Screening a library of antibacterial compounds leads to discovery of novel inhibitors for Neisseria gonorrhoeae and Chlamydia trachomatis
Abdallah S. Abdelsattar, Nader S. Abutaleb, Mohamed N. Seleem, Yung-Fu Chang, Yung-Fu Chang, Yung-Fu Chang

TL;DR
Researchers screened compounds to find new drugs that can treat both Neisseria gonorrhoeae and Chlamydia trachomatis, which commonly cause STIs and are often resistant to current treatments.
Contribution
The study identified gloxazone and SPR719 as novel inhibitors effective against both N. gonorrhoeae and C. trachomatis.
Findings
Gloxazone and SPR719 showed potent activity against both N. gonorrhoeae and C. trachomatis with MICs ≤ 1 µM.
A library of 1,128 bioactive compounds was screened, leading to the identification of 172 active hits against N. gonorrhoeae.
Current treatments for these STIs are ineffective or face resistance, highlighting the need for new drugs like gloxazone and SPR719.
Abstract
Chlamydia trachomatis and Neisseria gonorrhoeae were the most common bacteria causing sexually transmitted infections (STIs) in 2020, with 211 million cases worldwide. Despite the fact that the co-infections of N. gonorrhoeae with C. trachomatis are common, there is no single treatment effective against both pathogens. Ceftriaxone, the current recommended drug for gonococcal infections, is not effective against C. trachomatis. Additionally, N. gonorrhoeae has developed resistance against the drugs recommended for treating chlamydial infections. Therefore, new drugs capable of treating C. trachomatis/N. gonorrhoeae co-infections are needed. Drug repurposing is an attractive, fast-track approach for antimicrobial drug discovery. In an attempt to address the unmet need for development of C. trachomatis/N. gonorrhoeae therapeutics utilizing the drug repurposing approach, we screened the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
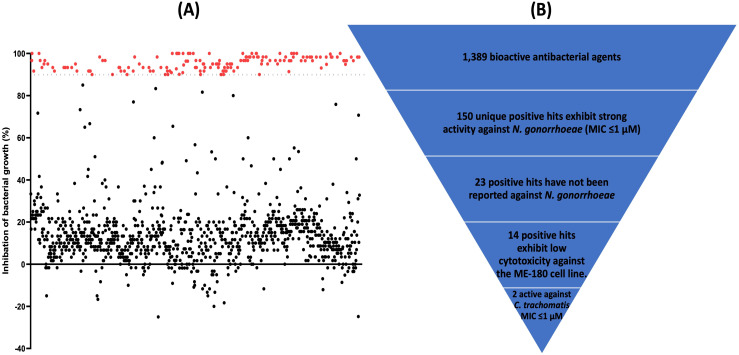 Fig 1
Fig 1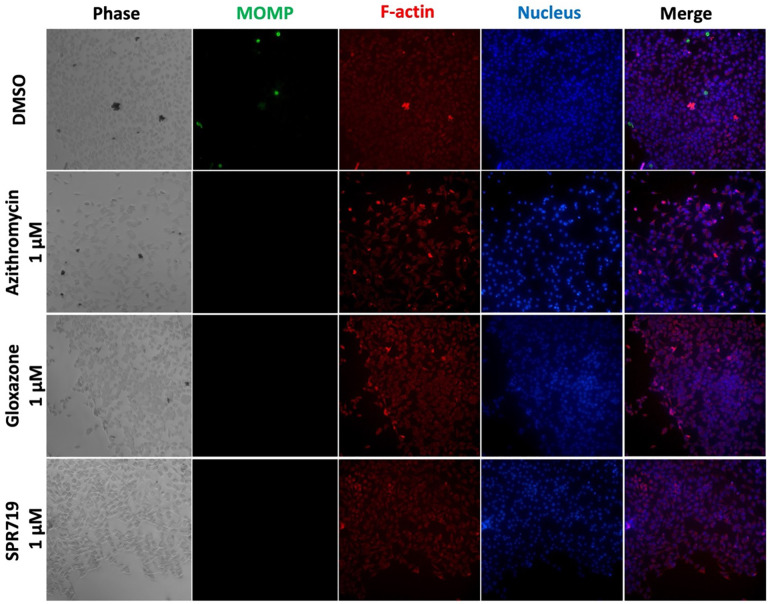 Fig 2
Fig 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReproductive tract infections research · Preterm Birth and Chorioamnionitis · Biochemical and Structural Characterization
1. Introduction
Sexually transmitted infections (STIs) greatly impact sexual and reproductive health globally, potentially causing serious issues, including genital ulcers, endocarditis, maternal mortality, pelvic inflammatory disease, infertility, lower abdominal pain, arthritis, and discharges from the urethra or vagina [1–5]. More than 1 million curable STIs are acquired daily worldwide in people aged 15–49 years, the majority of which are asymptomatic [6]. Bacterial STIs remain a globally significant public health problem, accounting for millions of infections annually. C. trachomatis and N. gonorrhoeae are the most prevalent bacterial STIs, with an estimated number of new cases of 129 and 82.4 million, respectively, in 2020 [6–8]. Infections caused by these bacteria can result in several medical complications, including infertility, ectopic pregnancy, eye inflammation, trachoma, arthritis, heart diseases, and perinatal mortality [9–13].
N. gonorrhoeae has progressively developed resistance to nearly all FDA-approved therapeutics. According to the Centers for Disease Control (CDC), azithromycin was removed from the guidelines of treating gonococcal infections, leaving ceftriaxone, as a single injection, as the only recommended drug for treatment of gonorrhea with no effective oral drug available [14–16]. However, over the last decade, gonococcal strains with ceftriaxone and high-level azithromycin resistance have begun to appear worldwide [17–20]. The increasing prevalence of antimicrobial resistance (AMR) in N. gonorrhoeae has led to the emergence of gonorrhea superbugs (also known as super gonorrhea), which could result in untreatable gonococcal infections globally in the future [21,22]. Gonorrhea superbugs are extensively drug-resistant N. gonorrhoeae with high-level resistance to not only ceftriaxone, but also to other classes such as penicillins, sulphonamides, tetracyclines, fluoroquinolones and macrolides (including azithromycin) [23]. Hence, in 2024, the WHO listed fluoroquinolone-resistant N. gonorrhoeae as a high-priority microorganism, surpassing methicillin-resistant Staphylococcus aureus (MRSA) [24]. Therefore, discovering effective and safe anti-N. gonorrhoeae therapies are a high priority globally.
C. trachomatis, an obligate intracellular pathogen, is the most common bacterium that causes STIs [7,8]. The current recommended treatment for C. trachomatis infections is doxycycline, especially among adolescents and adults [25]. Other alternative treatments, azithromycin and levofloxacin, have been associated with reported treatment failures and the emergence of resistance [26–28]. Co-infection rates of chlamydia and gonorrhea are estimated between 50% and 70%, and there is no single treatment effective for both pathogens [15,29]. Treating C. trachomatis/N. gonorrhoeae co-infections is challenging because doxycycline, the standard-of-care for chlamydia is ineffective against gonorrhea [15], and ceftriaxone, the current last-line treatment for gonorrhea, is ineffective against chlamydia [30,31]. In light of the above, there is an urgent need to identify an oral antibiotic effective against both C. trachomatis and N. gonorrhoeae.
Despite recent technological advances, the de novo process of discovering a novel drugs remains a complex and time-consuming task that could last for 15 years and cost an average of $2–3 billion [32]. However, one of the most promising and rapid strategies to combat the escalating AMR crisis is the repurposing of FDA-approved drugs. This approach has the potential of discovering new treatment options, offering a beacon of hope in the fight against gonorrhea [33]. The success of this strategy is evident in the repurposing of several drugs for antimicrobial use, such as doxycycline for malaria, amphotericin B and paromomycin for leishmaniasis [34–37], and spiramycin for toxoplasmosis [38]. The objective of the study was to conduct a rigorous screening of the antibacterial compounds library (HY-L049), which contains agents with confirmed bioactivity and safety, as demonstrated through preclinical and clinical trials, to identify potential agents against both N. gonorrhoeae and C. trachomatis. Additionally, the antibacterial activity of selected compounds was confirmed against N. gonorrhoeae and C. trachomatis strains*.*
2. Materials and methods
2.1. Bacterial strains and reagents
N. gonorrhoeae FA1090, C. trachomatis serovar L2 (ATCC VR-902B), and McCoy cell line were purchased from the American Type Culture Collection (ATCC). The media and supplements utilized in this work were purchased as follows: Phosphate-buffered saline (PBS) (Corning, NY, USA), nicotinamide adenine dinucleotide (NAD), pyridoxal, and hematin (Chem-Impex International, Wood Dale, IL, USA), and IsoVitaleX, brucella broth, chocolate II agar plates, and bovine hemoglobin, (Becton, Dickinson and Company, Cockeysville, MD, USA). Cycloheximide (Fisher Scientific, Fail Lawn, NJ, USA), C. trachomatis major outer membrane protein (MOMP) primary and secondary antibody (Bio-Rad, Hercules, CA, USA). Hoechst 33342 (MedChemExpress, Monmouth Junction, NJ, USA), azithromycin (TCI America, Portland, OR, USA), the phalloidin conjugates California red (AAT-Bioquest, Pleasanton, CA, USA) and Eagle’s Minimum Essential Medium (EMEM) (Sigma-Aldrich, St. Louis, MO, USA).
2.2. The antibacterial compounds library
The antibacterial compounds library (HY-L049), which contains a unique collection of 1,128 bioactive antibacterial compounds, was purchased from MedChemExpress (Princeton, Monmouth Junction, NJ, USA). The library was supplied in 96-well plates of 10 mM stocks of the drugs and clinical molecules dissolved in either dimethyl sulfoxide (DMSO), ethanol, or water.
2.3. Screening assay
The antibacterial compounds library was screened against N. gonorrhoeae FA1090 at a fixed concentration of 1 µM to evaluate anti-gonococcal activity as described previously [39–42]. Briefly, the N. gonorrhoeae FA1090 was grown on a chocolate II agar plate supplemented with IsoVitaleX. Single colonies were suspended in PBS and adjusted to a turbidity equivalent to 1 McFarland standard. Next, bacteria were diluted in Brucella broth supplemented with 1% IsoVitaleX to achieve a titer of about 1 × 10^6^ CFU/mL and added to 96-well plates containing the library drugs and clinical molecules (1 µM). Wells containing DMSO served as a growth control. The plates were incubated at 37°C in the presence of 5% CO_2_ for 24 h. Thereafter, SpectraMax i3 multi-mode microplate reader (Molecular Devices, Sunnyvale, CA, USA) was utilized to measure the OD_600_. The percentage of inhibition for each tested bioactive compound was calculated using the following equation.
Drugs and clinical molecules with an inhibition level of ≥90% were deemed as active hits, and their antibacterial activity was confirmed. GraphPad Prism 9.0 (Graph Pad Software, La Jolla, CA, USA) was utilized to illustrate the growth inhibition percentage.
2.4. Evaluation of MICs of the selected hits against N. gonorrhoeae
The selected hits were subsequently tested against N. gonorrhoeae FA1090 to confirm their MICs, using the broth microdilution method, as described previously [39–44]. Briefly, serial dilutions of the active hits and the control antibiotics (azithromycin and ceftriaxone) were incubated with bacterial solution (~ 1 × 10^6^ CFU/mL) at 37 °C in the presence of 5% CO_2_ for 24 h. The bacteria with DMSO served as a negative control. MICs were defined as the minimum concentrations of test agents that completely inhibited bacterial growth as determined by visual inspection of plates.
2.5. Investigation of the anti-chlamydial activity of selected hits
The anti-chlamydial activity of the selected hits was evaluated against C. trachomatis serovar L2 in McCoy cells, as previously described [45,46]. Briefly, the McCoy cell line was cultured in EMEM and incubated at 37°C with 5% CO_2_. Thereafter, cells were infected with C. trachomatis L2 (multiplicity of infection (MOI) = 1), in the presence of cycloheximide (1 μg/mL) for 2 hours. Subsequently, cells were treated with the test agents (1 μM). Azithromycin (1μM) and medium without antibiotics served as positive and negative controls, respectively. After 48 hours of treatment, the cells were stained with Hoechst 33342 for the DNA, phalloidin conjugated to California Red for the actin, in addition to C. trachomatis MOMP antibody and donkey anti-goat IgG conjugated to Alexa 488 as an indication for chlamydial inclusion. Finally, the images were taken using a Nikon Eclipse Ti2 inverted microscope (Nikon, Melville, NY, USA).
3. Results and discussion
3.1. Screening the antibacterial compounds library against N. gonorrhoeae
The antibacterial compounds library (containing 1,128 drugs and clinical molecules) was screened against N. gonorrhoeae FA1090, at a concentration of 1 µM, using the broth microdilution assay. Although the Clinical and Laboratory Standards Institute (CLSI) recommends the agar dilution method for antimicrobial susceptibility testing of N. gonorrhoeae, broth microdilution is used to screen drug libraries as established in a previously reported work [33]. The advantages of broth microdilution include its reproducibility, minimal sample requirement, low cost, and the ability to evaluate a large number of compounds [47]. The library screening identified 172 unique drugs and clinical molecules that inhibited the growth of N. gonorrhoeae FA1090 by more than 90% at 1 µM (S1 Table and Fig 1). In addition, 22 repeated drugs with different salts were eliminated. After analyzing the identified hits, we found that 127 had previously been reported against N. gonorrhoeae (S1 Table) and were therefore excluded. In addition, topical agents (such as antiseptics, surfactants, and fluorochrome agents), toxins, and anti-cancer agents were excluded, leaving 14 agents as promising hits.
Screening the antibacterial compounds library against N. gonorrhoeae FA1090.(A) Results of screening the antibacterial compounds library (containing 1,128 bioactive antibacterial agents), at a fixed concentration of 1 μM, against N. gonorrhoeae FA1090. Drugs exhibiting ≥ 90% inhibition of bacterial growth were considered positive hits (red). (B) Schematic of the screening process in this study, and the number of test agents at each step to finally obtain two molecules that are potent against N. gonorrhoeae and C. trachomatis.
The 14 agents identified, which were not previously reported against N. gonorrhoeae, were screened against N. gonorrhoeae FA1090, and their MICs were determined. They displayed potent activity against N. gonorrhoeae FA1090 with MIC values ranging from 0.008 μM to 1 µM (Table 1).
Table 1: MIC values of the selected hits against N. gonorrhoeae FA1090.
Beta-lactam antibiotics, which inhibit penicillin-binding proteins, thereby preventing the synthesis of peptidoglycan, are widely used in the management and treatment of bacterial infections due to their potent and broad-spectrum activity [48]. Currently, ceftriaxone, a beta-lactam antibiotic, is the only recommended treatment for N. gonorrhoeae infections [15,49,50]. Beta-lactam antibiotics make up about 65% of the total antibiotics market [51]. This could explain why the highest number of active hits (47) identified in our screening against N. gonorrhoeae belongs to the beta-lactam antibiotic class. Among these 47 beta-lactam antibiotic hits, two antibiotics were not previously reported against N. gonorrhoeae (aspoxicillin and ceftiofur). Aspoxicillin (TA-058) is an old semisynthetic penicillin compound that has a broad spectrum of activity against both Gram-positive and Gram-negative bacteria [52]. Aspoxicillin exhibited potent activity against N. gonorrhoeae FA1090 (MIC = 0.5 μM). Ceftiofur is FDA-approved for the treatment of mastitis in lactating dairy cattle by intramammary infusion [53]. Although ceftiofur has a lower MIC of 0.008 μM than aspoxicillin (0.5 μM), previous reports have demonstrated that the ability of Gram-negative bacteria to develop resistance against ceftiofur [54].
Macrolides, streptogramins, and phenicols are antibiotics that inhibit bacterial protein synthesis by binding to the bacterial 50S ribosomal subunit [55,56]. The macrolide antibiotic azithromycin was recommended in combination with ceftriaxone as the standard of care for the treatment of gonococcal infections until 2020 [16]. In addition, the CDC recommends a combination of azithromycin and gentamicin as an alternative treatment for uncomplicated gonococcal infection of the cervix, urethra, or rectum if a cephalosporin allergy is identified [15]. A total of 14 agents belonging to macrolides, streptogramins, and phenicols were identified as hits from our screening. Among these hits, two antibiotics were not previously reported against N. gonorrhoeae (azathramycin (desmethyl azithromycin) and virginiamycin M1). The MIC of azathramycin (MIC = 1 μM) was less effective than that of azithromycin (MIC = 0.25 μM) against the FA1090 strain. Furthermore, virginiamycin M1, a polyunsaturated macrocyclic lactone produced by Streptomyces virginiae, belonging to the streptogramin A group [57], exhibited a potent activity similar to that of azithromycin against N. gonorrhoeae FA 1090. Virginiamycin is widely used as a growth promoter and for the prevention and treatment of infections in farm animals.
The antibacterial activity of pleuromutilin derivatives is mediated by inhibiting bacterial protein synthesis after binding to the bacterial 50S ribosomal subunit [58,59], similar to azithromycin. However, earlier reports have indicated a slight difference in activity against azithromycin-resistant bacteria due to differences in binding sites [60–62]. Recently, lefamulin, a pleuromutilin derivative, has been assessed as a potential drug against STIs, including N. gonorrhoeae and Chlamydia trachomatis [63].
Recently, greater attention has been given to drugs that inhibit DNA synthesis in N. gonorrhoeae, such as zoliflodacin and gepotidacin [64]. Additionally, ciprofloxacin was one of the recommended treatments for N. gonorrhoeae until 2007 [65]. Among the 14 non-previously reported identified hits, four drugs belonging to the fluoroquinolones were identified (marbofloxacin, orbifloxacin, levonadifloxacin, and fluoroquinolonic acid), which showed an MIC range of 0.032–0.064 μM against N. gonorrhoeae FA1090. Marbofloxacin and orbifloxacin were approved by the FDA for the treatment of infections in dogs and cats [66,67]. Recently, levonadifloxacin was approved in India as an oral and injectable drug for the treatment of acute bacterial skin and skin structure infections [68,69]. In addition, fluoroquinolonic acid was identified as a ciprofloxacin impurity with inhibitory effect against E. coli MG1655 at a low concentration of 0.064 μg/mL [70].
Nitrofurans are a class of nitroaromatic antibacterial agents that require activation inside bacterial cells to form reactive intermediates that damage macromolecules. This reactivation is performed by the bacterial flavoprotein nitrofuran reductase which reduces the nitrofuran antibiotic and its derivatives to a reactive form, which then inhibits the synthesis of DNA, RNA, and proteins [71]. The analysis of the positive hists revealed 6 active hits from the nitrofurans class, 3 of which were not previously investigated against N. gonorrhoeae (furaltadone, nifursol, and nifurpirinol). They displayed potent activity against N. gonorrhoeae with MIC values of 1 μM (Table 1).
In addition to the previously identified hits, we identified other 5 active drugs and clinical molecules which were not reported before against N. gonorrhoeae (nigericin, SPR719, antibacterial agent 18, walrycin B, and gloxazone), with MIC values ranging from 0.06 to 1 μM. Nigericin, a polyether ionophore antibiotic, which was reported to have bactericidal activity against both Gram-positive and Gram-negative bacteria by disrupting the ionic balance [72,73]. Nigericin inhibited N. gonorrhoeae FA1090 at an MIC value of 0.5 μM. Additionally, SPR719 a novel benzimidazole antibiotic that inhibits the ATPase activity of the DNA gyrase (GyrB) and topoisomerase IV (ParE) in mycobacteria [74]. SPR720 is in clinical development for the treatment of non-tuberculous mycobacterial pulmonary disease (NTM-PD) and pulmonary tuberculosis [75]. SPR719 and its prodrug, SPR720, showed remarkable safety, tolerability, and pharmacokinetics results in clinical trials (NCT03796910) [76]. SPR719 demonstrated a potent anti-gonococcal activity, inhibiting the tested N. gonorrhoeae strain at a concentration of 0.125 μM. Furthermore, antibacterial agent 18 was previously reported as an active compound against Gram-negative bacterial pathogens, with an MIC ranging from 0.125 to 1 μg/mL, by disrupting their cell wall synthesis via hindering transpeptidation and glycosylation [77]. Antibacterial agent 18 showed an MIC value of 1 μM against N. gonorrhoeae FA1090. Additionally, the analysis of the positive hits revealed a potent activity of walrycin B against N. gonorrhoeae FA1090 (MIC = 0.5 μM). Walrycin B is an antibacterial compound that has been shown to target the WalK/WalR two-component signal transduction system, which is essential for the viability of many Gram-positive bacteria. This inhibition leads to the inhibition of crucial genes required for cell wall synthesis and coordinating cell division [78]. Furthermore, gloxazone, an effective drug against anaplasmosis [79], exhibited potent activity against N. gonorrhoeae FA1090 (MIC = 0.06 μM) (Table 1).
3.2. Activity of the selected positive hits against C. trachomatis
Co-infection rates of chlamydia and gonorrhea are high. Women with gonorrhea are co-infected with chlamydia in 17.6% – 57.9% of cases, while women with chlamydia are co-infected with gonorrhea in 2.1% – 17.2% of cases [30,31,80,81]. Moreover, during the co-infection, N. gonorrhoeae can induce C. trachomatis to enter a difficult-to-treat persistence-like state [80]. Since treating N. gonorrhoeae/C. trachomatis co-infections are challenging because there is no available drug effective against both pathogens. It was also reported that treatment with non-specific antibiotics can increase rates of N. gonorrhoeae resistance [82,83]. Hence, the search for an oral antibiotic targeting both pathogens cannot be overemphasized. Therefore, we sought to investigate the activity of the selected hits from our screening against C. trachomatis L2. Agents with reported toxicity, including walrycin B [84], and Nigericin [85] were excluded. We have also excluded the active hits belonging to known classes of antibiotics (beta-lactams, macrolides, fluoroquinolones, and nitrofurans). We selected only 2 hits (SPR719, and gloxazone) to evaluate their activity against C. trachomatis. We screened their activity, at a fixed concentration of 1 μM, against C. trachomatis L2 infecting McCoy cells*.* SPR719 and gloxazone displayed potent activity against C. trachomatis, completely clearing the bacteria at the tested concentration (MIC ≤ 1 μM) (Fig 2). The addition of SPR719, gloxazone, or azithromycin at a fixed concentration (1 μM) completely blocked the development of C. trachomatis inclusion bodies. However, the negative control (DMSO) shows the mature inclusions after 48 hours. Inclusion bodies were identified using primary antibodies bound to Chlamydia MOMPs and a secondary antibody conjugated to Alexa 488, which appears as green circles (Fig 2). We recommend further in vitro studies to assess the inhibitory effects of hit compounds (gloxazone and SPR719) on both N. gonorrhoeae and C. trachomatis simultaneously in a co-culture assay [86].
Immunofluorescence images showing the inhibitory effects of SPR719 and gloxazone (at a fixed concentration of 1 μM).McCoy cells were infected and incubated for 2 hours before being exposed to SPR719 and gloxazone (at 1 μM), and incubated for 48 hours at 37°C with 5% CO2. Azithromycin at 1 μM was used as a positive control. The untreated cells (DMSO) served as a negative control. Nuclear DNA was stained with Hoechst 33342 (blue), primary antibodies bound to the MOMPs of Chlamydia were stained with donkey anti-goat IgG conjugated to Alexa 488 (green), and phalloidin conjugated to California red was used to stain F-actin (red).
Conclusion
In conclusion, this study aims to identify new therapeutics for N. gonorrhoeae and C. trachomatis through repurposing existing drugs and compounds in clinical trials. Screening a library of antibacterial compounds led to the discovery of novel lead molecules, such as SPR719 and gloxazone, that possess potent in vitro anti-N. gonorrhoeae activity. They also showed potent activity against C. trachomatis. These agents warrant further investigation for the development of new anti-C. trachomatis/N. gonorrhoeae therapeutics.
Supporting information
S1 TableThe positive hit compounds against N. gonorrhoeae FA1090.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Masi AT, Eisenstein BI. Disseminated gonococcal infection (DGI) and gonococcal arthritis (GCA): II. Clinical manifestations, diagnosis, complications, treatment, and prevention. Semin Arthritis Rheum. 1981;10(3):173–97. doi: 10.1016/s 0049-0172(81)80002-9 6785887 · doi ↗ · pubmed ↗
- 2Burnett AM, Anderson CP, Zwank MD. Laboratory-confirmed gonorrhea and/or chlamydia rates in clinically diagnosed pelvic inflammatory disease and cervicitis. Am J Emerg Med. 2012;30(7):1114–7. doi: 10.1016/j.ajem.2011.07.014 22030186 · doi ↗ · pubmed ↗
- 3Jensen JS, Unemo M. Antimicrobial treatment and resistance in sexually transmitted bacterial infections. Nat Rev Microbiol. 2024;22(7):435–50. doi: 10.1038/s 41579-024-01023-3 38509173 · doi ↗ · pubmed ↗
- 4Emergence of multi-drug resistant Neisseria gonorrhoeae - threat of global rise in untreatable sexually transmitted infections fact sheet. [Cited 2025 June 7]. https://www.who.int/publications/i/item/emergence-of-multi-drug-resistant-neisseria-gonorrhoeae---threat-of-global-rise-in-untreatable-sexually-transmitted-infections-fact-sheet
- 5Geisler WM, Chow JM, Schachter J, Mc Cormack WM. Pelvic examination findings and Chlamydia trachomatis infection in asymptomatic young women screened with a nucleic acid amplification test. Sex Transm Dis. 2007;34(6):335–8. doi: 10.1097/01.olq.0000240344.20665.63 17028510 · doi ↗ · pubmed ↗
- 6Sexually transmitted infections (ST Is). [Cited 2025 June 7]. https://www.who.int/news-room/fact-sheets/detail/sexually-transmitted-infections-(stis)
- 7Gonorrhoea (Neisseria gonorrhoeae infection). [Cited 2024 August 14]. https://www.who.int/news-room/fact-sheets/detail/gonorrhoea-(neisseria-gonorrhoeae-infection)
- 8Chlamydia. [cited 19 May 2025]. https://www.who.int/news-room/fact-sheets/detail/chlamydia