Diffuse Pericardial and Diaphragmatic Involvement of Alveolar Echinococcosis in a Liver-Transplanted Patient
Yener Aydin, Elif Gozgec, Ugur Kaya

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
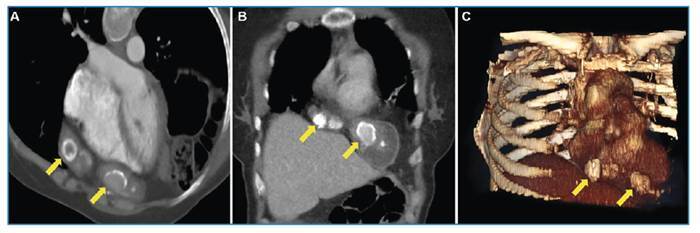 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasitic infections in humans and animals · Parasitic Infections and Diagnostics · Amoebic Infections and Treatments
A 40-year-old woman presented to our hospital with chest pain. She had undergone liver transplantation 5 years ago for alveolar echinococcosis. Radiological imaging revealed a hyperdense lesion in the pericardial area, characterized by dense calcified areas extending to the diaphragm (Figure 1). The patient underwent median laparotomy, and the lesion was resected en bloc with portions of the diaphragm and pericardium. The pericardial defect was reconstructed using the bovine pericardium, and the diaphragmatic defect was repaired using a Prolene mesh (Ethicon; Somerville, NJ, USA). Alveolar echinococcosis was confirmed histopathologically by identifying laminated membranes using periodic acid-Schiff (PAS) staining. The postoperative course was uneventful, and the patient was discharged on postoperative day 7.
FIGURE 1:Contrast-enhanced thorax CT images obtained in the axial oblique (A) and coronal (B) planes, as well as 3D oblique anterior-posterior reconstruction images (C), showing a central hyperdense lesion (arrows) in the pericardial area extending to the diaphragm.
Alveolar echinococcosis is a life-threatening parasitic disease caused by Echinococcus multilocularis, which primarily affects the liver. Early stage management relies on radical surgical resection combined with adjuvant chemotherapy to achieve the best outcomes; however, liver transplantation remains the only curative treatment for advanced alveolar echinococcosis1 ^,^ 2. Albendazole, the most widely used benzimidazole agent, is administered to prevent recurrence in surgically managed cases and to suppress parasitic growth in patients in whom surgery is not feasible1. In rare cases, recurrence of alveolar echinococcosis with calcified lesions can occur after transplantation, potentially involving extrahepatic sites3. Surgical resection should be considered as an effective approach for managing pleural and pericardial recurrences of alveolar echinococcosis after liver transplantation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Aydin Y Ogul H Topdagi O Ulas AB Sade R Ozturk G Relevance of Pulmonary Alveolar Echinococcosis Arch Bronconeumol Engl Ed 202056127797833142018210.1016/j.arbres.2019.07.014 · doi ↗ · pubmed ↗
- 2Zhu M Gao X Wang X Meng L Multimodal imaging for the diagnosis of cardiac alveolar echinococcosis: a case report BMC Cardiovasc Disord 20252511071073996239610.1186/s 12872-025-04531-z PMC 11834188 · doi ↗ · pubmed ↗
- 3Aydin Y Ulas AB Aksungur N Eroglu A Surgical Approach in the Pulmonary Alveolar Echinococcus Arch Bronconeumol 20246063853873846111110.1016/j.arbres.2024.02.014 · doi ↗ · pubmed ↗