Childhood Mental Health Characteristics of Adults Diagnosed With Borderline Personality Disorder: A Descriptive Study
Diana M Wang, Catherine A Ha, Joshua Z Xian, Henry H Kim, Gino A Mortillaro

TL;DR
This study describes high rates of mental health issues and healthcare use in young adults with borderline personality disorder, suggesting early intervention could improve outcomes.
Contribution
The study provides a large-scale descriptive analysis of psychiatric comorbidities and healthcare utilization in BPD patients.
Findings
Depressive and anxiety disorders were the most common comorbidities in BPD patients.
Most patients had psychotherapy or psychiatric visits before age 18.
Suicidal ideation was common, but actual suicide attempts were rare.
Abstract
Introduction: Borderline personality disorder (BPD) is a burdensome and diagnostically challenging condition. There is a need to identify its risk factors, yet prior studies are scarce and small-scale. We aimed to describe the prevalence of psychiatric comorbidities and the level of mental health resource utilization during adolescence in patients with BPD. Methods: We conducted a retrospective descriptive study of 938 participants (aged 18-26 years) with BPD at a large, multi-site, integrated health maintenance organization (HMO) system in Southern California. Data were collected from January 2010 to September 2020. Comorbidities of interest were other psychiatric conditions diagnosed before age 18. Healthcare utilization data included age of first psychiatry encounter, age at first psychiatric hospitalization, number of psychiatric hospitalizations per year, number of sessions of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
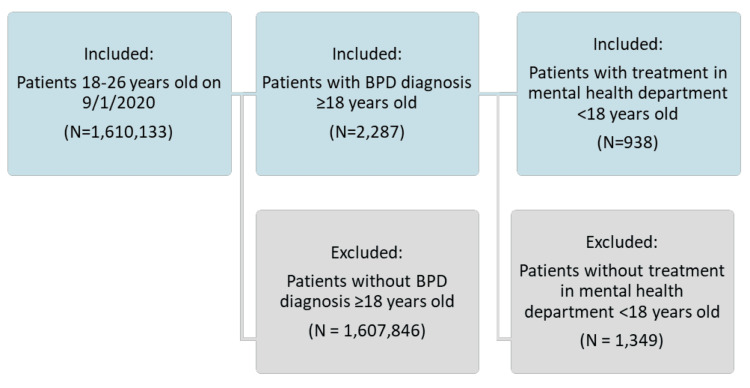 Figure 1
Figure 1| DSM-5-TR Criteria |
| A pervasive pattern of instability of interpersonal relationships, self-image, and affects, and marked impulsivity, beginning by early adulthood and present in a variety of contexts, as indicated by five (or more) of the following: |
| 1. Frantic efforts to avoid real or imagined abandonment. (Note: Do not include suicidal or self-mutilating behavior covered in Criterion 5). |
| 2. A pattern of unstable and intense interpersonal relationships characterized by alternating between extremes of idealization and devaluation. |
| 3. Identity disturbance: markedly and persistently unstable self-image or sense of self. |
| 4. Impulsivity in at least two areas that are potentially self-damaging (e.g., spending, sex, substance abuse, reckless driving, binge eating). (Note: Do not include suicidal or self-mutilating behavior covered in Criterion 5). |
| 5. Recurrent suicidal behavior, gestures, or threats, or self-mutilating behavior. |
| 6. Affective instability due to a marked reactivity of mood (e.g., intense episodic dysphoria, irritability, or anxiety usually lasting a few hours and only rarely more than a few days). |
| 7. Chronic feelings of emptiness. |
| 8. Inappropriate, intense anger or difficulty controlling anger (e.g., frequent displays of temper, constant anger, recurrent physical fights). |
| 9. Transient, stress-related paranoid ideation or severe dissociative symptoms. |
| Demographic Characteristics | Values |
| Age (years) | |
| Mean | 21.9 |
| Median | 22 |
| Range | 18.0-26.0 |
| Age Group (years), n (%) | |
| 18 | 66 (7%) |
| 19 | 105 (11.2%) |
| 20 | 116 (12.4%) |
| 21 | 120 (12.8%) |
| 22 | 139 (14.8%) |
| 23 | 124 (13.2%) |
| 24 | 110 (11.7%) |
| 25 | 93 (9.9%) |
| 26 | 65 (6.9%) |
| Sex, n (%) | |
| Female | 816 (87%) |
| Male | 122 (13%) |
| Race/Ethnicity, n (%) | |
| White | 378 (40.3%) |
| Asian | 47 (5%) |
| Black | 83 (8.8%) |
| Hispanic | 395 (42.1%) |
| Multiple | 15 (1.6%) |
| Native American or Alaskan | 2 (0.2%) |
| Pacific Islander | 3 (0.3%) |
| Other | 10 (1.1%) |
| Unknown | 5 (0.5%) |
| Diagnoses | Frequency (Percentage) |
| ADHD | |
| No | 719 (76.7%) |
| Yes | 219 (23.3%) |
| Anxiety Disorders | |
| No | 285 (30.4%) |
| Yes | 653 (69.6%) |
| Bipolar and Related Disorders | |
| No | 759 (80.9%) |
| Yes | 179 (19.1%) |
| Disruptive Behavior Disorders | |
| No | 815 (86.9%) |
| Yes | 123 (13.1%) |
| Depressive Disorders | |
| No | 155 (16.5%) |
| Yes | 783 (83.5%) |
| Neurodevelopmental Disorders | |
| No | 868 (92.5%) |
| Yes | 70 (7.5%) |
| Dissociative, Conversion, and Factitious Disorders | |
| No | 899 (95.8%) |
| Yes | 39 (4.2%) |
| Feeding and Eating Disorders | |
| No | 806 (85.9%) |
| Yes | 132 (14.1%) |
| Gender Dysphoria | |
| No | 909 (96.9%) |
| Yes | 29 (3.1%) |
| Impulse-Control Disorders | |
| No | 878 (93.6%) |
| Yes | 60 (6.4%) |
| Paraphilic Disorders | |
| No | 938 (100%) |
| Yes | 0 (0%) |
| Personality Disorders | |
| No | 885 (94.3%) |
| Yes | 53 (5.7%) |
| Schizophrenia Spectrum and Other Psychotic Disorders | |
| No | 880 (93.8%) |
| Yes | 58 (6.2%) |
| Suicide Attempts (initial encounter) | |
| No | 933 (99.5%) |
| Yes | 5 (0.5%) |
| Self-Harm and Suicide Attempts | |
| No | 754 (80.4%) |
| Yes | 184 (19.6%) |
| Suicidal Ideation | |
| No | 576 (61.4%) |
| Yes | 362 (38.6%) |
| Sleep-Wake Disorders | |
| No | 886 (94.5%) |
| Yes | 52 (5.5%) |
| Trauma- and Stress-Related Disorders | |
| No | 595 (63.4%) |
| Yes | 343 (36.6%) |
| Substance-Related and Addictive Disorders | |
| No | 716 (76.3%) |
| Yes | 222 (23.7%) |
| Tic Disorders | |
| No | 925 (98.6%) |
| Yes | 13 (1.4%) |
| Other and Unspecified Mood Disorders | |
| No | 728 (77.9%) |
| Yes | 207 (22.1%) |
| Unspecified Nonpsychotic Disorders | |
| No | 845 (90.1%) |
| Yes | 93 (9.9%) |
| Frequency* (Percentage) | Minimum | Median | Maximum | Mean | Standard Deviation | |
| Age at First Psychiatric Encounter (years) | 935** (99.7%) | 7.00 | 15.00 | 22.00 | 15.00 | 2.09 |
| Age at First Psychiatric Hospitalization (years) | 584** (62.3%) | 10.00 | 17.00 | 25.00 | 17.20 | 2.70 |
| Psychiatric Prescriber Visits Per Year Before Age 18 | 663 (70.7%) | 0.20 | 3.39 | 52.18 | 4.36 | 4.64 |
| Number of IOP/PHP Encounters Per Year Before Age 18 | 315 (33.6%) | 0.17 | 3.91 | 162.33 | 8.51 | 13.56 |
| Number of Crisis Encounters Per Year Before Age 18 | 61 (6.5%) | 0.24 | 0.84 | 17.39 | 1.84 | 2.77 |
| Number of Psychotherapy Visits Per Year Before Age 18 | 813 (86.7%) | 0.12 | 2.61 | 182.63 | 5.24 | 10.23 |
| Number of Psychiatric Hospitalizations Per Year Before Age 18 | 326 (34.8%) | 0.13 | 1.17 | 73.05 | 2.07 | 4.82 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPersonality Disorders and Psychopathology · Down syndrome and intellectual disability research · Schizophrenia research and treatment
Introduction
Borderline personality disorder (BPD) is a serious psychiatric condition defined as a “pervasive pattern of instability of interpersonal relationships, self-image, and affects, and marked impulsivity, beginning by early adulthood and present in a variety of contexts” [1]. However, due to the wide range and severity of BPD symptoms, vague descriptors, and variability in disease course, debate continues over the appropriate age for diagnosis, the criteria for diagnosis, and the necessity of BPD as a diagnosis altogether [2,3]. Compared to other psychiatric illnesses, BPD has been associated with higher rates of suicide, severe psychological impairment, and utilization of mental health resources [4,5]. While BPD affects up to 3% of the general population, patients with BPD encompass 10% of outpatient mental health visits and 20% of psychiatric inpatient hospitalizations [1,6]. The high mortality, morbidity, and burden of BPD call for the need to identify risk factors for its development, but few studies have examined traits in childhood that may predict BPD diagnosis.
While diagnosing BPD before age 18 has been historically controversial, there has been evidence of similar reliability and stability of BPD in adolescence and adulthood, thus supporting earlier diagnosis [7,8]. Previous research has identified impulsivity, emotional sensitivity, over-reactivity, invalidating parenting, disorganized attachment, and childhood trauma as potential pediatric predictors of BPD [9]. Prior studies have also suggested that adolescents with BPD have comorbid mental health conditions, most notably mood disorders, eating disorders, dissociative and post-traumatic stress disorders, substance use disorders, and oppositional defiant disorder [10,11]. However, these studies have been on relatively smaller scales, and the number of factors investigated has been limited. Our study aims to describe the prevalence of psychiatric comorbidities and the level of mental health resource utilization in adolescent patients with BPD within a large health maintenance organization (HMO) health system.
Materials and methods
This was a retrospective descriptive chart review study at a large, multi-site, integrated HMO health system, Kaiser Permanente Fontana Medical Center, Fontana, in Southern California, United States that serves a population of both privately and publicly insured patients from data collected between January 2010 and September 2020. The study was approved by the Institutional Review Board of Kaiser Permanente Southern California/Hawaii (approval number: 12709).
Study population
Out of 1,610,133 patients aged 18 to 26 years, those without a BPD diagnosis and those without treatment in the mental health department prior to age 18 were excluded, resulting in a final study population of 938 patients (Figure 1).
Study cohort selection flowchart.
Data collection
Age, race, sex, psychiatric diagnoses, and healthcare utilization data were retrospectively retrieved from patient medical records. Psychiatric illnesses were identified via International Classification of Diseases (ICD)-9 and ICD-10 codes and grouped into broader categories based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (Table 1) [1].
Healthcare utilization data included age at first encounter with psychiatry, age at first psychiatric hospitalization, number of psychiatric hospitalizations per year, number of sessions of intensive outpatient group therapy and partial hospitalization, number of visits with a psychiatrist, number of crisis calls, and number of psychotherapy sessions. Data were reported as the number of relevant encounters per year to control for the fact that these patients may not have had services through our specific healthcare organization for their entire life, and the electronic health record was only fully established throughout this hospital system in 2010.
Results
Demographics
Of the 938 participants included in the study population, 816 (87.0%) were female, with a mean age of 22 years (Table 2). A total of 395 (42.1%) participants were of Hispanic ethnicity, 378 (40.3%) were of White race, 83 (8.8%) were of Black race, 47 (5.0%) were Asian, three (0.3%) were Pacific Islander, two (0.2%) were Native American or Alaskan, 15 (1.6%) were multiracial, 10 (1.1%) were other, and five (0.5%) were of unknown race. Compared to the overall patient population, the study population had a higher proportion of female and White participants, a lower proportion of Asian participants, and a lower mean age. The prevalence of BPD in the overall population was 0.1% (2,287 out of 1,610,133).
Comorbidities
In examining comorbid conditions diagnosed before age 18, 219 (23.3%) were diagnosed with attention-deficit/hyperactivity disorder (ADHD), 653 (69.6%) with anxiety disorders, 179 (19.1%) with bipolar disorders, 123 (13.1%) with disruptive behavior disorders, 783 (83.5%) with depressive disorders, 70 (7.5%) with neurodevelopmental disorders, 39 (4.2%) with dissociative, conversion, and factitious disorders, 132 (14.1%) with feeding and eating disorders, 29 (3.1%) with gender dysphoria, 60 (6.4%) with impulse-control disorders, zero (0%) with paraphilic disorders, 53 (5.7%) with personality disorders, 58 (6.2%) with schizophrenia spectrum and other psychotic disorders, five (0.5%) with suicide attempt, 184 (19.6%) with self-harm behavior, 362 (38.6%) with suicidal ideation, 52 (5.5%) with sleep-wake disorders, 343 (36.6%) with trauma- and stress-related disorders, 222 (23.7%) with substance-related and addictive disorders, 13 (1.4%) with tic disorders, 207 (22.1%) with other or unspecified mood disorders, and 93 (9.9%) with unspecified nonpsychotic disorders (Table 3).
Table 3: Concurrent diagnoses during adolescence (age < 18 years old) in patients with BPD (N=938)BPD: borderline personality disorder; ADHD: attention deficit hyperactivity disorder
Healthcare utilization
Of the 938 participants, 935 (99.7%) had at least one psychiatric encounter in adolescence or adulthood, with a mean age at the first encounter with psychiatry of 15 years (Table 4). A total of 584 (62.3%) had at least one psychiatric hospitalization in adolescence or adulthood, with a mean age at first inpatient psychiatric hospitalization of 17 years. The mean time between participants’ first psychiatric encounter and first inpatient psychiatric hospitalization was two years. Before age 18, 663 (70.7%) participants had a psychiatric visit with a mean of 4.36 psychiatry visits per year, 813 (86.7%) had psychotherapy visits with a mean of 5.24 per year, and 326 (34.8%) had a psychiatric hospitalization with a mean of 2.07 per year. Prior to adulthood, 315 (33.6%) were part of an intensive outpatient therapy program (IOP) or partial hospitalization program (PHP) visit with a mean of 8.51 per year, and 61 (6.5%) had psychiatric crisis encounters with a mean of 1.84 per year.
**Table 4: Mental health service utilization data in study population (based only on those who utilized each service) (N=938)*Number of patients who utilized this healthcare service Includes patients who utilized this healthcare service in adolescence and/or adulthoodIOP: intensive outpatient program; PHP: partial hospitalization program
Discussion
Our descriptive study looked at early adolescent comorbidities and psychiatric service utilization among patients with BPD in a large HMO health system.
Comorbidities
The comorbidities with the highest prevalences in our study population before age 18 were depressive and anxiety disorders at 83.5% (n=783) and 69.6% (n=653), respectively, which is consistent with prior literature on both adolescents and adults [10,12]. Other previously indicated comorbid adolescent diagnoses, including trauma- and stress-related disorders, substance-related and addictive disorders, attention-deficit/hyperactivity disorder (ADHD), and feeding and eating disorders, were also notable in our study, with prevalences of 36.6% (n=343), 23.7% (n=222), 23.3% (n=219), and 14.1% (n=132), respectively [10,13]. Our data reaffirm these comorbidities as potential early predictors of BPD to be explored in future comparative analyses.
Additionally, about 60% of patients with BPD have been shown to exhibit suicidality or self-injurious behavior, and BPD symptom severity has been associated with suicidal ideation and attempts in adolescents [1,14]. One prior study found BPD to be associated with increased suicidal ideation and self-injury in children as early as preschool [9]. Our data show suicidal ideation and self-harm in 38.6% (n=362) and 19.6% (n=184) of the study population before age 18, respectively, both of which are at relatively high prevalences among psychiatric comorbidities. Interestingly, however, only 0.5% (n=5) of participants had attempted suicide in adolescence, a much lower number than other measures of suicidality. The literature is limited in specific analyses of adolescent suicide attempts in patients with BPD, but our data suggest that early intervention may help prevent progression of suicidal ideation and self-harm to active suicide attempt. Age-adapted psychotherapy approaches, such as dialectical behavioral therapy and mentalization-based therapy, have been shown to improve borderline symptoms, suicidal behaviors, and self-injury associated with BPD in adolescence [15,16]. Of note, the overall suicide rate in our study population in adolescence or adulthood was 3.3% (n=31), which is much lower than that reported in other clinical populations at 8-10% [17]. This difference may reflect differences in documentation, cohort characteristics, or patterns of healthcare access in our cohort; however, other measures of suicidality, such as suicidal ideation and self-injury, are prevalent. Thus, early intervention may still be key to potentially decreasing BPD-associated mortality.
Healthcare utilization
Patients with BPD have demonstrated high health care and emergency room utilization, especially in the setting of crises, self-injury, and suicidality [18,19]. The psychiatric healthcare utilization in our study population reflected this; the majority of patients with BPD had received psychiatric services before age 18. Stratifying for specific visit types, 70.7% (n=663) of patients had psychiatric visits, 86.7% (n=813) had psychotherapy visits, 34.8% (n=326) had psychiatric hospitalizations, and 33.6% (n=315) had an IOP or PHP encounter before adulthood. These data suggest that high healthcare utilization is seen even at earlier ages in patients with BPD.
Limitations and future directions
While these findings support the need for further research in pediatric personality disorders, there are a few limitations. Our study was descriptive and did not use statistical methods to analyze associations between BPD and potential predictors. Instead, we reported prevalences of comorbidities and healthcare utilization that are notable within our study population and should be further investigated in future research.
Additionally, due to changes between ICD-9 and ICD-10, certain diagnostic codes from the prior version needed to be equated to those in the current one. For example, non-suicidal self-harm behaviors and suicide attempts were combined under the same ICD-9 code but later separated in ICD-10 coding. Thus, our study may not fully capture specific distinctions between different code categorizations.
Furthermore, the generalizability of our findings remains limited to HMO-health-system clinical settings in the United States. The prevalence of BPD diagnoses in our study population was 0.1%, which is relatively low compared to the 3% previously noted in the general population [6]. This may also reflect underdiagnosis, given the challenges of diagnosing BPD that include wide variability of disease symptoms and course, potential overlap of traits with other psychiatric illnesses, and hesitancy to diagnose a condition tied to a stigma of therapeutic difficulty [2,20].
Future studies should perform comparative analyses focused on pediatric populations to see if notable adolescent comorbidities identified in our study, such as depression and anxiety, are associated with a greater risk of developing BPD, and if early screening for these factors can improve BPD-associated outcomes. Further research should also specifically consider socio-cultural factors to elucidate whether potential disparities between different demographic groups in adolescence are reflective of those observed in adulthood. For instance, African American women with BPD were shown to experience more severe symptoms of distress tolerance than White counterparts, and BPD was found to be more prevalent among Native American men, younger adults, and those with lower socioeconomic status [21,22]. Understanding these patterns in adolescents is essential to provide equitable care. In addition, more studies on potential early interventions in adolescents are warranted to identify effective ways to reduce the incidence of BPD, BPD-associated suicidality, and the severity of borderline traits.
Conclusions
BPD continues to pose multifaceted challenges in the identification, treatment, and management of symptoms in both the adult and child and adolescent patient populations. Early diagnosis and treatment of BPD may be essential to improving outcomes later in life. This study further elucidated the high comorbidity of mood disorders and high healthcare utilization by this patient population, though further research is needed to validate the statistical significance of these potential predictors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Diagnostic and statistical manual of mental disorders: DSM-5™ (5th ed.)Arlington, VA American Psychiatric Publishing, Inc.2013
- 2Diagnosis and treatment of borderline personality disorder in young people Curr Psychiatry Rep Chanen AM Nicol K Betts JK Thompson KN 252220203233577110.1007/s 11920-020-01144-5 · doi ↗ · pubmed ↗
- 3Response: Personality disorder is here to stay across the lifespan - a response to commentaries on the May 2022 debate Child Adolesc Ment Health Tyrer P 2532552720223584292110.1111/camh.12583 · doi ↗ · pubmed ↗
- 4Treatment utilization by patients with personality disorders Am J Psychiatry Bender DS Dolan RT Skodol AE 29530215820011115681410.1176/appi.ajp.158.2.295 · doi ↗ · pubmed ↗
- 5Borderline personality disorder Lancet Lieb K Zanarini MC Schmahl C Linehan MM Bohus M 45346136420041528874510.1016/S 0140-6736(04)16770-6 · doi ↗ · pubmed ↗
- 6Personality disorders: community prevalence and socio-demographic correlates Curr Opin Psychol Eaton NR Greene AL 28322120182896146210.1016/j.copsyc.2017.09.001 · doi ↗ · pubmed ↗
- 7Borderline personality disorder in young people and the prospects for prevention and early intervention Curr Psychiatry Rev Chanen A Jovev M Mc Cutcheon L Jackson H Mc Gorry P 485742008
- 8Two-year stability of personality disorder in older adolescent outpatients J Pers Disord Chanen AM Jackson HJ Mc Gorry PD Allot KA Clarkson V Yuen HP 5265411820041561566510.1521/pedi.18.6.526.54798 · doi ↗ · pubmed ↗