Racial and Socioeconomic Healthcare Disparities in Access to Chimeric Antigen Receptor T (CAR‐T) Cell Therapy for Blood Cancers
Hasini Warnakulasuriya, Ritika Tiwari

TL;DR
The paper examines how race and socioeconomic factors affect access to CAR-T therapy for blood cancers and suggests policy changes to reduce these disparities.
Contribution
The study systematically maps racial and socioeconomic disparities in CAR-T therapy access and proposes targeted policy solutions.
Findings
Financial constraints, lack of insurance, and systemic biases limit CAR-T therapy access for minority and low-income groups.
Minority populations are underrepresented in CAR-T clinical trials, contributing to inequitable treatment outcomes.
High treatment costs and lack of awareness further widen disparities in CAR-T accessibility.
Abstract
Health disparities remain a critical global public health challenge, particularly in access to advanced treatments for blood cancers. Racial and socioeconomic factors influence healthcare accessibility, contributing to inequities in patient outcomes. Despite the potential of CAR‐T therapy in treating blood cancers, disparities in financial resources, education, gender, and race hinder equitable access. This study evaluates literature on CAR‐T therapy to identify access disparities and proposes policy recommendations. The PRISMA‐ScR guidelines were followed for study selection and reporting. A comprehensive search strategy was used across databases like PubMed and Google Scholar, using keywords and MeSH terms. Inclusion criteria included peer‐reviewed studies in English since 2000. A basic quality appraisal was conducted to ensure the relevance and credibility of included studies,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
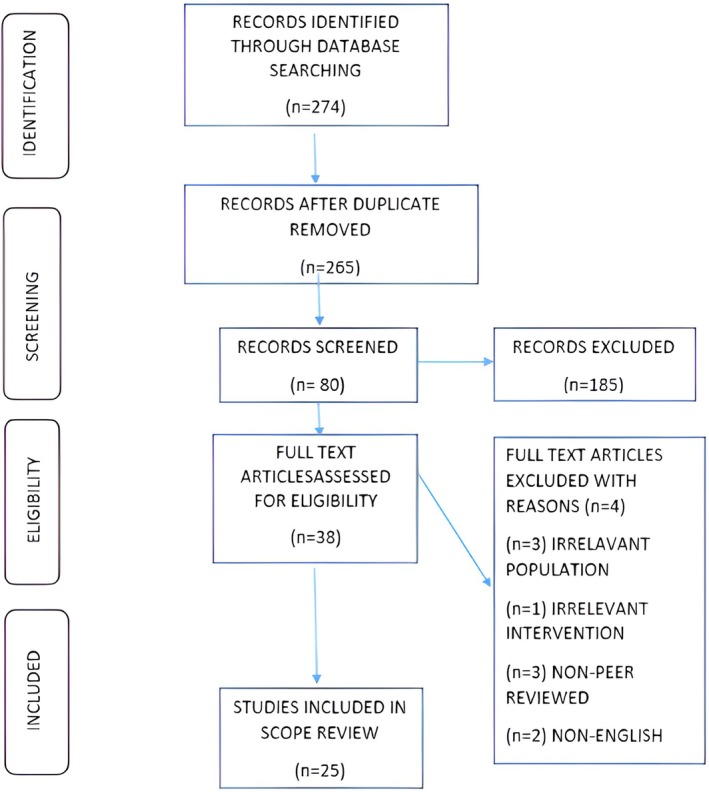 FIGURE 1
FIGURE 1| Theme/findings | Citation | Study type | Setting |
|---|---|---|---|
| Negative impacts of socioeconomic and racial imparities in health | National Research Council (US) [ | Book chapter | — |
| Education disparity in blood cancer related care in health sector |
Jibu et al. [ Montez and Cheng [ |
Cross sectional study Cross‐sectional study |
Online questionnaire, Chennai, India USA |
| Minorities and worst health outcome and impact of education |
Egede [ Cutler and Lleras‐Muney [ |
Editorial Quantitative analysis |
— USA |
| Influence of racial differences in health care | Williams and Sternthal [ | Literature review | USA |
| Impact of financial disparity | Jaeggi et al. [ | Observational analytical study | Tsimane, Bolivia |
| Financial and other socioeconomic disparities lead to unhealthy behavior. | Pampel et al. [ | Literature review | USA |
| Gender disparity | Mirin [ | Quantitative analysis | USA |
| Prevalence and insight of the severity of blood cancer | Siegel et al. [ | Descriptive study | USA |
| Racial and ethnic minorities affect cancer largely | Kirtane and Lee [ | Literature review | USA |
| Main blood cancer incidences in minorities | Kirtane and Lee [ | Literature review | USA |
| Prevalence of blood cancer, diagnosis and prognosis |
Howell et al. [ Chu et al. [ |
Qualitative study Experimental study |
UK China |
| Blood cancer prevalence in Hispanics, blacks and Asian/pacific islanders |
Bencomo‐Alvarez et al. [ Sheppard et al. [ Pang et al. [ Beale [ |
Commentary Descriptive study ( Cohort study (Asians and White) Commentary |
USA USA USA USA |
| Importance of CAR‐T cell therapy to treat blood cancer |
Morotti et al. [ De Marco et al. [ Sterner and Sterner [ Zhang et al. [ |
Literature review Literature review Literature review Book chapter |
USA — — USA |
| Disparities in CAR‐T cell therapy and future of the therapy |
Ahmed et al. [ Hall et al. [ Yamamoto et al. [ Bell et al. [ |
Cohort study Cohort study Analytical study Perspective study |
USA USA Japan, USA USA |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCAR-T cell therapy research · Biomedical Ethics and Regulation · Economic and Financial Impacts of Cancer
Introduction
1
Health Disparities
1.1
Health disparities are differences in health outcomes among particular groups. Differences in disease incidence, prevalence, mortality, and severity can be used to quantify these disparities [1].
In recent years, growing health disparities have become a global concern, particularly posing a huge threat to public health. Data suggests that social determinants of health such as the conditions in which people live, work, and learn can quickly change a society and impact the well‐being of society [1]. These determinants are the underlying cause of health disparities. The unequal distribution of resources, power, and wealth affects these variables, which could impact the disease incidence, access to care and mortality rate [2].
Socioeconomic Disparities
1.2
It is believed that socioeconomic disparities have a negative influence on the health outcomes of numerous illnesses according to the research [3] since these can prevent patients from receiving the full benefits of successful treatments as stated by the research [4] resulting in loss of functionality, physical and cognitive impairments, and even increased mortality rates. Public health is greatly impacted by racial and ethnic disparities since people from different ethnic backgrounds do not access healthcare services equitably [3]. Many studies have been conducted to determine the underlying causes of these disparities and create more equitable healthcare policies because of the wide discussion of these issues throughout history. Although there has been progress in narrowing these gaps, there is still much to be done to eliminate racial and ethnic disparities in healthcare [5]. Minority groups continue to receive lower‐quality healthcare than non‐minorities, despite the availability of advanced treatment options; this leads to worse health outcomes [6].
Financial Disparities
1.3
Financial disparities exacerbate health inequalities by limiting access to high‐quality healthcare [4]. Stressful living conditions and poor health outcomes are frequently caused by lower socioeconomic status. However, financial instability is not the only reason for some people to avoid medical care.
In addition to socioeconomic and racial disparities, health disparities can also stem from differences in gender, age, disability, and geographical factors [5].
Educational Disparities
1.4
While lower educational levels are linked to worse health outcomes, higher educational attainment is linked to improved health outcomes [7]. It also has an impact on behaviors like smoking and poor diet [8]. Disparities in education result in a lack of awareness of diseases, their symptoms, progression, and treatments. Health outcomes may deteriorate because of this ignorance, which is often aggravated by a lack of access to reliable information and social stigma. For instance, greater survival rates are associated with cancer awareness, but a lack of awareness lowers the possibility of a successful course of therapy [9]. Despite the effectiveness of CAR‐T cell therapy, many individuals cannot access it simply because they lack knowledge about the treatment.
Gender Disparities
1.5
Gender imbalance in healthcare is a critical concern, especially for women, who encounter more acute healthcare inequities. The undervaluation of women's health in society often results in delayed care and adverse health outcomes [10]. Particularly, women from underprivileged socioeconomic and racial backgrounds receive low‐quality treatment. These disparities can take many forms, including underrepresentation in studies, delayed diagnosis, and a disregard for women's health issues, which are frequently attributed to psychological reasons [10].
Blood Cancers and Treatment Methods
1.6
Hematologic malignancies which are also called blood cancers, such as leukemia, lymphoma, and multiple myeloma, originate from blood or lymphatic tissues and may be lethal [11]. With over 100 subtypes and different causes, blood malignancies rank fifth among all cancer forms in developed countries. Although intense treatment can cure some blood cancers, only 40% of them have the potential to be cured, and 60% of those can be fatal [12]. Early diagnosis is difficult due to the gradual onset of symptoms, which often appear as signs of other illnesses [12].
The course of treatment for blood cancers varies according to the type of cancer, patient age, metastasis, and progression. Surgery, chemotherapy, and radiotherapy are examples of conventional treatments; chemotherapy is frequently used as a first line of treatment. However, these therapies frequently have serious adverse effects, such as extended recovery periods and damage to healthy tissue [13].
Health Disparities and Blood Cancers
1.7
Health disparities include lower socioeconomic status, limited education, limited access to healthcare. Environmental factors are the main causes of cancer, which is also the top cause of death among Hispanics in the United States [14].
Approximately 60 million Hispanic people (18% of the US population) earn 30% less on average per year than non‐Hispanics. Hispanic children have the greatest incidence rates of leukemia (62.6 per million) compared to non‐Hispanic children (52.2 per million), making it the most prevalent blood cancer in this group [14]. Their five‐year survival rate is 90%, which is less than the 95% rate for white non‐Hispanic children. The prevalence of acute lymphoid leukemia (ALL) is higher among Hispanics than among other populations, and even with early detection, outcomes remain poorer [14]. Due to delayed care, lack of insurance, and restricted access to early treatments, Hispanics with Acute Promyelocytic Leukemia (APL), a curable form of acute myeloid leukemia, have a 5–10 year worse survival rate. Access to treatment is further restricted by the fact that 72% of Hispanics in the US do not have health insurance [14].
Black Americans have a 19% higher overall cancer rate than white Americans, making cancer the second most common cause of death for them [15]. Despite having the highest mortality and lowest survival rates, African Americans (AAs) are underrepresented in cancer research [15]. This underscores the need for AAs to participate more in cancer research to improve prevention and control.
The incidence of leukemia among U.S. Asians and foreign‐born Asian Americans is similar, suggesting a reduced risk relative to white populations [16]. Asians had the lowest rates of pediatric blood cancer, according to studies conducted in Europe and the UK, though the exact causes remain unknown [17]. Regardless of where they were born, Asians generally have the lowest prevalence of blood cancer; however, Asians born in the United States have slightly higher rates than Asians born outside [18].
According to projections, the United States' cancer rates will rise by 45% in the next 20 years, which could exacerbate the disparities in blood cancer among minorities, such as Asians and Pacific Islanders [19]. Socioeconomic factors contribute to these inequities, such as Pacific Islanders' lower insurance coverage. Delays in diagnosis, increased mortality, and decreased involvement in cancer research resulted from the increase in the percentage of people without insurance from 14.2% to 15.9% between 2000 and 2005 [19].
CAR‐T Cell Therapy
1.8
Cancer has emerged as a significant worldwide health threat, with a sharp rise in case incidence in recent years. Despite advancements in traditional treatment, managing those therapies remains complicated [20]. To decrease severe side effects, increase effectiveness, and raise survival rates, new treatments are required. Immunotherapy, a recent advancement, has shown significant promise. It uses immunological components, including cytokines, immune cells, and antibodies, to reduce cancer cells and minimize cytotoxic effects that damage healthy cells [13, 21].
Immunotherapy, including CAR‐T cell therapy, involves modified autologous T cells to specifically target and eliminate cancer cells while retaining healthy tissue. CARs improve T cells' capacity to recognize tumor antigens, which in turn triggers an immunological response [22].
Prior to reinfusion, a patient's T cells are extracted and modified to target cancer cells as part of CAR‐T therapy. To eliminate cancer, these cells identify tumor antigens and initiate cytotoxic reactions [13]. CAR‐T cell therapy selectively targets cancer cells, minimizing damage to healthy tissues, in contrast to chemotherapy, which may damage organs and have severe side effects [23].
The U.S. FDA approved two CAR‐T cell therapies for hematological malignancies, namely acute lymphoblastic leukemia and large B‐cell lymphomas. CAR‐T therapy has improved vastly over the last year, resulting in better clinical outcomes and longer remission periods [24].
Racial and Socioeconomic Disparities and CAR‐T Cell Therapy
1.9
Racial, ethnic, and socioeconomic disparities restrict the use of CAR‐T therapy, which offers hope to patients with blood cancer. Only 1% of African Americans and 5.4% of Hispanics participate in CAR‐T admissions, demonstrating the underrepresentation of minority groups in clinical trials [25]. Hispanic and Black patients with B‐cell lymphoma, multiple myeloma, and acute lymphoid leukemia are also impacted by barriers such as limited access, underrepresentation in trials, and language [26].
For low‐income minorities, transportation and related expenses create significant barriers because therapy requires regular visits to specialized clinics. Food, accommodation, and therapy management costs which are sometimes not covered by insurance, increase financial strain and increase the risk of relapses and adverse outcomes [27].
Improving healthcare access, particularly for CAR‐T cell therapy in blood cancers, requires addressing racial and socioeconomic disparities. These differences frequently result in lower health outcomes for socially disadvantaged communities. Future disparities can be avoided by identifying and addressing the underlying causes [28]. Racial and socioeconomic barriers still restrict access to CAR‐T therapy, which reduces the benefits for many patients despite medical improvements [5].
Resources have been stressed due to the increased demand for CAR‐T therapy, which has complicated patient selection and caused bias issues. For underprivileged populations, access and results could be increased by creating more medical centres and setting equitable frameworks in place [29]. This scoping review aims to map and synthesize existing evidence on racial and socioeconomic disparities in access to CAR–T cell therapy, an area critically underexplored despite its life‐saving potential.
Methodology
2
Guidelines Followed
2.1
This scoping review was conducted in accordance with established methodological frameworks, including the PRISMA‐ScR (Preferred Reporting Items for Systematic Reviews and Meta‐Analyses Extension for Scoping Reviews) guidelines (Table A1), to ensure transparency and reproducibility. The main research question was developed to examine the contemporary issue of socioeconomic and racial disparities in the accessibility of CAR‐T cell therapy for blood cancers. This question was designed to help focus the research and lead future studies into the causes, impacts, and possible solutions.
Eligibility Criteria
2.2
Inclusion Criteria
2.2.1
To ensure the inclusion of high‐quality, peer‐reviewed evidence, the inclusion criteria focused on English‐language literature published since 2000 including high‐quality editorials and commentaries published in academic journals and gray literature that specifically addressed racial and socioeconomic disparities in access to CAR‐T cell therapy for blood cancers.
Exclusion Criteria
2.2.2
The purpose of the exclusion criteria was to filter out research that was low‐quality, non‐peer reviewed or irrelevant. Studies on unrelated medical conditions or treatments have been excluded to keep the focus on CAR‐T cell therapy for blood cancers, and articles that were not published in English were excluded to ensure consistency in the study.
Data Sources
2.3
Data sources included widely used databases such as PubMed and Google Scholar, as well as gray literature and credible organization websites. The use of multiple sources facilitated comprehensive literature coverage, allowing for a thorough examination of racial and socioeconomic disparities in CAR‐T cell therapy accessibility.
Search Strategy
2.4
A systematic search strategy was applied to recognize relevant literature across multiple databases. Keywords and MeSH terms such as “health disparities,” “health equity,” “CAR‐T cell therapy,” and “blood cancers” were used to involve a wide range of appropriate studies. Boolean operators like “AND” “OR” and “NOT” enhanced search key strings for specificity. Examples included “health disparities” AND “CAR‐T cell therapy,” “health equity” AND “blood cancers,” and “CAR‐T cell therapy” NOT “solid tumors.” The search strategy was adapted to each database and documented to ensure reproducibility and transparency. The complete search strategy and corresponding outcomes are presented in Table A2.
PRISMA Flow Chart
2.5
The PRISMA flow chart visualizes the systematic study selection process, which includes study identification, screening, eligibility, and inclusion (Figure 1). This chart increased transparency and repeatability by ensuring that all relevant research was documented.
PRISMA flow chart: PRISMA flow diagram illustrating the study selection process for the scoping review. This flow diagram outlines the identification, screening, eligibility, and inclusion phases of the scoping review. A total of 274 records were initially identified through database searching. After removing duplicates, 265 records remained. Of these, 80 were screened, and 185 were excluded based on titles and abstracts. Full texts of 38 articles were assessed for eligibility, with 4 excluded for reasons including irrelevant population (n = 3), irrelevant intervention (n = 1), non‐peer‐reviewed sources (n = 3), and non‐English language (n = 2). Ultimately, 25 studies were included in the final review.
Screening Process
2.6
Titles and abstracts retrieved from database searches were screened against the predefined inclusion criteria. Full‐text articles of potentially relevant studies were then assessed for eligibility. No formal quality appraisal tool was used; however, a standardized data extraction form was employed to ensure consistency in capturing key study characteristics and emerging themes throughout the review process.
Quality Appraisal
2.7
A basic quality appraisal was carried out to assess the credibility and relevance of the included studies. Two simple tools were developed to correspond with different types of literature. For reviews, book chapters, editorials, and commentaries, the appraisal looked at aspects such as whether the purpose was clear, the author had relevant expertise, the content was supported by evidence, and how credible and useful the source was. For empirical studies including descriptive, analytical, and experimental studies, the appraisal focused on whether the study had clear inclusion criteria, an appropriate design, valid measurements, adequate sample size, control of confounding factors, and appropriate data analysis. Each item was scored as 1 (yes) or 0 (no), and the total score was used to rate the overall quality as high (5–6), moderate (3–4), or low (below 3). While no formal critical appraisal tool was used, this basic approach helped maintain consistency and transparency in evaluating the quality of the diverse sources included in the review. The results of the quality appraisal are presented in Tables A3, A4.
Data Synthesis and Extraction
2.8
Data synthesis involved charting and grouping extracted data to identify repeated themes related to disparities in access to CAR‐T cell therapy. Studies were grouped thematically, with primary themes including racial, financial, educational, and broader socioeconomic disparities. Additional contextual factors included healthcare system differences, insurance coverage, geographic location, and health literacy.
Analysis
2.9
A thematic content analysis approach was applied to explore these themes in depth. This process aimed to highlight disparities across ethnic and socioeconomic groups, identify contributing factors, and assess their implications for treatment access, outcomes, and patient well‐being.
Ethical Considerations
2.10
As this study involved only secondary data from published sources, all data were anonymized, and no personal health information was accessed. Furthermore, all included articles were properly cited in accordance with academic integrity standards. The article selection and analysis were conducted objectively and without bias, based solely on relevance and quality rather than author identity, institutional affiliation, or publication source.
Results
3
The key findings from the thematic analysis are presented in Table 1. A detailed summary of each article, including key findings and relevance, is provided in Table A5.
Articles from scientific databases such as PubMed, ScienceDirect and Nature were obtained to answer the knowledge gaps related to the research question of this report. After thorough investigation a total of 25 articles were selected to address the research aim and question. The duplicated and non‐English articles were excluded. Full text articles published since 2000 were selected. The selected articles and their findings, as presented in Table 1, were thematically categorized to address the key issues related to disparities in CAR‐T cell therapy access.
Several repeated factors contributing to health disparities were identified in the reviewed literature. Socioeconomic and racial disparities were regularly reported as major barriers to accessing CAR‐T cell therapy. Educational, financial, and gender‐related inequalities were also shown to intensify the gap in healthcare provision, especially among marginalized and minority populations. Ethnic and racial differences are contributing to health disparities in every country. Throughout the study, minority groups were identified and analyzed to understand the prevalent health disparities these minority groups are experiencing especially in the context of blood cancers.
The literature also highlighted the impact of disparities on treatment outcomes and the overall well‐being of individuals with blood cancers. This evidence is supported by several articles that outlined how disparities in CAR‐T cell therapy affect treatment outcomes and the overall patient experience. The socioeconomic disparities contributed by education, social status and financial disparities were shown to prevent patients from receiving the full benefit of these advanced treatments. Lack of knowledge of the CAR‐T cell treatment, financial inability to receive the treatment and racial or ethnic background are identified in the study as major health disparities in CAR‐T cell therapy access.
Several of the reviewed articles also proposed potential strategies and suggestions to minimize existing disparities in CAR‐T cell therapy. Minorities have low socioeconomic status, and it is negatively affecting them from receiving proper care for blood cancers. Therefore, policies that permit equitable access to each and every individual into care regardless of their racial and socioeconomic status need to be established. The individuals need to be granted accessible and affordable health care insurance to receive proper medication. The government also has to consider the families of the affected individuals and needs to prevent the economical, physical and psychological burden on them. Therefore, this study suggests the renewal and modification of existing policies and establishing newer policies that allow equitable access to CAR‐T cell therapy regardless of patient racial and socioeconomic status.
Discussion
4
Main Findings of This Study
4.1
CAR‐T cell therapy is an important cancer treatment, but health disparities limit access for underprivileged populations [36]. This article examines recent studies on racial and socioeconomic barriers to CAR‐T therapy. Minorities, particularly African Americans (AAs), are underrepresented in clinical trials, which limits obtaining the maximum health benefit from CAR‐T therapy. This gap highlights the need for greater minority involvement in trials to enhance health outcomes and improve the generalizability of clinical findings [4].
What Is Already Known on This Topic
4.2
Socioeconomic disparities restrict access to quality care. Financial, gender, and educational inequalities all contribute to these disparities. Low‐income populations have worse health outcomes because they cannot afford reliable medical care, whereas higher‐income populations have better access and outcomes [4]. Evidence shows that healthcare outcomes and access are impacted by one's position in the socioeconomic hierarchy, which defines one's relative access to resources [37].
Families may find it difficult to pay for CAR‐T cell therapy alongside other costs like food, accommodation, and travel, which could limit their ability to receive therapy. Relapses decrease survival rates, and worsened situations can result from this, which influences public health [27].
What This Study Adds
4.3
High mortality and low survival rates are indicators of insufficient healthcare, which has an impact on national politics and economics. These issues should be addressed in future initiatives, and collaboration will be necessary to discover effective solutions. In addition to ensuring that CAR‐T cell therapy treatments are cost‐effective, decision‐makers should advocate for insurance coverage of all associated expenses. To ensure equitable access to CAR‐T cell therapy, clinical practitioners need to develop strategies for equitable resource distribution that include eligible patients irrespective of race and socioeconomic backgrounds.
Limitations of This Study
4.4
This study has certain limitations. The exclusion of non‐English language studies may have omitted relevant international research. Additionally, reliance on published literature may introduce publication bias, as studies with statistically significant results are more likely to be published which were overcome by including gray literature.
Another limitation is that most of the included studies were conducted in the United States, a high‐income country according to the World Bank classification [38]. The significance of this is that even in a well‐resourced healthcare system, substantial socioeconomic and racial disparities in access to CAR‐T cell therapy persist. This highlights the likelihood that such disparities may be even more severe in low‐ and middle‐income countries (LMICs), where healthcare infrastructure, funding, and equitable access are more limited. Therefore, although the findings may not fully represent global contexts, they highlight universal challenges that are likely to exist and possibly be more severe, outside high‐income settings. This limitation may affect the generalizability of the findings and should be considered when interpreting the results.
The absence of data on African American involvement in CAR‐T cell therapy research is one of the study's limitations. However, it still provides important information on this minority group's access to CAR‐T cell therapy. Increasing AAs' engagement in CAR‐T cell therapy research must be one of the primary focuses of future studies, as it is essential for improving the generalizability of findings and ensuring equitable access to treatment [27].
Conclusion and Recommendations
5
This scoping review pinpoints important racial and socioeconomic inequities in access to CAR‐T cell therapy for patients with hematologic malignancies. These disparities limit timely diagnosis, clinical trial enrolment, and treatment access, especially among underprivileged groups.
The findings underscore the need for targeted policy reforms and strategic investments in equitable healthcare infrastructure. For example, studies [15] and [26] highlight the importance of establishing hospital‐based referral systems and community outreach programs to improve clinical trial participation among minority groups. Similarly, the study [25] emphasizes enrolling more underrepresented populations in CAR‐T trials to address racial and socioeconomic inequities and to ensure equitable access to CAR‐T therapy.
Future research should focus on inclusive recruitment strategies, socioeconomic considerations in healthcare delivery, and improved health literacy related to blood cancers, as noted by researchers [9] and [11]. Government‐led efforts, intersectoral collaboration, and the development of ethical frameworks for resource allocation as highlighted by the study [29] will be essential in ensuring that CAR‐T and other advanced therapies are accessible to all, regardless of race, ethnicity, or socioeconomic status.
Author Contributions
Hasini Warnakulasuriya: conceptualization (lead), methodology (lead), writing – original draft (lead). Ritika Tiwari: supervision (lead), validation (lead), writing – review and editing (lead).
Funding
The authors have nothing to report.
Ethics Statement
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1N. Kondo , “Socioeconomic Disparities and Health: Impacts and Pathways,” Journal of Epidemiology 22 (2012): 2–6, 10.2188/jea.je 20110116.22156290 PMC 3798573 · doi ↗ · pubmed ↗
- 2W. L. Macias‐Konstantopoulos , K. A. Collins , R. Diaz , et al., “Race, Healthcare, and Health Disparities: A Critical Review and Recommendations for Advancing Health Equity,” Western Journal of Emergency Medicine 24, no. 5 (2023): 906–918, 10.5811/westjem.58408.37788031 PMC 10527840 · doi ↗ · pubmed ↗
- 3National Research Council (US) , N. B. Anderson , R. A. Bulatao , and B. Cohen , Race/Ethnicity, Socioeconomic Status, and Health (National Academies Press (US), 2004), https://www.ncbi.nlm.nih.gov/books/NBK 25526/.
- 4A. V. Jaeggi , A. D. Blackwell , C. Rueden , et al., “Do Wealth and Inequality Associate With Health in a Small‐Scale Subsistence Society?,” e Life 10 (2021): e 59437, 10.7554/elife.59437.33988506 PMC 8225390 · doi ↗ · pubmed ↗
- 5National Academies of Sciences, Engineering, and Medicine, Health and Medicine Division, Board on Population Health and Public Health Practice, Committee on Community‐Based Solutions to Promote Health Equity United States , A. Baciu , Y. Negussie , A. Geller , and J. N. Weinstein , The State of Health Disparities in the United States (National Academies Press (US), 2017), https://www.ncbi.nlm.nih.gov/books/NBK 425844/.
- 6L. E. Egede , “Race, Ethnicity, Culture, and Disparities in Health Care,” Journal of General Internal Medicine 21 (2006): 667–669, 10.1111/j.1525-1497.2006.0512.x.16808759 PMC 1924616 · doi ↗ · pubmed ↗
- 7S. Khalatbari‐Soltani , J. Maccora , F. M. Blyth , C. Joannès , and M. Kelly‐Irving , “Measuring Education in the Context of Health Inequalities,” International Journal of Epidemiology 51 (2022): 701–708, 10.1093/ije/dyac 058.35362521 PMC 9189977 · doi ↗ · pubmed ↗
- 8F. C. Pampel , P. M. Krueger , and J. T. Denney , “Socioeconomic Disparities in Health Behaviors,” Annual Review of Sociology 36 (2010): 349–370, 10.1146/annurev.soc.012809.102529.PMC 316979921909182 · doi ↗ · pubmed ↗