Postpartum Myelitis Following Dengue-Related Limbic Encephalitis
Leonardo Torioni, Isidro Quispe Gonzales, Michel Elyas Jung Haziot, Arthur Moura Sarmento, Rene Leandro Magalhães Rivero, José Ernesto Vidal

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
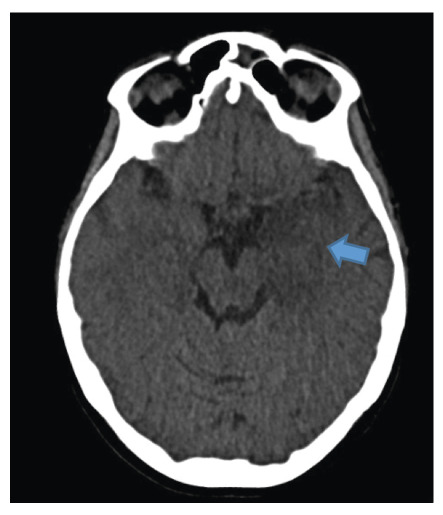 Figure 1
Figure 1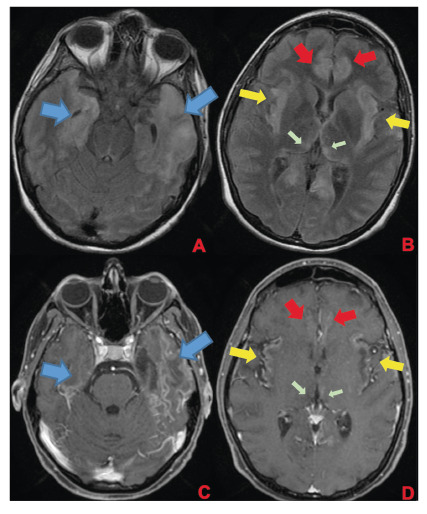 Figure 2
Figure 2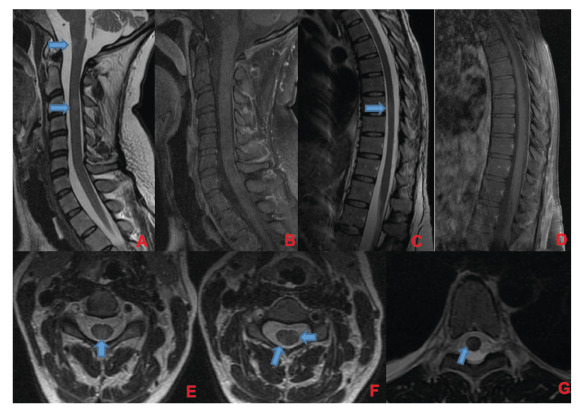 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Encephalopathies and Encephalitis · Mosquito-borne diseases and control · Viral Infections and Immunology Research
A 35-week pregnant woman was diagnosed with dengue fever. Within three days, she developed confusion and seizures, requiring an emergency caesarean section and mechanical ventilation. Brain computed tomography revealed a hypodense lesion in the left temporal lobe with mass effect, compatible with limbic encephalitis(Figure 1). Cerebrospinal fluid (CSF) analysis showed 40 cells/mm³ and 80 mg/dL of protein. Empirical intravenous acyclovir (10 mg/kg every 8 h) was initiated because of the presumptive diagnosis of herpetic encephalitis. After 9 d, she was extubated but remained cognitively impaired and was discharged 11 d later with partial neurological recovery. Two days later, she was admitted to a tertiary referral hospital with fever and generalized weakness. Brain magnetic resonance imaging (MRI) demonstrated the involvement of limbic structures, hyperintensities in the cortical and subcortical brain parenchyma with subtle mass effects, cortical enhancement in these regions, and findings consistent with volume loss in the left mesial temporal lobe and insular cortex, likely resulting from previous encephalitis (Figure 2). MRI revealed demyelinating lesions in the cervical and thoracic spinal cord (Figure 3). CSF analysis showed 57 cells/mm³, more than 300 mg/dL of protein, and glucose of 42 mg/dL. Molecular tests, including those for dengue and herpesviruses, as well as metagenomic sequencing of CSF, were negative. A comprehensive panel for autoimmune encephalitis in both the blood and CSF also yielded negative results. She received pulse methylprednisolone for 5 d, followed by intravenous immunoglobulin for 5 d, with slight cognitive improvement.
FIGURE 1:Initial CT scan of the patient. Hypodense lesion in left mesial temporal lobe with mass effect (blue arrow). Limbic encephalitis was suspected.
FIGURE 2:First brain MRI of the patient. In the superior row (A and B), axial FLAIR images; in the inferior row (C and D), axial T1 post-contrast images. Findings demonstrate encephalitis with involvement of limbic structures such as the temporal lobes (blue arrows), insula (yellow arrows), cingulate gyrus (red arrows), and medial portions of the thalami (green arrows). FLAIR images (A and B) show hyperintensities in cortical and subcortical brain parenchyma with a subtle mass effect, while post-gadolinium images demonstrate cortical enhancement in these regions and findings consistent with volume loss in the left mesial temporal lobe and insular cortex, likely resulting from previous encephalitis.
FIGURE 3:Corresponding spinal cord images of MRI shown in Figure 2. Demyelinating lesions in cervical (A, B, E, and F) and thoracic spinal cord (C, D, and G). In A and B, sagittal plane of cervical spinal cord, showing lesions in T2-weighted image (A) without enhancement in T1 post-gadolinium (B). There are involvement of spinal cord grey matter (E) and white matter (F) as shown in axial T2-weighted images. In C and D, sagittal plane of thoracic spinal cord, showing one lesion in T2-weighted image (C) without enhancement in T1 post-gadolinium (D). This lesion was located in spinal cord white matter as shown in axial T2-weighted image in that level (G). Demyelinating lesions are indicated by blue arrows.
Neurological manifestations occur in 1-5% of patients with dengue1. Both direct and indirect viral mechanisms contribute to dengue-associated neurological disease2 ^,^ 3. The clinical and radiological findings in our case suggest the presence of two successive neurological complications: limbic encephalitis and myelitis. The primary mechanisms include direct viral invasion and autoimmunity, respectively. This case highlights the importance of early recognition of these complications, especially during outbreaks, and the potential use of corticosteroids and immunotherapy in selected patients.
ETHICAL STATEMENT
This study was approved by the research and ethics committees of the corresponding institutions. The study began on March/24, and the patient signed an informed consent form indicating her agreement to participate.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Puccioni-Sohler M Rosadas C Cabral-Castro MJ Neurological complications in dengue infection: a review for clinical practice Arq Neuropsiquiatr 2013716676712414150110.1590/0004-282X 20130147 · doi ↗ · pubmed ↗
- 2Carod-Artal FJ Wichmann O Farrar J Gascón J Neurological complications of dengue virus infection Lancet Neurol 2013129069192394817710.1016/S 1474-4422(13)70150-9 · doi ↗ · pubmed ↗
- 3Burrell CJ Howard CR Murphy FA Pathogenesis of Virus Infections Fenner and White's Medical Virology 201777104