Hepatosplenic Tuberculosis Mimicking Metastatic Malignancy and Immune Reconstitution Inflammatory Syndrome (IRIS) in an HIV-Positive Patient
João Pedro Maldonado, Vânia Almeida, Rubén Carvalho, Maria Augusta Cipriano

TL;DR
An HIV-positive man was diagnosed with liver and spleen tuberculosis, which initially resembled cancer or IRIS, through biopsy and PCR testing.
Contribution
This case emphasizes the importance of histopathology and PCR in diagnosing extrapulmonary TB in HIV patients.
Findings
Liver biopsy showed epithelioid granulomas with central necrosis, suggesting infection.
PCR confirmed Mycobacterium tuberculosis in the biopsy sample.
Anti-TB therapy with antiretroviral treatment improved the patient's condition.
Abstract
A man in his late 30s, recently diagnosed with HIV-1, presented with persistent fever, weight loss, and fatigue, despite prior treatment for immune reconstitution inflammatory syndrome (IRIS). Imaging studies revealed splenomegaly, hepatic and splenic micronodular lesions, and pulmonary micronodules. A liver biopsy, pivotal in establishing the diagnosis, demonstrated multiple well-formed epithelioid granulomas with focal central necrosis, indicative of an infectious etiology. Polymerase chain reaction (PCR) analysis of the biopsy fragment confirmed the presence of Mycobacterium tuberculosis. The integration of histopathological findings and PCR analysis was instrumental in diagnosing extrapulmonary tuberculosis (TB) involving the liver and spleen. The patient was started on anti-TB therapy in conjunction with continued antiretroviral treatment, resulting in significant clinical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
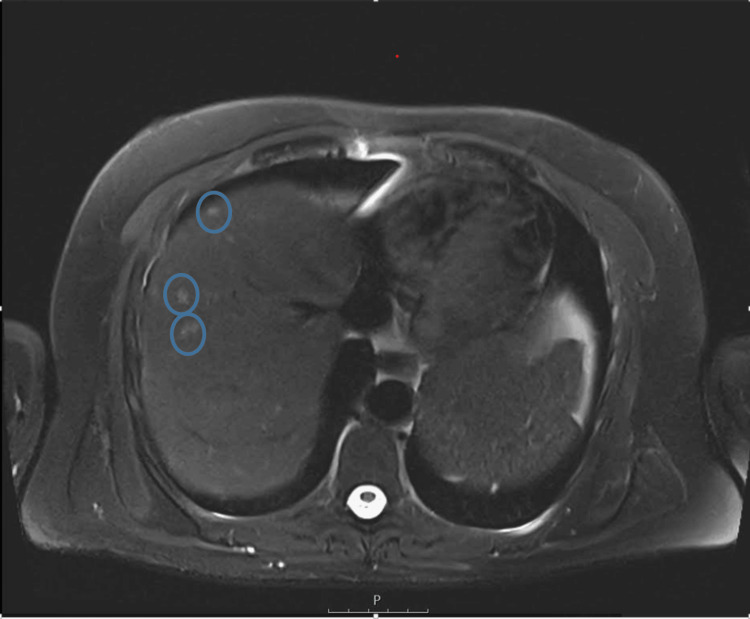 Figure 1
Figure 1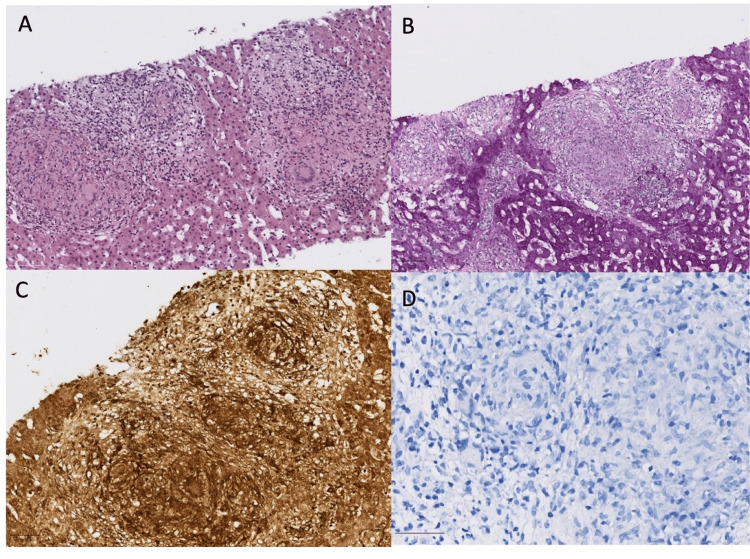 Figure 2
Figure 2| Parameter | Result | Normal range |
|---|---|---|
| Glucose | 224 mg/dL | 60-109 mg/dL |
| Urea nitrogen (Azoto uréico) | 14.8 mg/dL | 7.9-20.9 mg/dL |
| Creatinine | 1.10 mg/dL | 0.72-1.18 mg/dL |
| Sodium | 135 mmol/L | 136-146 mmol/L |
| Potassium | 4.5 mmol/L | 3.5-5.1 mmol/L |
| Total proteins | 7.3 g/dL | 6.6-8.3 g/dL |
| Calcium | 10.2 mg/dL | 8.8-10.6 mg/dL |
| Osmolality | 278 mOsm/kg | 260-302 mOsm/kg |
| LDH | 250 U/L | <248 U/L |
| AST (GOT) | 37 U/L | <35 U/L |
| ALT (GPT) | 51 U/L | <45 U/L |
| Alkaline phosphatase | 302 U/L | 30-120 U/L |
| GGT | 669 U/L | <55 U/L |
| Total bilirubin | 1.0 mg/dL | 0.2-1.2 mg/dL |
| Creatine kinase | 17.1 U/L | <171 U/L |
| C-reactive protein | 11.92 mg/dL | <0.50 mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiagnosis and treatment of tuberculosis · Infectious Diseases and Tuberculosis · Sarcoidosis and Beryllium Toxicity Research
Introduction
Extrapulmonary tuberculosis (TB), while less common than pulmonary TB, is a significant manifestation, particularly in immunocompromised individuals, such as those with HIV [1-3]. In Portugal, the incidence of TB was reported at 16 cases per 100,000 people in 2023 according to the World Health Organization (WHO) [4], highlighting the ongoing public health burden of the disease. Its presentation often mimics conditions like malignancies or fungal infections [1,5]. Nonspecific symptoms, including fever and weight loss, as well as systemic involvement, can obscure the diagnosis, particularly when routine diagnostic tests yield negative results. This case highlights the crucial role of an early liver biopsy in the diagnostic workup, enabling an accurate diagnosis and a timely initiation of appropriate therapy.
Case presentation
A man in his 30s, recently diagnosed with HIV (CD4+ count: 172 cells/μL), presented with a four-day history of fever reaching 39°C, muscle aches, fatigue, weight loss, and night sweats. Two months earlier, he had been hospitalized for a febrile illness thought to be associated with immune reconstitution inflammatory syndrome (IRIS) following the initiation of antiretroviral therapy (bictegravir 50 mg + emtricitabine 200 mg + tenofovir alafenamide 25 mg, once daily). His fever briefly resolved with corticosteroids (prednisolone) but recurred, accompanied by progressive anorexia and weight loss.
His medical history included type 2 diabetes mellitus, diagnosed several years prior, and gastroesophageal reflux disease. He lived with his spouse and reported no significant occupational or travel exposure. He denied any prior history of TB or known exposures. On physical examination, he exhibited considerable weight loss but had no lymphadenopathy, hepatosplenomegaly, ascites, or neurological deficits.
Initial laboratory results showed elevated inflammatory markers and liver enzymes (Table 1). Imaging studies, including abdominal magnetic resonance imaging (MRI), revealed multiple micronodules in the liver, spleen, and lungs, suggesting a disseminated disease process (Figure 1). Bronchoalveolar lavage and serological tests ruled out pathogens such as *Pneumocystis jirovecii *and Cytomegalovirus.
Axial T2-weighted MRI of the upper abdomen Axial T2-weighted MRI of the upper abdomen showing the liver with multiple hyperintense micronodular lesions scattered across both lobes
A targeted liver biopsy of the micronodules revealed a normal liver architecture with marked lobular disarray due to multiple well-formed sarcoid-type granulomas, some displaying central "clean" necrosis. The granulomas consisted of epithelioid cells, multinucleated Langhans-type giant cells, and peripheral lymphocytes. Despite negative histochemical staining results, including Gram, Periodic Acid-Schiff (PAS), Grocott, Warthin-Starry, and Ziehl-Neelsen techniques, morphological features strongly suggested an infectious etiology (Figure 2). Nucleic acid extraction and polymerase chain reaction (PCR) analysis for Mycobacterium tuberculosis confirmed the presence of the bacterium in the biopsy sample
Liver biopsyAFB: acid-fast bacillus; PAS: Periodic Acid-SchiffLiver biopsy showing granulomatous inflammation with multiple well-formed epithelioid granulomas, some displaying central "clean" necrosis (Figure A). There was no evidence of any organism in the AFB stain (Figure B), the Warthin-Starry stain (Figure C), and the PAS stain (Figure D)
The patient was initiated on a standard anti-TB regimen (isoniazid, rifampin, pyrazinamide, and ethambutol), which led to significant clinical improvement, including the resolution of fever. He remains under close follow-up with ongoing antiretroviral and anti-TB therapy.
Discussion
Hepatic and splenic TB is rare, accounting for less than 1% of all TB cases [1,3]. It is particularly uncommon for these forms of TB to serve as the initial presentation of the disease, especially in HIV-positive patients [2,6]. Immunosuppression caused by HIV increases susceptibility to latent TB reactivation and dissemination to atypical sites like the liver and spleen [1,5]. In this case, the presence of multiple micronodules across the liver, spleen, and lungs, combined with microbiological confirmation of Mycobacterium tuberculosis, led to the assumption of disseminated TB. This case underscores the importance of considering extrapulmonary TB in the differential diagnosis of HIV-positive patients, particularly when symptoms like fever and weight loss mimic other systemic infections or malignancies.
Imaging studies in such cases often reveal hypodense or micronodular lesions, findings that can also be observed in metastatic liver disease or fungal infections. In this patient, cat scratch disease was clinically suspected, but the typical necrotizing stellate abscesses surrounded by palisading histiocytes were absent. A definitive diagnosis was achieved only through a combination of histopathological suspicion and microbiological confirmation of TB.
Similar cases in the literature underscore the diagnostic challenges posed by hepatic TB. Wyffels et al. reported cases where hepatic TB mimicked metastatic liver cancer or cholangiocarcinoma [7]. Likewise, Niyogi et al. described five cases of primary hepatic TB in which imaging studies initially suggested malignancy, with diagnoses ultimately confirmed through biopsy [8,9]. These examples reinforce the need for a high index of suspicion for TB in HIV-positive patients presenting with unexplained liver lesions.
Current guidelines recommend histopathological confirmation for extrapulmonary TB, as imaging alone is often insufficient [10]. Clinicians must remain vigilant for opportunistic infections in HIV-positive patients, which can further complicate diagnosis. Given the extent of involvement in this patient, disseminated TB was presumed, necessitating early initiation of therapy. Anti-TB treatment remains the cornerstone of management, typically involving an initial two-month regimen of isoniazid, rifampin, pyrazinamide, and ethambutol, followed by isoniazid and rifampin for an additional four months. This case underscores the critical importance of timely diagnosis and early initiation of treatment to prevent severe complications associated with disseminated TB in immunocompromised individuals.
Conclusions
Extrapulmonary TB involving the liver and spleen should be considered in HIV-positive patients presenting with unexplained systemic symptoms such as persistent fever, weight loss, and fatigue. Because hepatic and splenic lesions may closely mimic malignancies or fungal infections, a definitive diagnosis requires combined histopathological and microbiological evaluation. Pathology plays a central role, as the identification of granulomatous inflammation guides targeted microbiological investigations, including PCR, for precise etiological confirmation.
Importantly, clinical improvement following corticosteroid therapy, often interpreted as IRIS, should not be relied upon in isolation without thoroughly excluding active infection. Early recognition and prompt initiation of anti-TB therapy are crucial to improve outcomes in immunocompromised patients, limiting disease progression and reducing the risk of severe complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Primary hepatic tuberculosis: an unexpected diagnosis J Com Med Col Teachers Asso Hasan SA Hassan N Hossain D 3841272023
- 2Primary hepatic tuberculosis: a rare occurrence Ann Hepatobiliary Pancreat Surg Niyogi D Goel M Shinde RS Patkar S 8083232019 https://pubmed.ncbi.nlm.nih.gov/30863814/3086381410.14701/ahbps.2019.23.1.80PMC 6405358 · doi ↗ · pubmed ↗
- 3Multiple hepatic lesions in a case of isolated hepatic tuberculosis simulating metastases on 18F-FDG PET/CT imaging Nucl Med Rev Cent East Eur Karunanithi S Sharma P Jain TK Vijay MK Kumar R 108109172014 https://pubmed.ncbi.nlm.nih.gov/25088112/2508811210.5603/NMR.2014.0027 · doi ↗ · pubmed ↗
- 4World Health Organization: global tuberculosis reports, 1997 to 20252023 https://www.who.int/teams/global-programme-on-tuberculosis-and-lung-health/tb-reports
- 5Hepatic tuberculoma: a challenging diagnosis Int J Infect Dis Wyffels K Coubeau L Dahlqvist G 509510962020 https://pubmed.ncbi.nlm.nih.gov/32439541/3243954110.1016/j.ijid.2020.05.054 · doi ↗ · pubmed ↗
- 6Isolated tuberculosis of liver & spleen: a rare presentation Clin Case Rep Rev Zubin PS Divya S 62020
- 7Tuberculosis: 6. Extrapulmonary disease CMAJ Fanning A 159716031601999 https://pmc.ncbi.nlm.nih.gov/articles/PMC 1230370/10374005 PMC 1230370 · pubmed ↗
- 8Primary hepatic tuberculosis mimicking intrahepatic cholangiocarcinoma: report of two cases Ann Surg Treat Res Park JI 98101892015 https://pmc.ncbi.nlm.nih.gov/articles/PMC 4518037/2623670010.4174/astr.2015.89.2.98PMC 4518037 · doi ↗ · pubmed ↗