ≤7 days | 138 (90.79) | 84.99–94.99 |
| 7 days and above | 14 (9.21) | 5.51–15.01 |
| Mean (SD) | 4.22 (±0.23) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEctopic Pregnancy Diagnosis and Management · Reproductive Health and Contraception · Appendicitis Diagnosis and Management
1. Introduction
An ectopic pregnancy is defined as the implantation of a fertilized ovum outside the uterine cavity, usually in the fallopian tubes [1]. It is a life‐threatening condition and a significant cause of maternal morbidity and mortality [2]. Globally, ectopic pregnancies account for approximately 1%–2% of all reported pregnancies [3]. However, the incidence varies due to different risk factors and access to health care in different populations and settings [4].
In high‐income countries, advances in diagnostics, such as transvaginal ultrasonography and sensitive human chorionic gonadotropin (hCG) testing, have facilitated the early detection of ectopic pregnancies [5, 6]. This has led to improved management options, including medical therapy with methotrexate, and reduced morbidity and mortality associated with this condition [7]. Conversely, in low‐income countries, however, limited access to healthcare services, lack of diagnostic facilities, and delayed presentation contribute to higher morbidity and mortality rates [8].
Ectopic pregnancy is still one of the main causes of pregnancy‐related deaths in low‐income countries. In sub‐Saharan Africa, ectopic pregnancy is estimated to be responsible for up to 10% of maternal deaths [9]. The clinical presentation often includes abdominal pain, vaginal bleeding, and amenorrhea, but symptoms can be nonspecific, leading to delays in diagnosis [10]. Complications such as tubal rupture and hemorrhagic shock are more common in low‐resource settings due to delayed diagnosis and treatment [11].
In Ethiopia, the burden of ectopic pregnancy is exacerbated by challenges such as limited access to reproductive health services, low utilization of antenatal care (ANC) and inadequate emergency obstetric care [12]. Cultural factors, socioeconomic barriers, and lack of awareness contribute to delayed healthcare‐seeking behavior among women [13]. Studies have shown that ectopic pregnancies are a significant cause of maternal morbidity and mortality in Ethiopia [14, 15].
Despite their importance, there is limited data on the epidemiology and management outcomes of ectopic pregnancies in Ethiopia, particularly in the Tigray region. Understanding the patterns of ectopic pregnancies, associated risk factors and management outcomes is critical for developing strategies to improve maternal health services. The aim of this study was to assess the prevalence, clinical presentation and management outcomes of ectopic pregnancies at Ayder Comprehensive Specialized Hospital (ACSH) in Ethiopia. By identifying gaps and challenges in the current management of ectopic pregnancy, the study aims to inform policy and practice to improve maternal health services in the region.
2. Methods
2.1. Study Area, Study Period, and Study Design
This study was conducted at Ayder Comprehensive Specialized Hospital (ACSH), one of the largest tertiary hospitals in the Tigray region of Ethiopia. The hospital serves over 300,000 patients annually, primarily from the Tigray region, with a smaller proportion from neighboring districts in the Amhara and Afar regional states. Each year, it records an average of 5000 deliveries. However, ACSH does not have a dedicated obstetric ICU or high‐dependency unit, resulting in obstetric cases being admitted to the limited medical and surgical ICUs. The research employed a cross‐sectional design, covering the period from January 1, 2017 to December 31, 2021.
2.2. Study Population and Sample Size
This study was conducted among 152 women diagnosed with ectopic pregnancy and consecutively admitted to ACSH from 2017 to 2021.
2.3. Study Variables and Source of Data
Data related to sociodemographic characteristics, obstetric history, signs and symptoms, laboratory investigation results, diagnosis methods, site of ectopic pregnancy, type of ectopic pregnancy, intraoperative and postoperative management, and length of hospital stay were retrospectively collected by reviewing medical records of the 152 ectopic pregnancy cases.
2.4. Data Collection Procedure
As an entry point to access patient charts, the hospital’s electronic medical record system, as well as the emergency room, inpatient wards, and operating theatre registers, were consulted. Moreover, additional entries were looked into maternal near‐miss and maternal death registries. Once the entries were collected, patient charts were retrieved from the archives room. Using a structured and pretested questionnaire, data were collected by trained obstetrics and gynecology specialists. EpiData 4.6 was used as data entry software to maintain skip logic, data consistency, typing error, and ease data export to statistical software.
2.5. Data Analysis
Data were exported to STATA 16 for analysis. Categorical variables are described using frequency, percent with its 95% confidence interval, and graphs. Continuous variables are described using an appropriate combination of measure of central tendency and measure of dispersion.
2.6. Ethical Considerations
Ethical approval was obtained from the Institutional Review Board (IRB) (MU‐IRB 1950/2022) of Mekelle University, College of Health Sciences. This was part of a large maternal near‐miss and mortality research project conducted in ACSH. Permission for data collection was obtained from the Chief Clinical Director (CCD) of ACSH. Informed consent was not required as we used secondary data. Patient charts were accessed and reviewed from May 1, 2022 to June 30, 2022.
3. Results
3.1. Prevalence of Ectopic Pregnancy
During the study period from 2017 to 2021, there were a total of 23,090 deliveries at ACSH. A total of 152 cases of ectopic pregnancy were recorded, resulting in a prevalence of 6.58 per 1000 deliveries.
3.2. Sociodemographic Variables
The mean age of the study participants was 28 years (SD = 0.5). More than half (55.5%) belong to the age group 25 to 34 years. Almost all (96.1%) of them were from Tigray regional state of Ethiopia. Majority of women (78.3%) were from rural area (Table 1).
3.3. Obstetric History
Primigravida, multigravida, and grand multigravida accounted for 35 (23.0%), 89 (58.6%), and 28 (18.4%) cases of ectopic pregnancy, respectively. One‐third (33.5%) of women with ectopic pregnancy were nulliparous and the rest were primiparous (26.3%), multiparous (34.9%), and grand multiparous (5.3%). History of abortion was recorded in 43 (28.3%) of them. A history of ectopic pregnancy was reported in 10 (6.6%) of the cases. Fourteen (9.3%) of the women had undergone gynecologic surgery, with the most common type of gynecologic surgery being salpingectomy/salpingostomy (10/14, 71.4%). Four patients had a history of abdominal surgery. A history of STI/STD and multiple sexual partners were reported in 12 (7.9%) and 11 (7.2%) of the patients, respectively. Of the women with an ectopic pregnancy, 81 (53.2%) were aware of their current pregnancy and only 16 (10.5%) of them had an ANC contact (Table 2).
3.4. Signs, Symptoms, and Laboratory Investigation Results During Admission
The most common physical examination findings on arrival were tender abdomen (128, 84%), adnexal motion tenderness (81, 53%), cervical motion tenderness (69, 45%), and pale conjuctiva (44, 29%). Hemoglobin level below 11 mg/dL was detected in 63 (41%) of the cases. HCG was positive in 140 (95%) of the cases (Figure 1).
Clinical profile of women diagnosed to have ectopic pregnancy and were admitted to ACSH from 2017 to 2021 (N = 152).
3.5. Diagnosis, Intraoperative Finding, and Management
Regarding the method of diagnosis, 135 (88.8%) of the cases were diagnosed both clinically and by ultrasound. The rest were diagnosed only clinically (4.6%), intraoperatively (3.3%), and only by ultrasound (3.3%). Heterotopic pregnancy was diagnosed in seven (4.6%) patients. The most common management was surgical only (92.1%), followed by medical–surgical (7.2%). Most (57.2%) of ectopic pregnancies occurred in the right tube. Ectopic pregnancies in the ovaries and in the abdomen occurred once each. Of the ectopic pregnancies that occurred in the fallopian tube, 103 (68.7%) were in the ampulla and 34 (22.7%) in the fimbriae. Pelvic adhesions were found in 59 (38.8%) of the cases. An adhered/spilled contralateral fallopian tube was found in 23 (15.1%) patients. About 80% of ectopic pregnancies were of the acute type. Salpingectomy and salpingostomy were performed in 141 (92.8%) and four (2.6%) of ectopic pregnancies, respectively. Blood transfusion was necessitated/carried out for 45 (29.6%) patients. Two patients were admitted to the intensive care unit. The median length of hospital stay was 4 days (IQR = 2) (Table 3).
4. Discussion
The primary aim of this study was to evaluate the prevalence, clinical presentation, and management outcomes of ectopic pregnancies at ACSH over 5 years. Our results show that ectopic pregnancy continues to be a significant health problem in the region with a prevalence of 6.58 (95% CI, 5.5–7.7) per 1000 deliveries. This prevalence is within the range reported in other studies from low‐income countries but is lower than the global average of 1%–2% [3].
Comparatively, a study in Nigeria reported a prevalence of 9.2 per 1000 deliveries [16], while a study in Ethiopia’s Jimma University Medical Center found a prevalence of 6.3 per 1000 deliveries [17]. The similarity in prevalence rates suggests common risk factors and challenges across these settings.
Our study found that the average age of women with ectopic pregnancy was 28 years, with the majority (55.5%) aged between 25 and 34 years. This age distribution is consistent with worldwide data indicating that ectopic pregnancies commonly occur in women in the prime reproductive period [18, 19]. The high prevalence in this age group may be attributed to increased sexual activity, higher fertility rates, and cumulative exposure to risk factors such as sexually transmitted infections (STIs) and pelvic inflammatory disease [10].
A remarkable result is that 78.3% of the patients lived in rural areas. Rural residence is associated with delayed access to health care due to factors such as limited transportation, fewer health care facilities, and lower health literacy [20, 21]. This delay can lead to more severe outcomes, such as ruptured ectopic pregnancies requiring emergency surgical interventions [22].
Regarding obstetric history, 58.6% of the women were multigravida and 28.3% had had an abortion. Previous abortions and ectopic pregnancies are known risk factors for possible tubal damage or scarring [23, 24]. The fact that 9.3% of patients had undergone previous gynecological surgery further emphasizes the role of tubal pathology in the risk of ectopic pregnancy. The low rate of ANC utilization (10.5%) is concerning. ANC contacts are crucial for the early detection of pregnancy complications [25]. Low utilization of ANC may be due to cultural beliefs, financial constraints or lack of awareness [13, 21]. Improving ANC services and encouraging early attendance could facilitate timely diagnosis and treatment of ectopic pregnancies.
Clinically, most patients presented with acute symptoms suggestive of ectopic pregnancy, such as abdominal tenderness and adnexal motion tenderness. The high incidence of anemia (hemoglobin < 11 mg/dL) in 41% of patients indicates significant blood loss likely due to tubal rupture [22]. This finding emphasizes the severity of the clinical picture and the need for immediate management. Diagnosis was made primarily on the basis of clinical assessment and ultrasound (88.8%). While ultrasound is a valuable tool, its effectiveness depends on the availability of equipment and qualified personnel [26]. In resource‐limited settings, reliance on clinical signs and symptoms remains essential [27]. The identification of heterotopic pregnancy in 4.6% of cases is noteworthy as this is a rare condition with significant diagnostic challenges [28].
Surgical treatment was the mainstay of treatment, with salpingectomy performed in 92.8% of cases. This high rate reflects the late presentation and severity of the cases [29]. In contrast, drug treatment with methotrexate is more common in stable patients in high‐income countries [30, 31]. Moreover, the need for blood transfusions in 29.6% of patients underscores the late presentation of significant number of patients, the severity of the bleeding, and the resource burden on healthcare facilities [32, 33]. Ensuring the availability of safe blood products is crucial for the management of such emergencies.
Pelvic adhesions were found in 38.8% of patients, indicating a history of pelvic infection or previous surgery [34]. Adhesions can impair fallopian tube function and increase the risk of future ectopic pregnancies [35].
4.1. Strengths and Limitations
A strength of this study is the comprehensive analysis of ectopic pregnancy cases over 5 years in a large tertiary care hospital, providing valuable insights into the epidemiology and management in a resource‐poor setting. However, limitations include the retrospective design, which may be subject to information bias due to incomplete medical records. In addition, results from a single institution may not be generalizable to other regions.
5. Conclusions
With a prevalence of 6.58 per 1000 deliveries, ectopic pregnancy remains an important health problem in the Tigray region. Most patients presented acutely and required surgical treatment. The high prevalence among women from rural areas underlines the need for improved access to reproductive health services and early detection mechanisms. Strengthening the health care infrastructure, improving the training of health care providers, and promoting awareness among the population are key strategies to address the challenges associated with ectopic pregnancy in Ethiopia. Future research should focus on prospective studies to evaluate interventions aimed at reducing the incidence of ectopic pregnancy and improving outcomes.
NomenclatureANCantenatal careBTLbilateral tubal ligationCIconfidence intervalhCGhuman chorionic gonadotropinICUintensive care unitMVAmanual vacuum aspirationOCPoral contraceptive pillsSTD/STIsexually transmitted disease/infection
Conflicts of Interest
The authors declare no conflicts of interest.
Author Contributions
- •Conceptualization and study design: Hale Teka, Mohammedtahir Yahya
- •Data collection: Mohammedtahir Yahya, Bisrat Tesfay, Ephrem Berhe, Fanos Gebru, Awol Yemane
- •Data analysis and interpretation: Hale Teka, Mohamedawel Mohamedniguss Ebrahim
- •Methodology development: Bisrat Tesfay, Ephrem Berhe, Hiluf Ebuy Abraha
- •Manuscript writing – original draft: Hale Teka, Mohamedawel Mohamedniguss Ebrahim, Hiluf Ebuy Abraha, Awol Yemane
- •Project administration: Hale Teka
- •Manuscript review and editing: All authors
Funding
No funding was received for this manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Barnhart K. T. , Clinical Practice. Ectopic Pregnancy, New England Journal of Medicine. (2009) 361, no. 4, 379–387, 10.1056/NEJ Mcp 0810384, 2-s 2.0-67651177703, 19625718.19625718 · doi ↗ · pubmed ↗
- 2Creanga A. A. , Shapiro-Mendoza C. K. , Bish C. L. , Zane S. , Berg C. J. , and Callaghan W. M. , Trends in Ectopic Pregnancy Mortality in the United States: 1980-2007, Obstetrics and Gynecology. (2011) 117, no. 4, 837–843, 10.1097/AOG.0b 013e 3182113 c 10, 2-s 2.0-79953194482, 21422853.21422853 · doi ↗ · pubmed ↗
- 3Murray H. , Baakdah H. , Bardell T. , and Tulandi T. , Diagnosis and Treatment of Ectopic Pregnancy, CMAJ. (2005) 173, no. 8, 905–912, 10.1503/cmaj.050222, 2-s 2.0-27144477401, 16217116.16217116 PMC 1247706 · doi ↗ · pubmed ↗
- 4Sivalingam V. N. , Duncan W. C. , Kirk E. , Shephard L. A. , and Horne A. W. , Diagnosis and Management of Ectopic Pregnancy, Journal of Family Planning and Reproductive Health Care. (2011) 37, no. 4, 231–240, 10.1136/jfprhc-2011-0073, 2-s 2.0-81055147674, 21727242.21727242 PMC 3213855 · doi ↗ · pubmed ↗
- 5Kirk E. , Papageorghiou A. T. , Condous G. , Tan L. , Bora S. , and Bourne T. , The Diagnostic Effectiveness of an Initial Transvaginal Scan in Detecting Ectopic Pregnancy, Human Reproduction. (2007) 22, no. 11, 2824–2828, 10.1093/humrep/dem 283, 2-s 2.0-40849085237, 17855406.17855406 · doi ↗ · pubmed ↗
- 6Crochet J. R. , Bastian L. A. , and Chireau M. V. , Does this Woman have an Ectopic Pregnancy?: The Rational Clinical Examination Systematic Review, Journal of the American Medical Association. (2013) 309, no. 16, 1722–1729, 10.1001/jama.2013.3914, 2-s 2.0-84876584553, 23613077.23613077 · doi ↗ · pubmed ↗
- 7Lipscomb G. H. , Medical Therapy for Ectopic Pregnancy, Seminars in Reproductive Medicine. (2007) 25, no. 2, 93–98, 10.1055/s-2007-970048, 2-s 2.0-33947588310, 17377896.17377896 · doi ↗ · pubmed ↗
- 8Jurkovic D. and Wilkinson H. , Diagnosis and Management of Ectopic Pregnancy, BMJ. (2011) 10, no. 342, d 3397, 10.1136/bmj.d 3397, 2-s 2.0-84858998688, 21665933.21665933 · doi ↗ · pubmed ↗