Characteristics of Patients with De Novo Metastatic Breast Cancer and Positive Human Epidermal Growth Factor Receptor 2 in a Reference Center in Mexico
Rogelio J Martinez-Samano, Mireya López-Gamboa

TL;DR
This study describes characteristics and survival outcomes of Mexican patients with HER2-positive breast cancer diagnosed at a late stage.
Contribution
The study provides descriptive insights into HER2-positive de novo metastatic breast cancer in a Mexican cohort, highlighting clinical and sociodemographic patterns.
Findings
Median overall survival was 96 months with high survival rates up to five years.
No significant survival differences were found between receptor subtypes in multivariate analysis.
Most patients belonged to HER2+ ER+ PR+ and HER2+ ER- PR- subtypes.
Abstract
Background Breast cancer is an important disease with a high burden worldwide; approximately 5% to 10% of cases are diagnosed as metastatic breast cancer. A subset of patients with human epidermal growth factor receptor 2 (HER2) positivity and stage IV disease at diagnosis are identified as having HER2-positive de novo metastatic breast cancer, which is poorly characterized. Methods A retrospective cohort study was performed at the National Cancer Institute in Mexico City using 10 years of collected data. Variables included patient status, sociodemographics, and clinical, pathological, treatment patterns, and receptor status, while overall survival (OS) and progression-free survival (PFS) were also estimated. For assessing possible differences between receptor-status groups, a Fisher's exact test was performed. Survival analyses were performed using Kaplan-Meier plots, and a log-rank…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
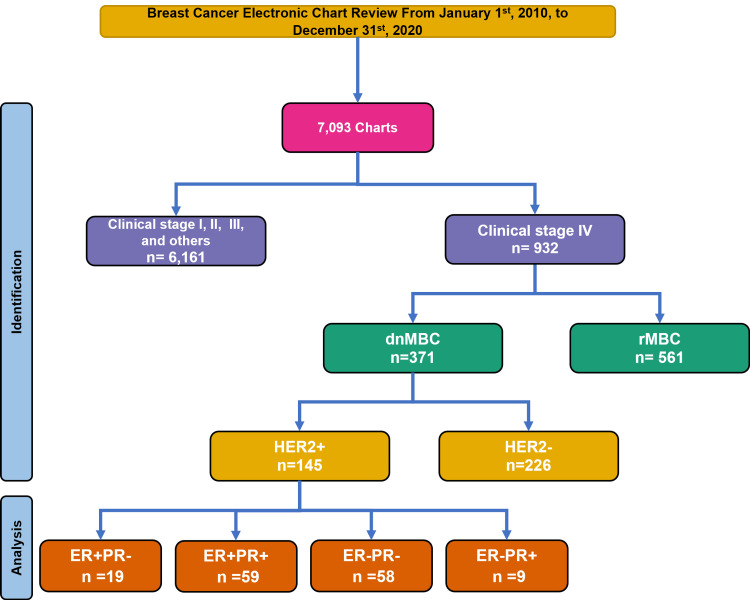 Figure 1
Figure 1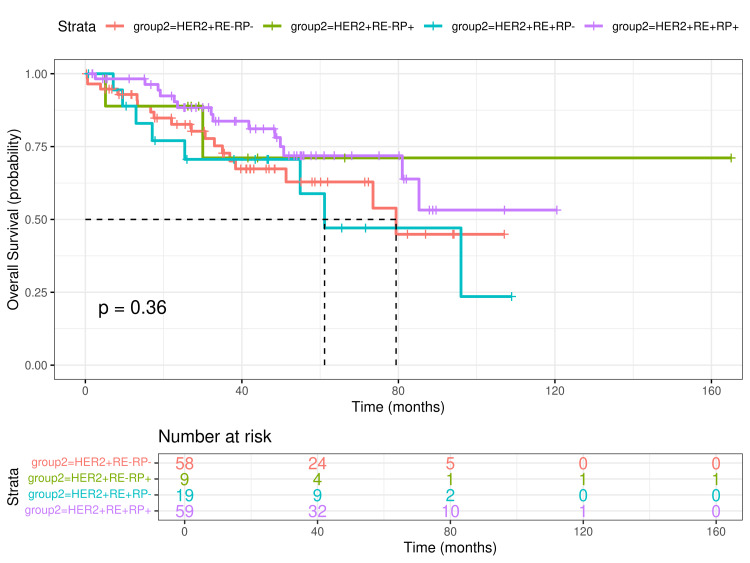 Figure 2
Figure 2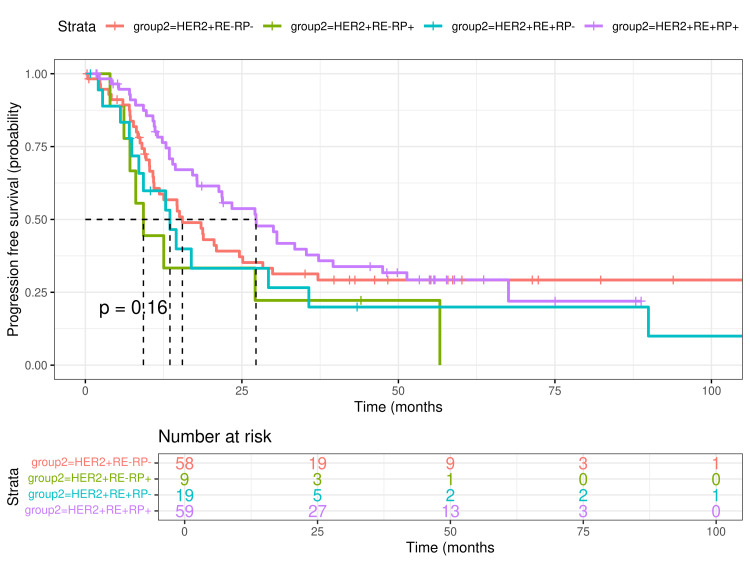 Figure 3
Figure 3| Status | All Patients (n, %) | HER2+ER+PR- (n, %) | HER2+ER+PR+ (n, %) | HER2+ER-PR- (n, %) | HER2+ER-PR+ (n, %) |
| Alive | 49 (33.8) | 6 (4.1) | 20 (13.8) | 20 (13.8) | 3 (2.1) |
| Dead | 42 (29) | 8 (5.5) | 14 (9.7) | 18 (12.4) | 2 (1.4) |
| LFU | 54 (37.2) | 5 (3.4) | 25 (17.2) | 20 (13.8) | 4 (2.8) |
| Total | 145 (100) | 19 (13.1) | 59 (40.7) | 58 (40) | 9 (6.2) |
| Characteristics | All Patients (n, %) | HER2+ER+PR- (n, %) | HER2+RE+RP+ (n, %) | HER2+RE-RP- (n, %) | HER2+RE-RP+ (n, %) |
| Marital status | |||||
| Married | 61 (42.1) | 6 (4.1) | 26 (17.9) | 27 (18.6) | 2 (1.4) |
| Divorced | 12 (8.3) | 1 (0.7) | 2 (1.4) | 6 (4.1) | 3 (2.1) |
| Single | 38 (26.2) | 7 (4.8) | 16 (11) | 13 (9) | 2 (1.4) |
| Common-law | 16 (11) | 1 (0.7) | 7 (4.8) | 6 (4.1) | 2 (1.4) |
| Widowed | 18 (12.4) | 4 (2.8) | 8 (5.5) | 6 (4.1) | 0 (0) |
| Insurance status | |||||
| Insured | 8 (5.5) | 0 (0) | 4 (2.8) | 4 (2.8) | 0 (0) |
| Not insured | 137 (94.5) | 19 (13.1) | 55 (37.2) | 54 (37.2) | 9 (6.2) |
| Geographical origin | |||||
| Center | 124 (85.5) | 15 (10.3) | 51 (35.2) | 51 (35.2) | 7 (4.8) |
| Southeast | 19 (13.1) | 4 (2.8) | 6 (4.1) | 7 (4.8) | 2 (1.4) |
| West | 2 (1.4) | 0 (0) | 2 (1.4) | 0 (0) | 0 (0) |
| Educational level | |||||
| Illiterate | 9 (6.2) | 2 (1.4) | 3 (2.1) | 4 (2.8) | 0 (0) |
| Bachelor’s | 15 (10.3) | 3 (2.1) | 8 (5.5) | 4 (2.8) | 0 (0) |
| High school | 23 (15.9) | 3 (2.1) | 8 (5.5) | 9 (6.2) | 3 (2.1) |
| Elementary | 54 (37.2) | 5 (3.4) | 21(14.5) | 24 (16.6) | 4 (2.8) |
| Secondary | 40 (27.6) | 6 (4.1) | 18 (12.4) | 15 (10.3) | 1 (0.7) |
| Technical | 4 (2.8) | 0 (0) | 1 (0.7) | 2 (1.4) | 1 (0.7) |
| Occupation | |||||
| Housewife | 112 (77.2) | 13 (9) | 45 (31) | 46 (31.7) | 8 (5.5) |
| Unemployed | 5 (3.4) | 0 (0) | 2 (1.4) | 2 (1.4) | 1 (0.7) |
| Retired | 1 (0.7) | 0 (0) | 0 (0) | 1 (0.7) | 0 (0) |
| Non-professional | 17 (11.7) | 3 (2.1) | 6 (4.1) | 8 (5.5) | 0 (0) |
| Professional | 9 (6.2) | 3 (2.1) | 5 (3.4) | 1 (0.7) | 0 (0) |
| Technical | 1 (0.7) | 0 (0) | 1 (0.7) | 0 (0) | 0 (0) |
| Characteristic | All patients (n, %) | HER2+RE+RP- (n, %) | HER2+RE+RP+ (n, %) | HER2+RE-RP- (n, %) | HER2+RE-RP+ (n, %) |
| Menopausal status | |||||
| Menopausic | 5 (3.4) | 1 (0.7) | 2 (1.4) | 2 (1.4) | 0 (0) |
| Premenopausal | 68 (46.9) | 10 (6.9) | 26 (17.9) | 27 (18.6) | 5 (3.4) |
| Postmenopausal | 72 (49.7) | 8 (5.5) | 31 (21.4) | 29 (20) | 4 (2.8) |
| Pregnancies | |||||
| >5 | 18 (12.4) | 4 (2.8) | 8 (5.5) | 4 (2.8) | 2 (1.4) |
| 0-2 | 66 (45.5) | 8 (5.5) | 26 (17.9) | 27 (18.6) | 5 (3.4) |
| 3-5 | 61 (42.1) | 7 (4.8) | 25 (17.2) | 27 (18.6) | 2 (1.4) |
| BC laterality | |||||
| Right | 77 (53.1) | 8 (5.5) | 33 (22.8) | 31 (21.4) | 5 (3.4) |
| Left | 62 (42.8) | 10 (6.9) | 24 (16.6) | 24 (16.6) | 4 (2.8) |
| Both | 6 (4.1) | 1 (0.7) | 2 (1.4) | 3 (2.1) | 0 (0) |
| T status | |||||
| T1 | 3 (2.1) | 0 (0) | 1 (0.7) | 2 (1.4) | 0 (0) |
| T2 | 23 (15.9) | 4 (2.8) | 10 (6.9) | 8 (5.5) | 1 (0.7) |
| T3 | 25 (17.2) | 2 (1.4) | 11 (7.6) | 10 (6.9) | 2 (1.4) |
| T4 | 90 (62.1) | 13 (9) | 36 (24.8) | 35 (24.1) | 6 (4.1) |
| Tx | 4 (2.8) | 0 (0) | 1 ( 0.7) | 3 (2.1) | 0 (0) |
| N status | |||||
| N0 | 3 (2.1) | 0 (0) | 1 (0.7) | 1 (0.7) | 1 (0.7) |
| N1 | 19 (13.1) | 1 (0.7) | 11 (7.6) | 5 (3.4) | 2 (1.4) |
| N2 | 29 (20) | 7 (4.8) | 12 (8.3) | 8 (5.5) | 2 (1.4) |
| N3 | 93 (64.1) | 11 (7.6) | 35 (24.1) | 43 (29.7) | 4 (2.8) |
| Nx | 1 (0.7) | 0 (0) | 0 (0) | 1 (037) | 0 (0) |
| Metastasis sites* | |||||
| 1 | 68 (46.9) | 6 (4.1) | 25 (17.2) | 35 (24.1) | 2 (1.4) |
| 2 | 39 (26.9) | 4 (2.8) | 20 (13.8) | 13 (9) | 2 (1.4) |
| 3 | 23 (15.9) | 7 (4.8) | 8 (5.5) | 4 (2.8) | 4 (2.8) |
| 4 | 8 (5.5) | 1 (0.7) | 3 (2.1) | 3 (2.1) | 1 (0.7) |
| 5 | 3 (2.1) | 0 (0) | 1 (0.7) | 2 (1.4) | 0 (0) |
| 6 | 3 (2.1) | 0 (0) | 2 (1.4) | 1 (0.7) | 0 (0) |
| 7 | 1 (0.7) | 1 (0.7) | 0 (0) | 0 (0) | 0 (0) |
| Visceral MT at diagnosis | |||||
| Yes | 75 (51.7) | 7 (4.8) | 36 (24.8) | 28 (19.3) | 4 (2.8) |
| No | 70 (48.3) | 12 (8.3) | 23 (15.9) | 30 (20.7) | 5 (3.4) |
| Characteristic | All patients (n, %) | HER2+RE+RP- (n, %) | HER2+RE+RP+ (n, %) | HER2+RE-RP- (n, %) | HER2+RE-RP+ (n, %) |
| Histological type | |||||
| Invasive ductal | 124 (85.5) | 19 (13.1) | 51 (35.2) | 46 (31.7) | 8 (5.5) |
| Invasive lobular | 15 (10.3) | 0 (0) | 5 (3.4) | 9 (6.2) | 1 (0.7) |
| Other | 6 (4.1) | 0 (0) | 3 (2.1) | 3 (2.1) | 0 (0) |
| SBR status | |||||
| 3 | 5 (3.4) | 0 (0) | 2 (1.4) | 3 (2.1) | 0 (0) |
| 4 | 5 (3.4) | 0 (0) | 1 (0.7) | 3 (2.1) | 1 (0.7) |
| 5 | 6 (4.1) | 0 (0) | 3 (2.1) | 3 (2.1) | 0 (0) |
| 6 | 26 (17.9) | 6 (4.1) | 11 (7.6) | 9 (6.2) | 0 (0) |
| 7 | 41 (28.3) | 4 (2.8) | 20 (13.8) | 16 (11) | 1 (0.7) |
| 8 | 47 (32.4) | 6 (4.1) | 18 (12.4) | 18 (12.4) | 5 (3.4) |
| 9 | 11 (7.6) | 3 (2.1) | 3 (2.1) | 3 (2.1) | 2 (1.4) |
| Not reported | 4 (2.8) | 0 (0) | 1 (0.7) | 3 (2.1) | 0 (0) |
| Desmoplasia* | |||||
| Mild | 29 (20) | 5 (3.4) | 14 (9.7) | 10 (6.9) | 0 (0) |
| Moderate | 39 (26.9) | 9 (6.2) | 13 (9) | 16 (11) | 1 (0.7) |
| Severe | 56 (38.6) | 5 (3.4) | 22 (15.2) | 22 (15.2) | 7 (4.8) |
| Not reported | 21 (14.5) | 0 (0) | 10 (6.9) | 10 (6.9) | 1 (0.7) |
| Presence of inflammatory cells | |||||
| No | 6 (4.1) | 1 (0.7) | 1 (0.7) | 4 (2.8) | 0 (0) |
| Not reported | 20 (13.8) | 0 (0) | 8 (5.5) | 11 (7.6) | 1 (0.7) |
| Yes | 119 (82.1) | 18 (12.4) | 50 (34.5) | 43 (29.7) | 8 (5.5) |
| Lymphovascular invasion | |||||
| No | 66 (45.5) | 9 (6.2) | 20 (13.8) | 32 (22.1) | 5 (3.4) |
| Not reported | 12 (8.3) | 1 (0.7) | 5 (3.4) | 5 (3.4) | 1 (0.7) |
| Yes | 67 (46.2) | 9 (6.2) | 34 (23.4) | 21 (14.5) | 3 (2.1) |
| Neural invasion | |||||
| No | 102 (70.3) | 14 (9.7) | 39 (26.9) | 42 (29) | 7 (4.8) |
| Not reported | 23 (15.9) | 2 (1.4) | 11 (7.6) | 9 (6.2) | 1 (0.7) |
| Yes | 20 (13.8) | 3 (2.1) | 9 (6.2) | 7 (4.8) | 1 (0.7) |
| KI67 | |||||
| >45 | 63 (43.4) | 10 (6.9) | 20 (13.8) | 28 (19.3) | 5 (3.4) |
| ≤15 | 18 (12.4) | 3 (2.1) | 10 (6.9) | 4 (2.8) | 1 (0.7) |
| 16-25 | 15 (10.3) | 1 (0.7) | 9 (6.2) | 5 (3.4) | 0 (0) |
| 26-35 | 27 (18.6) | 3 (2.1) | 12 (8.3) | 11 (7.6) | 1 (0.7) |
| 36-45 | 22 (15.2) | 2 (1.4) | 8 (5.5) | 10 (6.9) | 2 (1.4) |
| Receptor Type | All patients (n, %) | HER2+RE+RP- (n, %) | HER2+RE+RP+ (n, %) | HER2+RE-RP- (n, %) | HER2+RE-RP+ (n, %) |
| Estrogens* | |||||
| <50 | 18 (12.4) | 10 (6.9) | 8 (5.5) | 0 (0) | 0 (0) |
| 101–200 | 42 (29) | 8 (5.5) | 34 (23.4) | 0 (0) | 0 (0) |
| 201–300 | 12 (8.3) | 1 (0.7) | 11 (7.6) | 0 (0) | 0 (0) |
| 51–100 | 6 (4.1) | 0 (0) | 6 (4.1) | 0 (0) | 0 (0) |
| Progesterone# | |||||
| <50 | 29 (20) | 0 (0) | 22 (15.2) | 0 (0) | 7 (4.8) |
| 101-200 | 21 (14.5) | 0 (0) | 21 (14.5) | 0 (0) | 0 (0) |
| 201-300 | 6 (4.1) | 0 (0) | 6 (4.1) | 0 (0) | 0 (0) |
| 51-100 | 12 (8.3) | 0 (0) | 10 (6.9) | 0 (0) | 2 (1.4) |
| HER2 | |||||
| 2+ | 8 (5.5) | 1 (0.7) | 6 (4.1) | 1 (0.7) | 0 (0) |
| 3+ | 137 (94.5) | 18 (12.4) | 53 (36.6) | 57 (39.3) | 9 (62) |
| Characteristic | All Patients (n, %) | HER2+ER+PR- (n, %) | HER2+RE+RP+ (n, %) | HER2+RE-RP- (n, %) | HER2+RE-RP+ (n, %) |
| Surgery* | |||||
| Palliative mastectomy | 22 (15.2) | 2 (10.5) | 6 (10.2) | 13 (22.4) | 1 (11.1) |
| Radiotherapy site | |||||
| Breast | 87 (60) | 12 (63.2) | 39 (66.1) | 31 (53.4) | 5 (55.6) |
| Vertebral column | 23 (15.9) | 1 (5.3) | 11 (18.6) | 6 (10.3) | 5 (55.6) |
| Brain | 51 (35.2) | 4 (21.1) | 16 (27.1) | 26 (44.8) | 5 (55.6) |
| Other | 15 (10.3) | 4 (21.1) | 6 (10.2) | 4 (6.9) | 1 (11.1) |
| Lines of treatment | |||||
| 1L | 145 (100) | 19 (100) | 59 (100) | 58 (100) | 9 (100) |
| 2L | 127 (87.6) | 16 (84.2) | 54 (91.5) | 50 (86.2) | 7 (77.8) |
| 3L | 93 (64.1) | 12 (63.2) | 44 (74.6) | 31 (53.4) | 6 (66.7) |
| 4L | 59 (40.7) | 8 (42.1) | 27 (45.8) | 20 (34.5) | 4 (44.4) |
| 5L | 44 (30.3) | 7 (36.8) | 23 (39) | 10 (17.2) | 4 (44.4) |
| 6L | 32 (22.1) | 4 (21.1) | 19 (32.2) | 6 (10.3) | 3 (33.3) |
| 7L | 21 (14.5) | 4 (21.1) | 9 (15.3) | 5 (8.6) | 3 (33.3) |
| 8L | 11 (7.6) | 3 (15.8) | 4 (6.8) | 2 (3.4) | 2 (22.2) |
| 9L | 5 (3.4) | 2 (10.5) | 2 (3.4) | 0 (0) | 1 (11.1) |
| 10L | 1 (0.7) | 0 (0) | 1 (1.7) | 0 (0) | 0 (0) |
| Variable / Group | HR | Lower 95% CI | Upper 95% CI | p value |
| Receptor status (vs HER2+RE-RP-) | ||||
| HER2+RE+RP+ | 0.560 | 0.242 | 1.299 | 0.1768 |
| HER2+RE+RP- | 1.311 | 0.496 | 3.465 | 0.5855 |
| HER2+RE-RP+ | 0.704 | 0.156 | 3.179 | 0.6477 |
| Age (vs <50 years) | ||||
| ≥ 51years | 0.708 | 0.313 | 1.598 | 0.4056 |
| Marital status (vs widowed) | ||||
| Married | 0.510 | 0.158 | 1.654 | 0.2624 |
| Divorced | 0.635 | 0.149 | 2.708 | 0.5393 |
| Single | 0.465 | 0.127 | 1.704 | 0.2478 |
| Common-law | 0.546 | 0.124 | 2.405 | 0.4240 |
| Insurance status (vs not insured) | ||||
| Insurance | 0.000 | 0.000 | NE | 0.9945 |
| Geographical origin (vs Southeast) | ||||
| Center | 1.824 | 0.604 | 5.511 | 0.2868 |
| West | 0.000 | 0.000 | NE | 0.9957 |
| Educational level (vs technical) | ||||
| Illiterate | 2.281 | 0.199 | 26.154 | 0.5076 |
| Bachelor’s | 0.504 | 0.023 | 10.834 | 0.6615 |
| High school | 1.299 | 0.124 | 13.547 | 0.8271 |
| Elementary | 1.073 | 0.122 | 9.443 | 0.9495 |
| Secondary | 1.370 | 0.150 | 12.509 | 0.7804 |
| Occupation (vs technical) | ||||
| Housewife | 0.233 | 0.000 | NE | 0.9996 |
| Unemployed | 0.335 | 0.000 | NE | 0.9997 |
| Retired | 0.516 | 0.000 | NE | 0.9999 |
| Non professional | 0.194 | 0.000 | NE | 0.9996 |
| Professional | 0.112 | 0.000 | NE | 0.9995 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdvanced Breast Cancer Therapies · Breast Cancer Treatment Studies · HER2/EGFR in Cancer Research
Introduction
Breast cancer (BC) is one of the leading causes of mortality and morbidity worldwide; it is the most common cancer in women and the second leading cause of death among women [1], with an estimated 2.3 million cases and 685,000 deaths in 2020 [2]. BC represents approximately 24.5% of all cancers and 15.5% of cancer deaths; it ranks first in incidence and mortality in developing countries [2].
Among patients with BC, approximately 5%-10% are diagnosed with metastases at the initial physician visit. Those patients with BC who present with synchronous macroscopic sites of distant disease at diagnosis are considered to have de novo metastatic BC (dnMBC) [3]. A subset of dnMBC cases includes those that have HER2 (human epidermal growth factor receptor 2) enriched in tumor tissue; proportionally, HER2-positive BC occurs with more frequency than HER2-negative in de novo settings [3]. Also, the expression of hormonal receptor (HR) is associated with several outcomes, but its relevance in dnMBC is not fully described [4].
Survival in BC is influenced by race, geography, socioeconomic status, and insurance status, which complicates the effort to identify the determinants of survival in patients with dnMBC [5]. In HER2-positive and HR-positive dnMBC, targeted therapy is essential and constitutes the backbone of treatment. The efficacy and safety of these molecules has been extensively studied [6].
The aim of this retrospective research is to characterize the social, clinical, treatment patterns, and pathological characteristics of HER2-positive dnMBC in a cancer care reference center in Mexico, describing the possible differences according to the HR status. In addition, a survival analysis was performed as an exploratory way to infer possible associations between variables and outcomes.
Materials and methods
This was a retrospective cohort study carried out in the National Cancer Institute in Mexico City with the participation of patients with dnMBC. To obtain records from target patients, a search of electronic health records was made based on a list provided by the statistics and archive department and selectively filtered after reviewing clinical information about cancer histories and the fulfillment of criteria for HER2-positive dnMBC. The time for data collection was 10 years (from January 2010 to December 2020). Data was collected prospectively and retrospectively outside this time window to ensure the collection of all relevant variables for survival analysis. The cut-off for analysis was May 2024.
The collected variables were patient status (alive, dead, and lost to follow-up); sociodemographics (age, marriage status, medical insurance status, geographical origin, level of education, and occupation); clinical data (age of menarche, menopausal status, births, breast cancer laterality, tumor, node, metastasis (TNM) status, and metastasis number and localization); treatment patterns (surgery, radiotherapy, lines of treatment) and pathological features (cancer type; pattern; Scarff-Bloom-Richardson (SBR) status; desmoplasia; presence of inflammatory cells; lymphatic, vascular and neural permeation; estrogens (ER), progesterone (PR), HER2 receptor status; and KI67 expression reported as a percentage of expression in the tumoral tissue). The receptor quantification was according to institutional procedures (Allred score) using internal cut-off thresholds for defining positivity. For assessing possible differences between groups, Fisher’s exact tests were performed to compare receptor-status groups for categorical data.
As an exploratory analysis, survival techniques were used to describe the possible effect of receptor status, and sociodemographics in survival. Overall survival (OS) was calculated from the first time the patient received any treatment (biological or chemotherapy) for BC until death, last consultation, or lost to follow-up (LFU); progression-free survival (PFS) was calculated from first time patient received any treatment until clinical or radiological disease progression (whichever happened first) according with medical records. Survival analyses were performed using Kaplan-Meier plots and missing or incomplete data were censored in the analysis of time-to-event endpoints. A log-rank test was used to evaluate possible differences between groups. After proportionality assumptions were tested, a multivariate survival analyses for social and demographic variables were performed with OS data using Cox’s proportional hazard model, and the results were reported as hazard ratios with 95% confidence intervals (CI). The protocol was assessed by the local Research and Ethics Committee and approved with the number SR01/CI/01-2020.
All statistical procedures were performed using R software, version 24.0 (R Foundation for Statistical Computing, Vienna, Austria). In the statistical test, p<0.05 was considered statistically significant.
Results
Patients and status
Of the 7,093 records retrieved of patients with BC, only 145 met the criteria for HER2-positive dnMBC. According to histopathological and immunohistochemical results, 59 patients (40.7%) were stratified as HER2+ER+PR+, 58 (40%) as HER2+ER-PR-, 19 (13.1% ) as HER2+ER+PR-, and nine (6.2%) as HER2+ER-PR+ (Figure 1). At the time of analysis (May 2024), 49 patients (33.8%) were still alive, 42 (29%) had died, and 54 (37.2%) were lost to follow-up (Table 1). The total follow-up time was (median, range) 42 months (1-166 months) for all patients; 39 months (1.4-10 months) for the HER2+ER+PR- group, 44 months (3.3-121 months) for the HER2+ER+PR+ group, 35 months (27 days to 108 months) for the HER2+ER-PR- group, and 30 months (11.5-166 months) for the HER2+ER-PR+ group.
Flow chart for identifying patients with HER2-postive dnMBC according with hormonal receptorsdnMBC=de novo metastatic breast cancer, rMBC=recurrent metastatic breast cancer, HER2=human epidermic growth factor, receptor 2; ER=estrogen receptor; and PR=progesterone receptor.
Sociodemographics
Sociodemographic characteristics are shown in Table 2. All patients were women aged 52 years (28-89 years) (median, range), split as 52.1 years (29-72 years) in the HER2+ER+PR- group, 53.7 years (34-89 years) in the HER2+ER+PR+ group, 50.8 years (31-67 years) in the HER2+ER-PR- group and 48.1 years (28-62 years) in the HER2+ER-PR+ groups. Out of the participants, 61 (42.1%) were married, 38 (26.2%) were single, 18 (12.4%) were widowed, 16 (11%) practiced common-law marriage and 12 (8.3%) were divorced. One hundred and thirty-seven patients (94.5%) did not have any insurance, whereas eight (5.5%) patients had social-medical insurance. As regards the geographical origin, 124 patients (85.5%) came from the center of Mexico, 19 (13.1%) from the southeast and two (1.4%) from west of the country. No statistical differences were found for any variable or group.
Conversely, the level of education was identified in all patients: 54 (37.2%) had elementary education, 40 (27.6%) secondary education, 23 (15.9%) high school education, and 15 (10.3%) a bachelor’s degree; nine (6.2%) were illiterate and four (2.8%) had technical training. Most patients were housewives (112 patients, 77.2%) followed by no professional activities (17 patients, 11.7%), professional activities (nine patients, 6.2%), unemployed (five patients, 3.4%), and retired and technical (one patient each, 0.7%). No statistical differences were found for any variable or group.
Clinical data
The age at menarche (average, range) was 12.9 years (8-18 years) for all patients, with 12.7 years (8-18 years) in the HER2+ER+PR- group, 13 years (9-18 years) in the HER2+ER+PR+ group, 12.8 years (9-16 years) in the HER2+ER-PR- group, and 13.8 years (13-15 years) in the HER2+ER-PR- group. According to medical records, five patients (3.4%) were classified as menopausal, 68 (46.9%) as premenopausal and 72 (49.7%) as postmenopausal. We also documented parity: 66 patients (45.5%) had zero to two deliveries, 61 (42.1%) had three to five deliveries, and 18 (12.4%) had more than five deliveries. No statistical differences were found for any variable or group.
Regarding the clinical characteristics of BC, 77 patients (53.1%) had a tumor in the right mammary gland, 62 (42.8%) in the left gland, and six (4.1%) were diagnosed with double synchronic BC (bilateral). Tumor burden was reported with T4 status in 90 patients (62.1%), followed by T3 in 25 patients (17.2%), T2 in 23 patients (15.9%), Tx in four patients (2.8%), and T1 in three patients (2.1%). Also, N3, N2, N1, N0, and Nx were documented in 93 (64.1%), 29 (20%), 19 (13.1%), three (2.1%) patients, and one (0.7%) patient, respectively. Metastatic disease was measured as the number of metastatic sites in increasing order: 68 (46.9%), 39 (26.9%), 23 (15.9%), eight (5.5%), three (2.1%), three (2.1%) patients and one (0.7%) patient had one, two, three, four, five, six, and seven sites of secondary disease. Finally, visceral metastatic disease was found in 75 patients (51.7%). Statistical differences were found only in metastasis sites between the groups (p=0.0001; Table 3).
Pathological status
The histological type of BC was invasive ductal in 124 patients (85.5%), invasive lobular in 15 patients (10.3%), and another type of BC in six (4.1%). SRB scores were, in increasing order, three (five patients, 3.4%), four (five patients, 3.4%), five (six patients, 4.1%), six (26 patients, 17.9%), seven (41 patients, 28.3%), eight (47 patients, 32.4%), and nine (11 patients, 7.6%), with four not reported (2.8%). Severe desmoplasia was reported in 56 patients (38.6%), followed by moderate (39 patients, 26.9%), and mild (29 patients, 20%); desmoplasia was not reported in 21 patients (14.5%). Inflammatory cells in neoplastic tissue were reported in 119 patients (82.1%); whereas lymphovascular and neural invasion were reported in 67 (46.2%) and 20 (13.8%) patients, respectively. Finally, the KI67 biomarker was found to have a higher expression (>45%) in 63 patients (46.4%), followed by percentages in the range of 26-35 (27 patients, 18.6%), 36-45 (22 patients, 15.2%), ≤15 (18 patients, 12.4%) and 16-25 (15 patients, 10.3%). Statistical differences were found only in tumor desmoplasia (p=0.0001; Table 4).
Receptor status
The expression of estrogen receptor was reported as a range with a value of 201-300 (12 patients, 8.3%) followed by 101-200 in 42 patients (29%), 51-100 (six patients, 4.1%) and <50 in 18 patients (12.4%). In the same way, progesterone receptors in tumoral tissue were reported as ranges; a value of 201-300 was found in six patients (4.1%), followed by 101-200 in 21 patients (14.5%) , 51-100 in 12 patients (8.3%) and <50 in 29 patients (20%). HER2 receptor status was positive in 137 patients (94.5%) and indeterminate in eight patients (5.5%); for this group, a fluorescence in situ hybridization (FISH) analysis was carried out to confirm the overexpression of HER2 (Table 5). Statistical differences were found only in estrogen and progesterone receptors in tumors between groups (p=0.0001).
Treatment
Palliative mastectomy was performed in 22 (15.2%) patients; with regard to radiotherapy, 87 (60%) patients received radiation on the breast, followed 51 patients on the brain (35.2%) and 23 patients on the backbone (15.9%). At least one line of treatment was offered to all patients, up to 10 lines in one patient (Table 6). Statistical differences was found only in surgery (palliative mastectomy) between the analyzed groups (p=0.001).
Survival
OS was 96 months (median; 95% CI: 79 to not estimable), whereas median PFS was 18.7 months (95% CI: 14.5-27.3). The median of estimated OS was 79.4 months (95% CI: 51.3 to not estimable) for the HER2+ER-PR- group and 61.1 months (95% CI: 54.9 to not estimable) for the HER2+ER+PR+ group. The medians for the HER2+ER-PR+ and HER2+ER+PR- groups were not reached. The median of PFS was 15.5 months (95% CI: 10.9-28.3), 9.27 months (95% CI: 7.12 to not estimable), 13.51 months (95% CI: 8.54 to not estimable), and 27.2 months (95% CI: 17.85-39.6), for the HER2+ER-PR-, HER2+ER-PR+, HER2+ER+PR-, and HER2+ER+PR+ groups, respectively. The survival time rate for one through five years was 94% (95% CI: 90-98), 84% (95% CI: 78-91), 77% (95% CI: 69-85), 73% (95% CI: 66-82), and 66% (95% CI: 57-76). No statistical differences were found in the log-rank test for any group in OS or PFS (Figures 2, 3).
Overall survival (OS) in patients with HER2-positive dnMBC according to ER and PR expression The upper panel shows survival rates for the different groups. Data was analyzed with a log-rank test. The lower panel shows the number of patients at risk by time and by ER and PR expression.dnMBC=De novo metastatic breast cancer; HER2=Human epidermic growth factor, receptor 2; ER=estrogen receptor; PR=progesterone receptor
Progress-free survival (PFS) in patients with HER2-positive dnMBC according to ER and PR expressionThe upper panel shows survival rates for the different groups. Data was analyzed with a log-rank test. The lower panel shows the number of patients at risk by time and by ER and PR expression.dnMBC=De novo metastatic breast cancer; HER2=Human epidermic growth factor, receptor 2; ER=estrogen receptor; PR=progesterone receptor
A multivariate Cox regression was performed to determine the influence of social variables on the survival rates of dnMBC, but no factors associated with the outcome were found in the social characteristics when analyzed under the model specifications (Table 7).
Discussion
The present study described the social, clinical, and pathological characteristics and treatment patterns as well as exploratory survival outcomes in patients with HER2-positive dnMBC for the Mexican population in a reference center for cancer care. Breast cancer is the most frequent form of cancer in women and the leading cause of mortality; in 2020, the incidence was 39.5 and mortality was 9.9 per 100,000 women [7]. We found an overall incidence of dnMBC of 39% in HER2-positive MBC patients; these results are consistent with previous research in which the incidence was 28.8%-40.2% [8-12].
According to the data, the median follow-up time was 42 months (with a range of 27 days to 166 months) with no differences in hormonal receptor status between subgroups; this time is similar to that reported by Han-Fang [8] (42.8 months) and by Smith [13] (90 months in patients with durable response). This finding could be related to treatment patterns in HER2-positive dnMBC as reported by Smith [13]. Trastuzumab-Pertuzumab-Carboplatin-Docetaxel (TCHP)-based treatments are associated with prolonged responses, which could support our findings.
Regarding social and demographic characteristics, the results are consistent with previous research; for example, we found age ranges comparable to similar studies [13-15]. Conversely, our study reports on social variables in HER2-positive dnMBC. Married women, housewives, uninsured women, and women with elementary education were most frequently patients with BC; in a review, Coughlin [16] stated that social determinants such as poverty, lack of education, lack of social support, and social isolation are associated with late-stage BC diagnosis, reflecting inadequate access to medical care, consistent with our own findings. Finally, most of the patients came from center of Mexico, which can be explained by the fact that the National Cancer Institute is the reference center for highly specialized cancer care in the country for patients without medical insurance.
Reproductive factors such as early menarche, late menopause, late age at first pregnancy, and low parity can increase the risk of breast cancer [17]. For HER2-positive dnMBC patients, this is the first study in which menarche age and pregnancies are reported in a descriptive way; the menopausal status data were consistent with other studies with the same population in which postmenopausal women were the most frequent status reported, ranging from 69.9% to 77.3% [18,19].
The reported clinical burden of disease was above those reported by other authors. There was a high frequency of T4 status and N3 node status. Previously, the tumor burden had not been reported for this population; however, other comparative studies between dnMBC and recurrent metastatic breast cancer (rMBC) have reported the TN status. So, Almasri and colleagues [10] found that T2 status was more frequent than other T statuses; also, 74% of patients were positive for lymph node status. Conversely, File and colleagues [20] reported a proportion of 51.7% for T3/T4 status, and 16.1% of patients had positive nodes. The number of sites with metastasis and presence of visceral disease coincided with previous studies in which few sites were found in up to 60% of the patients [14,15,18,21,22]. As reported by others, this burden of disease is characteristic for metastatic breast cancer [23] and our observations corresponded with those findings.
Several pathological features have not been reported previously for HER2-positive dnMBC; the present study has documented characteristics such as inflammatory cells and the presence of desmoplasia in tumor tissue as well as lymphovascular and neural infiltration by BC cells. However, for MBC (both de novo and recurrent), some studies [9,10,18-20] have documented invasive ductal carcinoma, high-grade tumors, and elevated Ki67 tumor expression as reported in the present study. All studies discussed tumoral characteristics; these have been extensively reviewed [24,25] and match our findings.
One point of interest was to classify HER2-positive dnMBC in accordance with ER and PR expression; in this study, 53% and 46% of dnMBC cases had any level of estrogen or progesterone expression, respectively, and these values are in concordance with other reports with similar populations [13,15,18]. The findings regarding the strength of ER or PR positivity could be predictive factors for survival, progression, or treatment response, as reported by Morgan [26]; however, the existing data in HER2-positive dnMBC is limited and too heterogeneous to make inferences about its usefulness in disease behavior.
We reported a median OS of 96 months and a median PFS of 18.7 months for all patients; these findings were higher than others previously published; Yardley et al. [21] reported an OS of 41.7 months (95% CI: 36.1-47.2) and a PFS 12.1 of months (95% CI: 11.4-13.5) in the context of dnMBC. In the same way, Tripathy et al. [14] reported a PFS of 17.7 months (95% CI: 16.0-19.7); other reports in the same population [18] showed OS and PFS of 55.9, and 14.4 months, respectively. This difference in OS could be due to treatment patterns, as reported by Lambertini et al. [18]; for this study, we noted that patients were treated with several modalities, which could be the main reason for this difference. To clarify this, a subgroup analysis was done; surprisingly, for OS, the HER2+ER-PR+ was 79.4 months with HR of 0.70 (95% CI, 0.15-3.17) and, 61.1 months for HER2+ER+PR+ with a hazard ratio (HR) of 0.56 (95% CI: 0.24-1.29) without statistical significance. As an exploratory analysis, several factors and their effect on survival was inconclusive and the study does not clearly show if these factors are responsible for the survival and to what extent; so, more research is needed to clarify this finding.
Our study showed a survival rate of 94% from year one to 66% in year five; several publications have documented the survival rates of dnMBC in comparison with recurrent metastatic BC (rMBC); in one, the overall survival at year one was 84% and 28.9% in year five [20]. Another study [10] showed a 32.6% survival rate at year five; for the mentioned studies, the cohorts included HER2-positive and negative cases, which might cause the results to be underestimated. Conversely, Wong and colleagues [15] reported survival rates of 98% in years five and 10 in HER2-positive patients with no evidence of disease after treatment with anti-HER2 therapy; this finding supports the idea that receptor status (HER2, estrogen, or progesterone) is directly related to survival outcomes. The present study reports treatment patterns, but future research is needed to clarify this statement.
Despite our interest in identifying the influence of social variables on the survival for HER2-positive dnMBC patients, multivariate analysis did not show any factors associated with survival. However, this study reports variables such as marital status, geographical origin, level of education, insurance status, and occupation. So, the lack of any difference could be associated with tumor biology instead of social and economic variables, as reported by Soares et al. [27]. More research is needed to associate social variables with clinical outcomes in HER2-positive dnMBC.
Some limitations were observed; as a retrospective study, missing or incomplete data could affect the interpretation of results, which should be treated with some caution. This is only a limited study, and the full potential of the results should be considered in controlled conditions as randomized clinical trial. Closer examinations in survival results showed some anomalies, for example the high lost-to-follow up rate led us to question its suitability for real results; so, our results should be considered as exploratory only. The data was collected from a single institution specializing in cancer over 10 years, which could increase the robustness of findings, but more research should be done to clarify the social, clinical, and pathological relationships of HER2-positive dnMBC.
Conclusions
Breast cancer is a leading cause of mortality and morbidity worldwide; in any clinical stage, it represents a high burden of disease in the healthcare system because medical care is sometimes associated with higher resource utilization than other diseases. Recently, differences in survival between de novo and recurrent metastatic breast cancer have been reported, but molecular receptor expression has not been extensively characterized and correlated with survival outcomes. This study provides descriptive results of clinical, sociodemographic, treatment patterns, and pathological characteristics according with molecular receptor status. The reported survival outcomes should be interpreted as exploratory due to high lost-to-follow up rate, the main limitation of this retrospective study.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Breast cancer statistics 2024 CA Cancer J Clin Giaquinto AN Sung H Newman LA 4774957420243935204210.3322/caac.21863 · doi ↗ · pubmed ↗
- 2Global patterns of breast cancer incidence and mortality: a population-based cancer registry data analysis from 2000 to 2020 Cancer Commun (Lond) Lei S Zheng R Zhang S 118311944120213439904010.1002/cac 2.12207 PMC 8626596 · doi ↗ · pubmed ↗
- 3Epidemiology of de novo metastatic breast cancer Clin Breast Cancer Daily K Douglas E Romitti PA Thomas A 3023082120213375064210.1016/j.clbc.2021.01.017 · doi ↗ · pubmed ↗
- 4The evolving landscape of metastatic HER 2-positive, hormone receptor-positive breast cancer Cancer Treat Rev Boscolo Bielo L Trapani D NicolòE 10276112820243877216910.1016/j.ctrv.2024.102761 · doi ↗ · pubmed ↗
- 5Breast cancer epidemiology and contemporary breast cancer care: a review of the literature and clinical applications Clin Obstet Gynecol El Masri J Phadke S 4614816520223570321310.1097/GRF.0000000000000721 · doi ↗ · pubmed ↗
- 6Targeting HER 2-positive breast cancer: advances and future directions Nat Rev Drug Discov Swain SM Shastry M Hamilton E 1011262220233634467210.1038/s 41573-022-00579-0PMC 9640784 · doi ↗ · pubmed ↗
- 7SMEO: Consenso Mexicano sobre el diagnóstico y tratamiento del cáncer mamario SMEO: Consenso Mexicano sobre el diagnóstico y tratamiento del cáncermamario 2023 http://consensocancermamario.com/
- 8Clinical outcomes and metastatic behavior between de novo versus recurrent HER 2-positive metastatic breast cancer: a 17-year single-institution cohort study at Taipei Veterans General Hospital J Chin Med Assoc Cheng HF Tsai YF Huang CC 88948520223456140910.1097/JCMA.0000000000000622 PMC 12755518 · doi ↗ · pubmed ↗