Data-driven predictive modeling for massive intraoperative blood loss during living donor liver transplantation: Integrating machine learning techniques
Taiichi Wakiya, Yukihiro Sanada, Noriki Okada, Yuta Hirata, Toshio Horiuchi, Takahiko Omameuda, Yasuharu Onishi, Yasunaru Sakuma, Hironori Yamaguchi, Yoshihiro Sasaki, Naohiro Sata

TL;DR
This study uses machine learning to predict severe bleeding during liver transplants, improving risk assessment for better patient outcomes.
Contribution
A data-driven machine learning model is developed to predict massive intraoperative blood loss in living donor liver transplants.
Findings
A machine learning model achieved an AUC of 0.844 in predicting massive intraoperative bleeding.
An online risk calculator was developed and made publicly available for clinical use.
The model outperformed traditional logistic regression in capturing complex risk interactions.
Abstract
Massive intraoperative bleeding (IBL) in liver transplantation (LT) poses serious risks and strains healthcare resources necessitating better predictive models for risk stratification. As traditional models often fail to capture the complex, non-linear patterns underlying bleeding risk, this study aimed to develop data-driven machine learning models for predicting massive IBL during living donor LT (LDLT) using preoperative factors. Two hundred ninety consecutive LDLT cases from a prospective database were analyzed. Logistic regression models were built using 73 preoperative demographic and laboratory variables to predict massive IBL (≥ 80 mL/kg). The dataset was randomly split (70% training, 30% testing). The model was trained and validated through three-fold cross-validation, with backward stepwise feature selection iterated 100 times across unique random splits. The final model,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
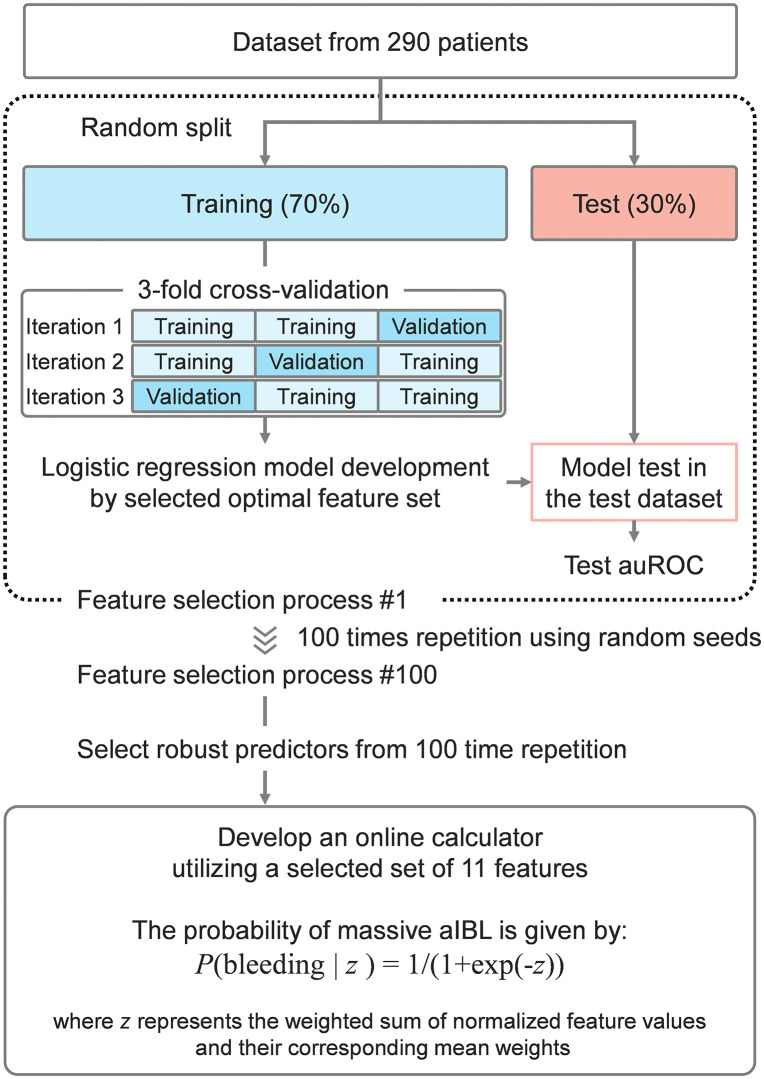 Fig 1
Fig 1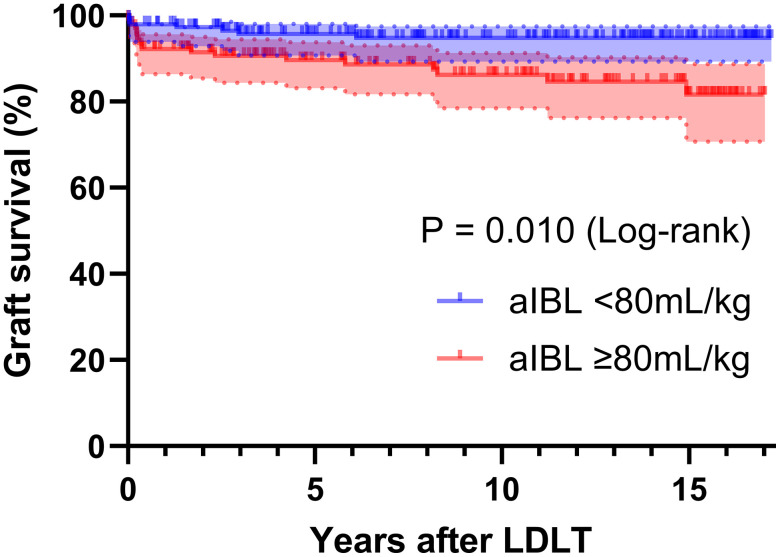 Fig 2
Fig 2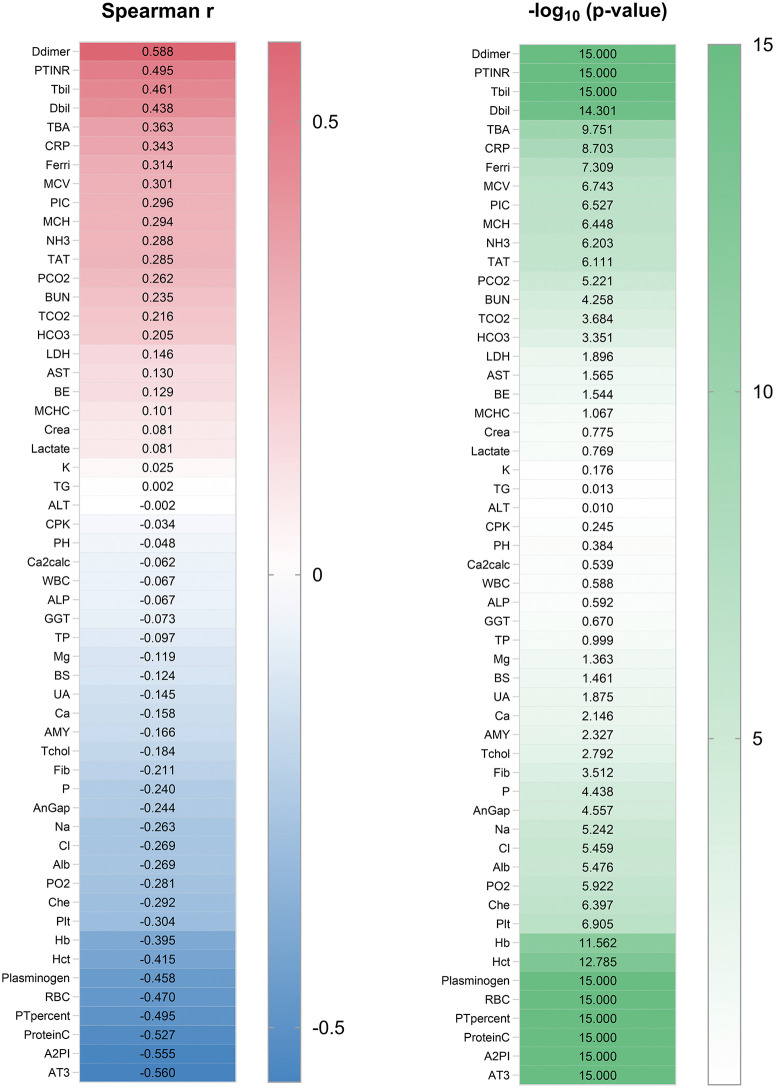 Fig 3
Fig 3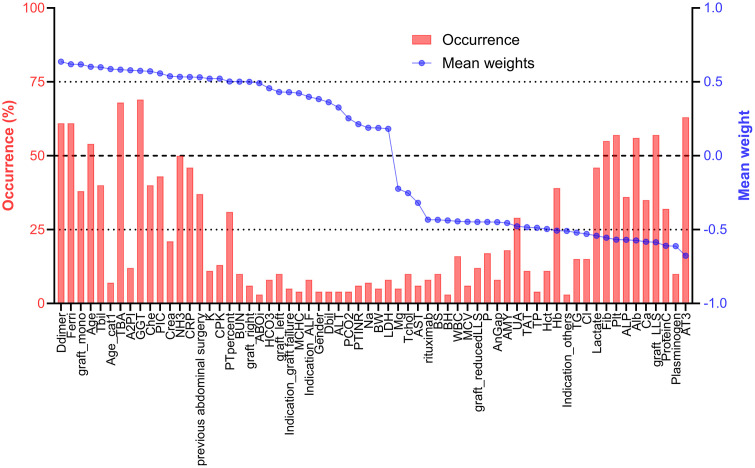 Fig 4
Fig 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrgan Transplantation Techniques and Outcomes · Liver Disease and Transplantation · Blood donation and transfusion practices
Introduction
Liver transplantation (LT) is a high-risk procedure frequently accompanied by substantial intraoperative bleeding (IBL), which can lead to adverse outcomes [1–3]. Additionally, perioperative bleeding and transfusions consume significant human and financial resources [4,5]. Accordingly, effective strategies to anticipate and reduce bleeding are essential for optimizing outcomes and maintaining the sustainability of transplant programs.
Despite ongoing advances, predicting critical IBL during LT remains a major clinical challenge. Risk stratification tools using conventional statistical methods, such as logistic regression, have been developed to identify patients at increased risk [6–9]. However, these models often assume linearity and independence among variables, limiting their ability to capture the complex, multifactorial nature of LT-associated bleeding. As a result, their accuracy and clinical utility remain suboptimal.
Machine learning offers a promising alternative by allowing the integration of numerous interrelated factors without requiring pre-specified assumptions about variable relationships. ML models can capture nonlinear associations and detect complex patterns that traditional approaches or clinical intuition may overlook. This capability also extends to handling high-dimensional datasets and identifying subtle but clinically relevant trends, potentially offering novel insights into perioperative risk [10,11]. This capability may enhance the predictive performance of bleeding models and facilitate more personalized perioperative management.
Although ML has shown value in various surgical contexts [12–14], its application in predicting bleeding outcomes in LT is still limited. Therefore, we aimed to develop a data-driven, ML-based model using prospectively collected preoperative variables to predict massive IBL in LDLT. Our objective was to establish a clinically applicable framework that outperforms conventional models and supports individualized surgical planning.
Materials and methods
Patients
We conducted a retrospective monocentric observational study using a prospectively maintained database. This study was approved by the Ethics Committee of Jichi Medical University (Approval No. 20−008). This study was designed and conducted in accordance with the principles of the Declaration of Helsinki and Istanbul. The need for written informed consent for the present study was waived by the Institutional Review Board of Jichi Medical University in view of its retrospective design, in accordance with national and local guidelines, considering the fact that all clinical/laboratory measurements and procedures were part of routine care. This study included 290 consecutive patients who underwent LDLT at our facility between 2008 and 2024.
As an institutional policy, LDLT was not undertaken in the presence of any extrahepatic infection or when vasopressor or inotropic support was required. All recipients therefore proceeded to incision without active extrahepatic infection and without vasopressor or inotropic support.
Surgical procedures and operative management
Donor hepatectomy was selected based on the recipient’s standard liver volume, weight, and graft volume determined using preoperative computed tomographic volumetry. For the recipient’s operation, inverted T-shaped or transverse incisions were made, and a total hepatectomy was performed. The graft hepatic vein was anastomosed to the stump of the recipient’s hepatic veins, which formed a single orifice, in an end-to-end manner. Hepatic artery reconstruction was routinely performed using microsurgical techniques. Choledocho-choledochostomy was the first choice for biliary reconstruction, except in cases in which the bile duct could not be used, such as with biliary atresia (BA) or primary sclerosing cholangitis.
Definition of massive intraoperative bleeding
At the start of surgery, pre-existing ascites was aspirated and excluded from IBL calculation. During the procedure, newly accumulated peritoneal fluid was included in the field in–out balance to calculate IBL. The volume was measured using suction canisters and swab weight, and it may include non-blood components to a variable extent, such as ascites, bile, or lymph. IBL was divided by body weight and referred to as adjusted intraoperative bleeding (aIBL, mL/kg). Massive aIBL was defined as aIBL ≥ 80 mL/kg. In clinical practice, the estimated circulating blood volume is approximately 70–80 mL/kg [15]. Therefore, aIBL exceeding 80 mL/kg is effectively equivalent to the loss of the entire circulating blood volume, indicating a clinically significant hemorrhagic event. Accordingly, 80 mL/kg serves as a physiologically meaningful and practical cutoff.
Data collection
For each patient, we collected demographic and laboratory data immediately before LT. The data were accessed for research purposes on April 22, 2025. Investigators had access to identifiable participant information during data collection; however, all data were de-identified prior to analysis. Seventy-three perioperative variables were extracted from the prospectively collected database. Patient demographic data included age, sex, body height, body weight, and etiology. Etiology was categorized as follows: acute liver failure (ALF), BA, graft failure, or other. Additionally, information regarding the history of previous abdominal surgery, ABO incompatibility, rituximab desensitization, and graft type was collected. Graft type was categorized as left lateral segment (LLS), left liver (LL), right liver (RL), right posterior segment (RPS), reduced LLS, or monosegment graft. To prevent statistical bias and enhance the generalizability of the model, incidence factors with a prevalence of less than 5%, such as spontaneous bacterial/fungal peritonitis and portal vein thrombosis, were excluded from the predictive variables. The 55 laboratory variables and their abbreviations are detailed in S1 Table. Prior to binary logistic regression analysis, the variables were standardized to have a mean of 0 and a standard deviation of 1, thereby ensuring that the logistic coefficients reflected the magnitude of influence on prediction. Given our focus on identifying modifiable risk factors, we placed particular emphasis on preoperative laboratory parameters, which can be influenced by conditions such as infection and thrombosis and can be actively managed before surgery. Accordingly, our candidate predictors were drawn primarily from preoperative indicators. In particular, we included pre-incision laboratory values because they integrate the cumulative effects of prior treatments, including the management of preoperative infections and the administration of blood products, and best capture the immediate preoperative physiological state. The study dataset used in this analysis is provided in S2 File.
Statistical analyses
Continuous variables were expressed as medians (ranges) and analyzed using nonparametric methods for non-normally distributed data (Mann–Whitney U test). Categorical variables were reported as numbers (percentages) and analyzed using the chi-square test or Fisher’s exact test, as appropriate. Variables with a significant relationship to massive IBL in univariate analysis were used in a binary logistic regression model. The correlation between the two parameters was analyzed using the Spearman rank-order method. Differences were considered significant at P < 0.05. Statistical analyses were performed using GraphPad Prism (v10.2.3; GraphPad Software, San Diego, CA; USA, https://www.graphpad.com).
Data preparation and splitting
The overall workflow is illustrated using a block diagram in Fig 1. The dataset comprised 73 features along with corresponding binary labels. Data preprocessing involved a stratified random split, allocating 70% of the data for training and 30% for testing. To ensure a robust evaluation across different random splits, this process was repeated 100 times using unique random seeds (random_state = rr, where rr = 0, 1,..., 99).
The study workflow and methodological process.
Backward feature selection and model optimization
To identify the most informative predictors of massive intraoperative bleeding, we applied backward stepwise feature selection within a logistic regression framework. Model optimization and evaluation were conducted using stratified 3-fold cross-validation, repeated across 100 random data splits to ensure generalizability. At each iteration, variables were progressively removed based on their contribution to model performance, assessed using the area under the receiver operating characteristic curve (AUC). The feature set yielding the highest validation AUC was selected as the final model. Details of the feature elimination procedure, coefficient ranking, and model tuning are provided in S1 File. All analyses were conducted using Python libraries including Scikit-learn and Pandas [16]. Run instructions are provided in S3 File. The analysis script is provided in S4 File.
Development of an online calculator for estimating the risk of massive aIBL
We developed an online calculator based on the final logistic regression model to estimate the probability of massive aIBL. To ensure model robustness, feature stability was evaluated across multiple random data splits using occurrence rate and absolute mean weight. The summarization script is provided in S5 File. Features consistently selected with strong predictive weights were incorporated into the final model. Prior to application, selected features were standardized and weighted using their regression coefficients to calculate the predicted probability of massive aIBL. The calculator is available at: https://tai1wakiya.shinyapps.io/ldlt_bleeding_ml/. Details of the feature selection metrics, weighting procedures, and standardization process are provided in S1 File.
Results
Clinical significance of massive aIBL
Among the 290 patients, those with aIBL greater than 80 mL/kg exhibited significantly higher rates of graft loss compared to those with lower aIBL (Fig 2). These findings support the clinical validity of using 80 mL/kg as a reasonable and actionable threshold for defining massive aIBL in LDLT.
Graft survival curve stratified by adjusted intraoperative bleeding volume using an 80 mL/kg cutoff.IBL, intraoperative bleeding; LDLT, living donor liver transplantation.
Comparison of patient characteristics in the massive aIBL and non-massive aIBL groups
The demographic data of the 290 enrolled patients are presented in Table 1, which also includes information on the IBL. Among all cases, massive aIBL was observed in 141 patients (48.6%). Except for indication and graft type, no significant differences were observed in the demographic data between the groups.
Table 1: Comparison of patient characteristics in the massive aIBL and non-massive aIBL groups.
Comparison of laboratory data in the massive aIBL and non-massive aIBL groups
Laboratory data are presented in Table 2. Significant differences (P < 0.05) were observed in 40 of the 55 laboratory test items between the two groups. To predict the occurrence of massive aIBL, we conducted a binary logistic regression analysis with the occurrence of massive aIBL as the dependent variable. Forty significant predictor variables associated with massive aIBL, identified using univariate analysis (P < 0.05), were included in the binary logistic regression analysis. The analysis identified total bile acids (P = 0.013, odds ratio [OR] = 1.010, 95% confidence interval [CI]: 1.000–1.010), albumin (P = 0.014, OR = 0.228, 95% CI: 0.071–0.736), and ammonia (P = 0.043, OR = 1.020, 95% CI: 1.000–1.050) as significant predictors of incidences of massive aIBL. However, as noted in S2 Table, there was significant multicollinearity among many factors in this analysis. The presence of multicollinearity can lead to instability in estimates, wider confidence intervals, and increased errors in coefficient estimates, complicating interpretation and potentially leading to incorrect conclusions. These results indicate that to construct a predictive model that exhibits multicollinearity with our dataset, it is crucial to select variables objectively, excluding subjectivity, and to utilize alternative analytical methods.
Table 2: Comparison of laboratory data in the massive aIBL and non-massive aIBL groups.
Correlations between preoperative laboratory tests and intraoperative bleeding volume
Next, we examined the relationship between the preoperative laboratory test results and aIBL. Of the 55 parameters tested, 42 showed significant correlations with the bleeding volume. Positive correlations were found for 43.6% of the parameters, whereas 56.4% exhibited negative correlations. The top five positively correlated biomarkers were D-dimer (r = 0.588), prothrombin time international normalized ratio (r = 0.495), total bilirubin (r = 0.461), direct bilirubin (r = 0.438), and total bile acids (r = 0.363). Conversely, antithrombin III (r = −0.560), alpha 2-plasmin inhibitor (r = −0.555), protein C (r = −0.527), prothrombin time percent (r = −0.495), and plasminogen (r = −0.458) were highly negatively correlated (Fig 3). These findings suggest that these markers can potentially guide preoperative assessment and intervention.
Correlations between preoperative laboratory tests and intraoperative bleeding volume. The left panel shows Spearman’s rank correlation coefficients, and the right panel shows p-values.All abbreviations and their units are listed in S1 Table.
Feature selection and model performance in logistic regression for massive aIBL prediction
We further explored a more robust prediction model for massive aIBL. We used the backward stepwise method for feature selection to construct our binary logistic regression model. During this process, we calculated the absolute magnitudes of the coefficients and removed the least influential covariates. This analysis incorporated laboratory variables as well as demographic data, including age, categorical age (under 6 years, 6–18 years, or 18 years and older), sex, body height, body weight, etiologies (ALF, BA, graft failure, or other), history of previous abdominal surgery, ABO incompatibility, rituximab desensitization, and graft type (LLS, LL, RL, RPS, reduced LLS, or monosegment). We started with all 73 features and systematically removed the least significant ones from the set. One of the representative feature selection processes is presented in S3 Table and S1 Fig. The process for narrowing down the variables is detailed in S3 Table. Antithrombin III was identified as the final covariate in the dataset. S1 Fig illustrates the performance of the model at each stage. The highest validation AUC of 0.867 was observed at the stage with 12 covariates. The AUC obtained in the test dataset was 0.728. To ensure a robust evaluation, this process was repeated 100 times across different random splits (S2 Fig). The average number of selected features across these 100 trials was 15.1. The average AUC in the validation and test datasets was 0.840 (standard deviation [SD] = 0.022) and 0.738 (SD = 0.046), respectively. These findings support a systematic approach for preoperatively predicting massive IBL in LDLT, suggesting the robustness and reliability of feature selection and model performance.
Identifying key predictors and constructing an online calculator for massive aIBL
To evaluate the consistency of selected features across 100 random data splits, index stability was assessed using occurrence rate and absolute mean weight (Fig 4). Based on the results from 100 iterations, features meeting the predefined criteria of an occurrence rate of at least 50% and an absolute mean weight of 0.5 or greater were selected. A total of 11 features were identified as robust predictors. Among them, six features exhibited positive mean weights, indicating a direct association with massive aIBL occurrence: D-dimer, ferritin, age, total bile acids, gamma-glutamyl transferase, and ammonia. Conversely, five features demonstrated negative mean weights, suggesting a potential protective effect: fibrinogen, platelet count, albumin, LLS graft, and antithrombin III. To enhance clinical applicability and ensure streamlined implementation, we developed a final prediction model for massive aIBL using these 11 selected features. In the test across all 290 cases, the model achieved an AUC of 0.844, with a sensitivity of 74.5%, specificity of 78.5%, positive predictive value of 76.6%, and negative predictive value of 76.5%. To further facilitate clinical adoption, we developed a user-friendly online calculator based on this risk model and made available online at: https://tai1wakiya.shinyapps.io/ldlt_bleeding_ml/.
Index stability across 100 iterations.The index is arranged in order of occurrence, sorted by mean weight. All abbreviations and their units are listed in S1 Table.
Discussion
In this study, we developed and validated ML models to predict massive IBL during LDLT. Using preoperative demographic and laboratory data, we employed logistic regression models with backward feature selection to achieve high predictive accuracy. Furthermore, we developed an online calculator that provides physicians with an accessible tool to estimate an individualized risk of massive IBL in the preoperative setting. To our knowledge, this is the first study to apply a ML model for IBL prediction in LT and to translate these findings into a clinically applicable prediction tool. The true innovation of this study lies not only in the excellent accuracy of the model but also in showcasing a groundbreaking artificial intelligence-based approach with significant future potential for management in LT.
Previous studies have attempted to predict bleeding and transfusion requirements in LT by using various clinical parameters and traditional standard statistical models [6–9]. While these studies have provided valuable insights, their models often exhibit suboptimal predictive performance and limited clinical applicability. Standard methods in clinical studies have several limitations, including the selection of variables, confounding factors, and multicollinearity, as demonstrated in this study. Even in prospective studies, the issue of multicollinearity remains a challenge to resolve. Furthermore, standard methods often fail to capture the complex, non-linear relationships between variables that significantly influence bleeding risk. In contrast, our study goes beyond traditional analyses by employing a data-driven approach, allowing us to systematically identify not only well-established risk factors but also previously unrecognized predictors.
Our study leveraged ML techniques, which are used to identify intricate patterns and interactions among multiple factors, demonstrating superior accuracy and robustness in predicting massive IBL. ML offers several key benefits, including increased accuracy through the simultaneous analysis of multiple variables and their interrelationships, and the ability to identify complex patterns and correlations that traditional methods might overlook. By incorporating a comprehensive set of preoperative variables and employing advanced feature selection methods, our ML models offer a more reliable and practical tool for preoperative risk stratification in LDLT. These models effectively manage complex, high-dimensional datasets, uncover hidden correlations, and explore non-linear medical relationships, enhancing predictive capabilities and potentially leading to new scientific insights.
Crucially, we went beyond model development by translating these findings into a tangible clinical tool. To ensure practical utility in real-world clinical settings, we developed an online calculator based on our predictive model, providing an accessible platform for physicians to rapidly assess massive IBL risk. This helps bridge the gap between advanced computational modeling and clinical decision-making, while integrating ML into clinical practice, which may contribute to improving patient outcomes and optimizing resource management.
Antithrombin III and ferritin emerged as significant predictors in our machine learning-based model, providing new insights into bleeding risk in LT. Antithrombin, a liver-derived serine protease inhibitor, is a key physiological anticoagulant with additional anti-inflammatory effects mediated through endothelial interactions [17]. In cardiovascular surgery, low preoperative antithrombin III levels have been consistently associated with increased intraoperative blood loss [18]. Mechanistically, reduced antithrombin activity allows excess thrombin and factor Xa activity, promotes systemic microthrombosis and a hypercoagulable state, and accelerates the consumption of coagulation factors, platelets, and antithrombin itself. Secondary fibrinolysis then ensues, leading to a bleeding tendency. Antithrombin supplementation can, in principle, interrupt this cycle by suppressing thrombin generation and indirectly support hemostasis through endothelial protection. However, clinical outcomes have been inconsistent across studies and meta-analyses [19–22]. Similarly, although the available studies are both dated and limited in number, evidence supporting a positive effect of antithrombin III supplementation in LT remains limited [23,24]. Therefore, while antithrombin appears useful as a biomarker for risk stratification, effective intervention in the LT setting will likely require targeting the early hypercoagulable phase with optimized dosing and timing rather than antithrombin restoration alone.
Regarding ferritin, no direct evidence has previously established its role in predicting bleeding in liver surgery, including LT. Ferritin reflects both iron metabolism and systemic inflammation, and its elevation may indicate a preoperative inflammatory state that predisposes patients to coagulopathy [25]. Iron overload induces oxidative stress through Fenton chemistry, which causes endothelial dysfunction and consequently promotes bleeding [26]. Inflammatory responses are known to disrupt hemostasis through mechanisms such as endothelial dysfunction, hyperfibrinolysis, and altered coagulation cascades [27]. Supporting this, our analysis identified a strong positive correlation between IBL and C-reactive protein, another established inflammatory marker; however, ferritin demonstrated greater stability as a predictive index than C-reactive protein. Together, these findings illustrate how machine learning can reveal biologically and clinically relevant predictors that are often overlooked by conventional approaches. Ferritin appears to be a useful biomarker for risk stratification, but interventional evidence is limited. No randomized controlled trial has shown that lowering ferritin through iron chelation reduces IBL in LT. Therefore, the benefit of iron-metabolism–targeted hemostatic strategies remains uncertain and warrants prospective evaluation.
This model was developed and calibrated in an LDLT cohort and is therefore positioned primarily for LDLT workflows; application to orthotopic liver transplantation (OLT) should be undertaken with caution. In settings where LDLT predominates, including Japan, OLT often represents a different case mix, with a higher prevalence of ALF and higher MELD scores, which may shift the relative importance of predictors. As a small exploratory check, we applied the LDLT model without recalibration to our 13 OLT recipients treated during the study period and obtained 9 of 13 correct classifications, corresponding to sensitivity 75%, specificity 60%, accuracy 69%, and AUC 0.694 (S4 Table). While this suggests some portability, broader applicability will require model updating on dedicated OLT datasets and, ideally, training and validation in mixed multicenter cohorts that include both OLT and LDLT.
The findings of this current study should be interpreted in light of several limitations. First, because fluid that accumulates intraoperatively can contain non-blood components, our measurement may slightly overestimate true blood loss. Although pre-existing ascites at laparotomy was excluded from IBL measurement, complete separation of blood from newly accumulated non-blood peritoneal fluid during surgery is difficult in routine practice. In anticipation of multicenter validation, standardizing IBL definitions and measurement across institutions would improve comparability and model transportability. Second, some clinically relevant factors could not be incorporated. For example, viscoelastic testing with ROTEM, which informs coagulopathy management, was not routinely available during the study period. These variables were therefore not included in feature selection. The candidate feature set warrants reconsideration in future work, and incorporating such additional features may further improve model discrimination and calibration. Third, it was a single-institution cohort study with a relatively small patient population, which limits generalizability. Additional training data could potentially enhance the prediction accuracy. Furthermore, the lack of external validation using an independent dataset is also a limitation. One reason for the absence of external validation is the argument made by some biostatistics experts in predictive research stating that independent verification can be misleading and should be omitted as a model evaluation step [28,29]. These experts report that simulations confirming at least 100 events and 100 non-events are required for a reliable assessment of predictive performance. They suggest using all available data for model development, with some form of cross-validation or bootstrap validation to assess the statistical optimism in average predictive performance [29,30]. Based on these biostatistical perspectives, we chose to build our ML model using all data with cross-validation, performing 100 iterations with randomly split datasets to ensure robustness and generalizability. However, we acknowledge that the results of predictive research with small sample sizes are exploratory in nature [29]. Nevertheless, external validation in various clinical settings, covering the heterogeneity among cases, is essential for clinical application. Given the high prediction accuracy of our method, further development using large databases, such as national or regional datasets, is expected and necessary.
Conclusions
Our study demonstrates the potential of ML to predict massive IBL during LDLT. These data-driven predictive models could revolutionize preoperative planning and intraoperative management, ultimately improving patient care and resource efficiency. As some predictors are exploratory, they should be interpreted cautiously until externally validated. Future research should focus on external validation using large datasets and the integration of these models into clinical practice.
Supporting information
S1 FigAUC by step in backward selection.AUC at each step of backward stepwise feature selection for the binary logistic regression model, shown for one representative iteration (one of 100 repetitions). AUC, area under the receiver operating characteristic curve.(TIF)
S2 FigBest performance across 100 runs.Model performance from backward feature selection repeated 100 times; the best-performing result is shown for each random split. AUC, area under the receiver operating characteristic curve.(TIF)
S1 TableList of abbreviations.(DOCX)
S2 TableList of variance inflation factors.(DOCX)
S3 TableBackward stepwise variable reduction.(DOCX)
S4 TablePerformance in OLT cases.(DOCX)
S1 FileSupplementary methods.(DOCX)
S2 FileDataset used in this study.(TXT)
S3 FileTechnical appendix – reproducibility and run guide.(TXT)
S4 FileSource code 1 – model training and validation.(PY)
S5 FileSource code 2 – feature selection and stability.(PY)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rana A, Petrowsky H, Hong JC, Agopian VG, Kaldas FM, Farmer D, et al. Blood transfusion requirement during liver transplantation is an important risk factor for mortality. J Am Coll Surg. 2013;216(5):902–7. doi: 10.1016/j.jamcollsurg.2012.12.047 23478547 · doi ↗ · pubmed ↗
- 2Yuasa T, Niwa N, Kimura S, Tsuji H, Yurugi K, Egawa H, et al. Intraoperative blood loss during living donor liver transplantation: an analysis of 635 recipients at a single center. Transfusion. 2005;45(6):879–84. doi: 10.1111/j.1537-2995.2005.04330.x 15934985 · doi ↗ · pubmed ↗
- 3Ramos E, Dalmau A, Sabate A, Lama C, Llado L, Figueras J, et al. Intraoperative red blood cell transfusion in liver transplantation: influence on patient outcome, prediction of requirements, and measures to reduce them. Liver Transpl. 2003;9(12):1320–7. doi: 10.1016/jlts.2003.50204 14625833 · doi ↗ · pubmed ↗
- 4Stokes EA, Wordsworth S, Staves J, Mundy N, Skelly J, Radford K, et al. Accurate costs of blood transfusion: a microcosting of administering blood products in the United Kingdom National Health Service. Transfusion. 2018;58(4):846–53. doi: 10.1111/trf.14493 29380872 · doi ↗ · pubmed ↗
- 5Ruiz J, Dugan A, Davenport DL, Gedaly R. Blood transfusion is a critical determinant of resource utilization and total hospital cost in liver transplantation. Clin Transplant. 2018;32(2):10.1111/ctr.13164. doi: 10.1111/ctr.13164 29193383 · doi ↗ · pubmed ↗
- 6Priem F, Karakiewicz PI, Mc Cormack M, Thibeault L, Massicotte L. Validation of 5 models predicting transfusion, bleeding, and mortality in liver transplantation: an observational cohort study. HPB (Oxford). 2022;24(8):1305–15. doi: 10.1016/j.hpb.2022.01.002 35131142 · doi ↗ · pubmed ↗
- 7Giabicani M, Joly P, Sigaut S, Timsit C, Devauchelle P, Dondero F, et al. Predictive role of hepatic venous pressure gradient in bleeding events among patients with cirrhosis undergoing orthotopic liver transplantation. JHEP Rep. 2024;6(6):101051. doi: 10.1016/j.jhepr.2024.101051 38699073 PMC 11060951 · doi ↗ · pubmed ↗
- 8Thibeault F, Plourde G, Fellouah M, Ziegler D, Carrier FM. Preoperative fibrinogen level and blood transfusions in liver transplantation: A systematic review. Transplantation Reviews. 2023;37(4):100797. doi: 10.1016/j.trre.2023.10079737778295 · doi ↗ · pubmed ↗