An Unusual Suspect: Right Hypochondrium Pain in the Third Trimester of Pregnancy
Dina Jleilati, Romain Gillard

TL;DR
This paper discusses a rare case of right hypochondrium pain in a pregnant woman caused by adrenal vein thrombosis.
Contribution
It highlights the importance of considering adrenal vein thrombosis in pregnant patients with unexplained unilateral adrenal enlargement.
Findings
Adrenal vein thrombosis can present as unexplained unilateral adrenal enlargement in pregnancy.
Early diagnosis and anticoagulant management can prevent adrenal insufficiency.
Abstract
Teaching point: Adrenal vein thrombosis should be considered in pregnant patients presenting with unexplained unilateral adrenal enlargement, even when the thrombus itself is not visualized, as early diagnosis allows effective anticoagulant management and prevention of adrenal insufficiency.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
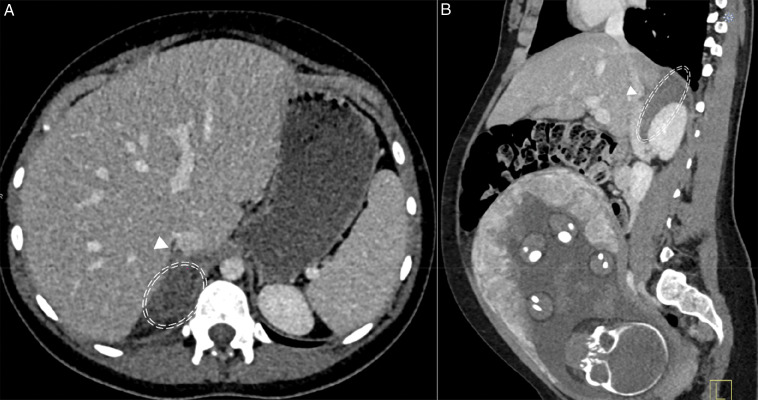 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdrenal and Paraganglionic Tumors · Adrenal Hormones and Disorders · Hormonal Regulation and Hypertension
Right Adrenal Vein Thrombosis in the Third Trimester of Pregnancy
Case
A 28-year-old woman at 32 weeks of pregnancy presented with acute right upper-quadrant abdominal pain radiating to the back. She had no urinary or gastrointestinal symptoms and was afebrile. Physical examination revealed localized right-sided tenderness without peritoneal signs. The obstetric assessment was normal. Laboratory tests showed elevated CRP and moderate leukocytosis. An initial ultrasound revealed no abnormalities. Because the pain persisted and inflammatory markers remained elevated, a contrast-enhanced CT scan was performed. The CT demonstrated an enlarged hypodense right adrenal gland with periadrenal fat stranding. A filling defect extending from the right adrenal vein into the inferior vena cava (IVC) was identified, confirming the diagnosis of right adrenal vein thrombosis. Figures 1A and 1B show an axial (a) and sagittal (b) plane abdominal CT at portal phase showing poor enhancement and swollen appearance of the right adrenal gland (circle) and hypodense filling defect within the IVC (arrowhead), corresponding to the adrenal vein thrombosis overflowing in the IVC. Therapeutic anticoagulation with enoxaparin was initiated, resulting in progressive resolution of symptoms.
Axial (A) and sagittal (B) plane abdominal CT at portal phase showing poor enhancement and swollen appearance of the right adrenal gland (circle) and hypodense filling defect within the inferior vena cava (arrowhead), corresponding to the adrenal vein thrombosis overflowing in the inferior vena cava.
Postpartum thrombophilia screening demonstrated persistently elevated factor VIII levels and a heterozygous G20210A prothrombin gene mutation, supporting an underlying inherited thrombophilia. Anticoagulation was continued for six weeks postpartum.
Comment
Adrenal vein thrombosis is a rare but clinically significant cause of acute abdominal pain, particularly in pregnant patients in the third trimester. Its presentation is often non-specific and overlaps with several more common differentials, making timely diagnosis challenging.
Its true incidence is likely underestimated because imaging is required for diagnosis, and the condition may be misattributed to more common causes of abdominal pain in pregnancy. The right adrenal gland is disproportionately affected owing to its direct drainage into the IVC and the increased venous stasis induced by uterine compression during late gestation. Progression to adrenal insufficiency is rare because bilateral involvement is exceptional [1].
Imaging plays a key diagnostic role. The thrombus is often not directly visualized; therefore, the diagnosis relies on characteristic indirect signs. CT typically shows unilateral adrenal enlargement, parenchymal hypoattenuation, and periadrenal fat stranding. When visible, a filling defect in the adrenal vein or IVC confirms thrombosis (Figures 1A and 1B). MRI can be used to avoid fetal radiation and may demonstrate findings consistent with edema, infarction, or hemorrhage [1].
Awareness of this diagnosis in cases of unexplained adrenal swelling is essential, even in the absence of direct thrombus visualization. It helps ensure prompt management and good maternal-fetal outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.