Cervical Osteophytosis Causing Tracheomalacia and Dyspnea
Laith Fada, Emma Karesh, John Wahidy, Shawn Clark

TL;DR
A rare case shows how cervical osteophytosis from DISH can cause tracheomalacia, leading to breathing difficulties that were resolved through surgery.
Contribution
Reports a rare clinical case linking cervical osteophytosis to tracheomalacia and successful surgical treatment.
Findings
Cervical osteophytosis from DISH caused localized tracheomalacia and airway obstruction.
Surgical removal of osteophytes improved airway function and resolved symptoms.
Bronchoscopy and imaging are essential for diagnosing tracheomalacia in such cases.
Abstract
Cervical osteophytosis, a common manifestation of degenerative spondylosis, can rarely exert mass effect to compromise adjacent airway structures. Acquired tracheomalacia secondary to anterior cervical osteophytes is exceptionally uncommon and results from dynamic airway collapse due to weakened tracheal cartilaginous support. Tracheomalacia may present with nonspecific respiratory symptoms such as dyspnea, cough, and orthopnea, and diagnosis is best established with direct visualization on bronchoscopy. We report a rare case of localized upper tracheal tracheomalacia caused by cervical diffuse idiopathic skeletal hyperostosis (DISH) with severe anterior osteophyte formation, resulting in clinically significant airway obstruction. A 74-year-old male with a history of coal worker’s pneumoconiosis, osteoarthritis, DISH, and prior lumbar spine surgery presented with a six-year history of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
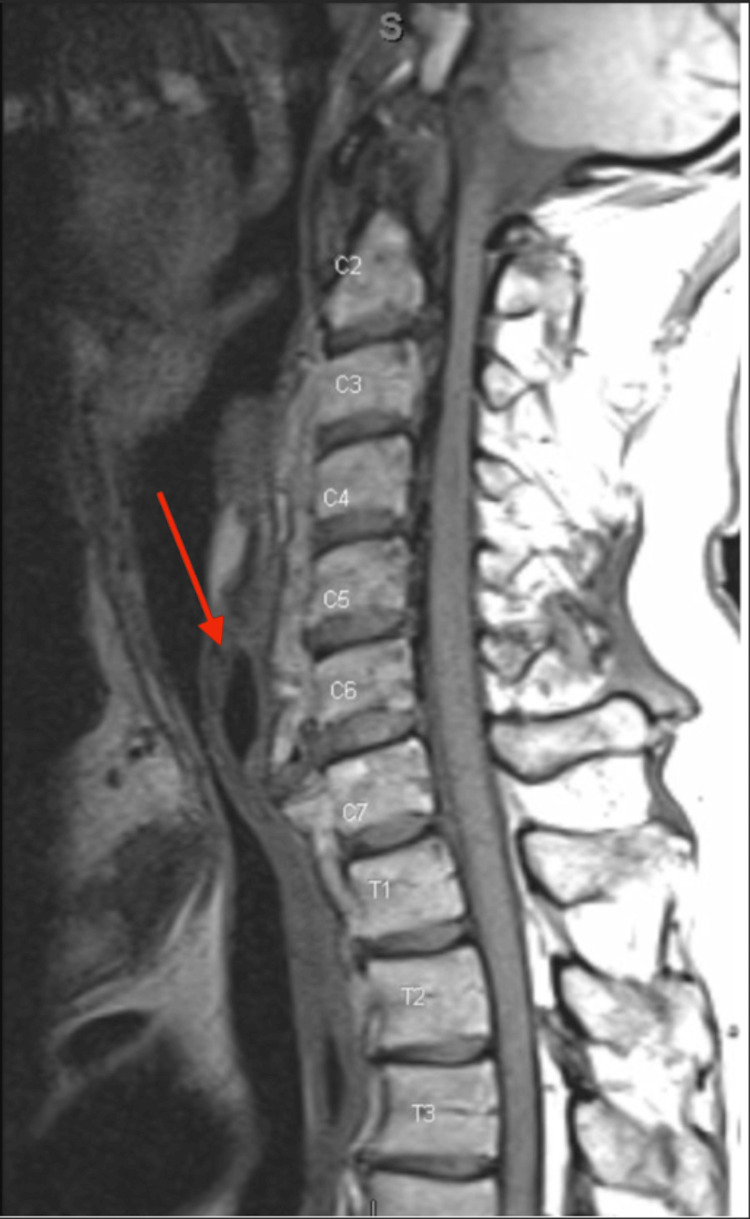 Figure 1
Figure 1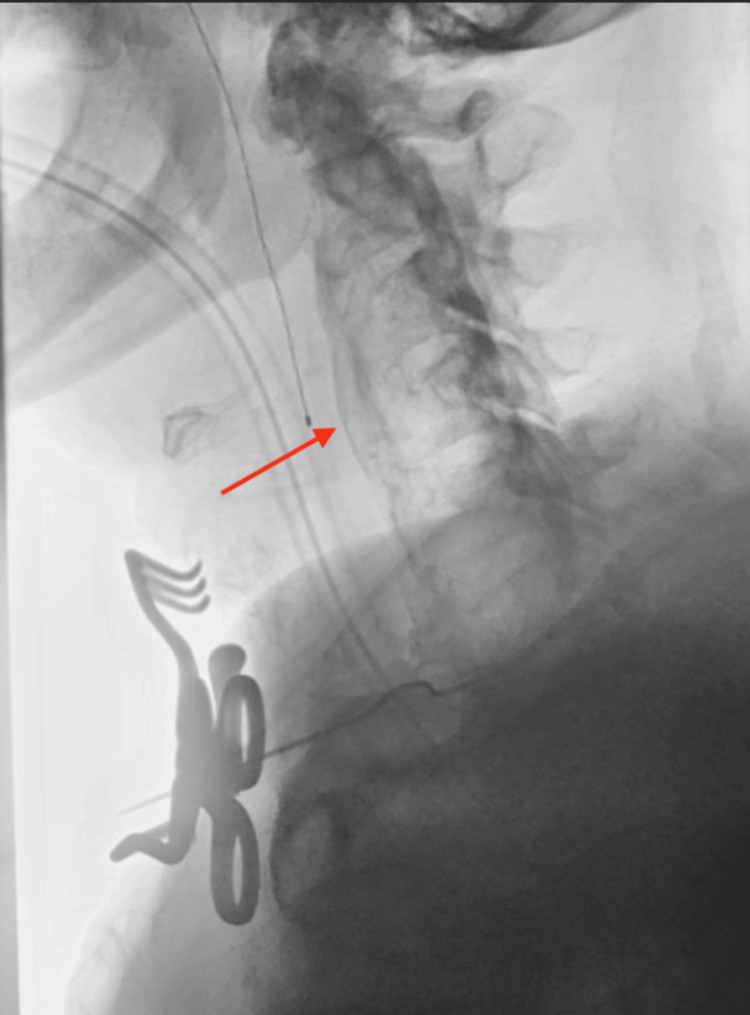 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCervical and Thoracic Myelopathy · Spondyloarthritis Studies and Treatments · Heterotopic Ossification and Related Conditions
Introduction
Cervical osteophytosis is a manifestation of degenerative spondylosis in which chronic spinal degeneration leads to the formation of bony outgrowths, or osteophytes, along the vertebral margins. While these osteophytes most commonly cause local pain or neurologic symptoms, they can rarely exert a mass effect - defined as direct physical compression - on adjacent structures, including the esophagus and airway. We present an unusual case of acquired tracheomalacia resulting from chronic compression of the trachea by a large anterior cervical osteophyte at the C3-C6 levels.
Tracheomalacia is a condition characterized by abnormal weakness of the tracheal cartilaginous framework, leading to excessive airway collapsibility during respiration. Depending on the underlying cause, tracheomalacia may be classified as diffuse or localized, with localized disease often resulting from prolonged external compression [1]. Common presenting symptoms are nonspecific and include cough, dyspnea, orthopnea, and, in more advanced cases, audible stridor. The patient in this case reported progressive dyspnea over six to seven years and was noted to have stridor on physical examination.
The pathophysiology of acquired tracheomalacia involves chronic mechanical stress on the trachea, which leads to cartilage weakening and laxity of the posterior tracheal wall, resulting in dynamic airway narrowing during expiration. One potential cause of such chronic compression is diffuse idiopathic skeletal hyperostosis (DISH), a noninflammatory condition characterized by excessive ossification of spinal ligaments and entheses, most commonly affecting the cervical spine. Bronchoscopy remains the diagnostic gold standard, as it allows direct visualization of dynamic airway collapse [2]. In this case, bronchoscopy demonstrated tracheomalacia localized to the upper trachea, while magnetic resonance imaging revealed severe cervical DISH with anterior ossification and spinal stenosis. The patient was subsequently referred to neurosurgery and underwent surgical excision of the offending osteophyte.
Case presentation
A 74-year-old male with a history of coal worker’s pneumoconiosis, longstanding osteoarthritis, diffuse idiopathic skeletal hyperostosis, and previous lumbar spine surgery presented with a six-year history of progressive dyspnea, recently advancing to audible stridor at rest. He presented with worsening exertional limitations and dyspnea, but denied dysphagia, orthopnea, or other red-flag symptoms. He had a 40-year smoking history but quit in 2001.
Bronchoscopic evaluation revealed dynamic upper tracheal narrowing with collapse of the posterior tracheal wall consistent with localized tracheomalacia. Cross-sectional imaging, using MRI (Figure 1) and X-ray (Figure 2), demonstrated prominent anterior cervical osteophytes extending from C5 to C7, causing posterior tracheal and esophageal compression, as well as spinal stenosis from C1-C6.
MRI of the cervical spine demonstrating extensive anterior osteophyte formation at C5–C7 (arrow).
X-ray demonstrating causing posterior displacement of the trachea and esophagus (arrow).
Given the patient’s progressive airway symptoms and imaging findings, a multidisciplinary discussion concluded that surgical intervention was indicated to relieve airway obstruction and prevent further tracheal compromise. The patient underwent an anterior cervical approach with microsurgical removal of the C5-C7 anterior osteophytes, followed by posterior decompressive laminectomy (C1-C6) with partial facetectomies and foraminotomies for concurrent spinal stenosis. Intraoperative microscopy and fluoroscopy confirmed complete resection of the osteophytic mass.
Postoperatively, the patient demonstrated resolution of stridor and improved respiratory effort, with stable airway patency and no new neurological deficits. He participated in early physical therapy and was discharged home with outpatient rehabilitation. At follow-up, the patient remained free of airway compromise and reported significant improvement.
Discussion
This case illustrates a rare presentation of tracheomalacia caused by cervical osteophytes due to Diffuse Idiopathic Skeletal Hyperostosis (DISH). While DISH can lead to ossification of spinal ligaments, airway obstruction and tracheomalacia are rare outcomes. Studies from 2011 showed that cervical osteophytes can lead to airway compromise via outward compression of the trachea [3]. Our patient's presentation shows noticeable C5-C7 osteophytes that likely led to chronic compression of the tracheal wall, leading to eventual tracheomalacia and dysphagia. This mechanism stresses the significance of dynamic airway evaluation via MRI imaging to explore the several possibilities of what may be causing the patient's symptoms.
Surgical management is the best way to treat airway obstruction from DISH when conservative measures fail. One report indicates that surgical excision of osteophytes along the anterior longitudinal ligament can help relieve dysphagia and respiratory distress [4]. The decision to perform an anterior cervical approach along with a posterior decompressive laminectomy led to the resolution of the airway compromise and spinal stenosis. This approach is not commonly found in literature, however, it presents the favorable outcome of resolving patients' symptoms via surgical intervention.
Airway evaluation (via imaging or bronchoscopy) should be considered in all patients presenting with cervical DISH to explain possible dyspnea, dysphagia, or stridor that the patient may present with. Early recognition of airway involvement in these patients can prevent serious respiratory compromise in those who elect to undergo surgical intervention to resolve their symptoms. A multidisciplinary approach should be used in surgical planning, given the complex anatomic and physiologic dynamics that are involved.
Conclusions
This case presents a rare example of tracheomalacia developing in the setting of diffuse idiopathic skeletal hyperostosis (DISH), highlighting the potential for chronic anterior cervical osteophyte compression to progressively weaken tracheal cartilaginous support. Such airway compromise may mimic more common pulmonary or cardiac pathologies, often leading to delayed diagnosis and prolonged morbidity. Early recognition of tracheomalacia in patients with advanced cervical osteophytosis is therefore critical, particularly when respiratory symptoms are unexplained or progressive. Prompt multidisciplinary evaluation and timely intervention can be lifesaving, prevent irreversible airway collapse, and significantly improve functional and respiratory outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Current concepts in severe adult tracheobronchomalacia: evaluation and treatment J Thorac Dis Buitrago DH Wilson JL Parikh M Majid A Gangadharan SP 09201710.21037/jtd.2017.01.13PMC 530306728203438 · doi ↗ · pubmed ↗
- 2Tracheomalacia Chest Surg Clin N Am Wright CD 3493571320031275531910.1016/s 1052-3359(03)00036-x · doi ↗ · pubmed ↗
- 3Diffuse idiopathic skeletal hyperostosis of the cervical spine: an underestimated cause of dysphagia and airway obstruction Spine J Verlaan JJ Boswijk PF de Ru JA Dhert WJ Oner FC 105811671120112201523610.1016/j.spinee.2011.09.014 · doi ↗ · pubmed ↗
- 4Diffuse idiopathic skeletal hyperostosis causes acute airway obstruction following upper respiratory tract infection: a case report Spine Surg Relat Res Kumamoto S Honke H Higuchi K Inoue T Mawatari M 114116520213384272010.22603/ssrr.2020-0063 PMC 8026211 · doi ↗ · pubmed ↗