Quad Fever After a Traumatic Cervical Spinal Cord Injury: Diagnostic Challenges and Therapeutic Response to Bromocriptine
Rita Bragança, Mariana Esteves, Paulo Carrola

TL;DR
A rare condition called quad fever, causing extreme non-infectious fever after spinal injury, was successfully treated with bromocriptine in a 72-year-old woman.
Contribution
This case report demonstrates bromocriptine's effectiveness in treating quad fever, a rare and often misdiagnosed condition after spinal cord injury.
Findings
Quad fever was diagnosed after ruling out infections and other causes in a patient with C4-C5 spinal injury.
Bromocriptine administration led to rapid and sustained resolution of high fevers within 24 hours.
The patient successfully continued rehabilitation and was discharged in good condition after treatment.
Abstract
Quad fever is a rare, potentially fatal form of neurogenic hyperpyrexia occurring after high cervical or upper thoracic spinal cord injury (SCI) and is frequently misdiagnosed as severe infection. It is characterised by extreme, non-infectious hyperthermia resulting from autonomic and central thermoregulatory dysfunction. We report the case of a previously healthy 72-year-old woman who sustained a traumatic C4-C5 SCI and developed abrupt postoperative hyperpyrexia (40.9 °C) within 12 hours of anterior cervical decompression and fusion. Despite antipyretics, broad-spectrum antibiotics, and physical cooling, daily high-grade fevers persisted. An extensive evaluation excluded infectious, inflammatory, endocrine, neoplastic, and hardware-related causes, with normal inflammatory markers and sterile cultures. Based on the clinical context and exclusion of alternative etiologies, a diagnosis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
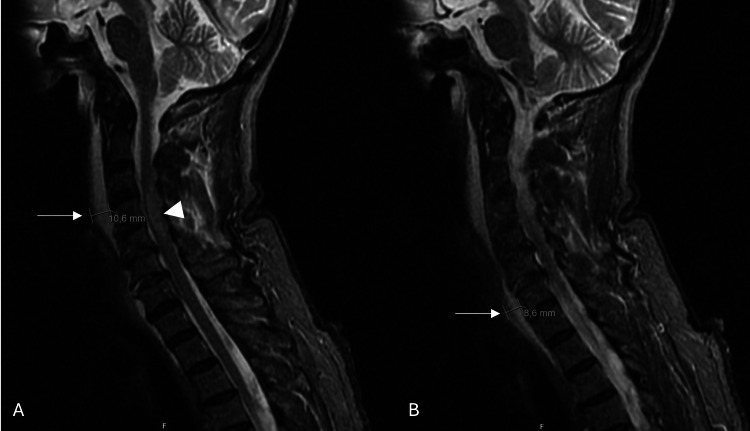 Figure 1
Figure 1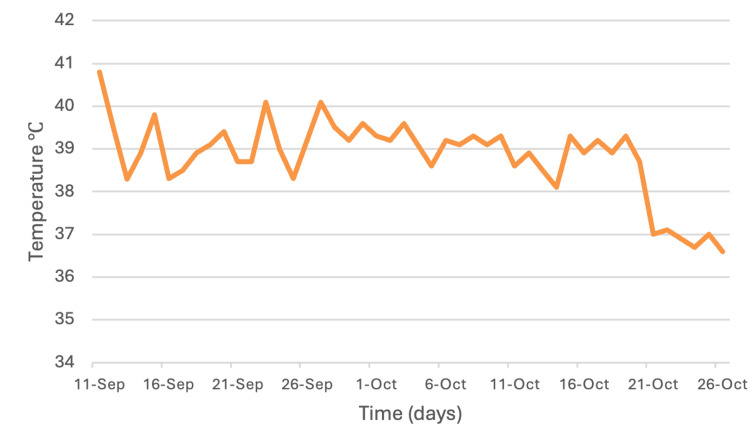 Figure 2
Figure 2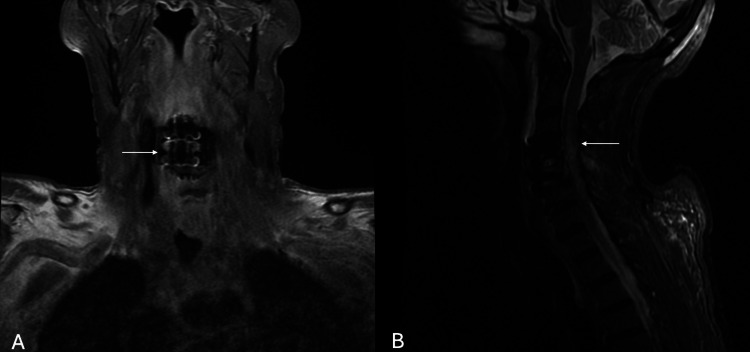 Figure 3
Figure 3| Parameter | Result | Reference value |
| Hematology/Inflammation | ||
| Blood smear | Normocytic anemia | — |
| C-reactive protein | <0.5 mg/dL | <0.5 mg/dL |
| ESR | 20 mm/1st h | 0–30 mm/1st h |
| Hemoglobin | 10.9 g/dL | 12–16 g/dL |
| Peripheral blood immunophenotyping | Small-sized lymphoid population without immunophenotypic alterations suggestive of lymphoproliferative disease | — |
| Procalcitonin | 0.1 ng/mL | <0.5 ng/mL |
| White blood cells | 6.59×10³/µL | 4.00–11.00×10³/µL |
| Neutrophils | 4.44×10³/µL | 2.00–7.50×10³/µL |
| Lymphocytes | 1.60×10³/µL | 1.50–4.00×10³/µL |
| Monocytes | 0.40×10³/µL | 0.20–0.80×10³/µL |
| Eosinophils | 0.11×10³/µL | 0.04–0.40×10³/µL |
| Basophils | 0.05×10³/µL | 0.02–0.10×10³/µL |
| Biochemistry/Metabolism | ||
| ACTH | 58.2 | < 63.3 ng/L |
| Angiotensin-converting enzyme | 29 U/L | 6–52 U/L |
| C3c | 126 mg/dL | 90–180 mg/dL |
| C4 | 25 mg/dL | 12–36 mg/dL |
| Creatine kinase | 104 | — |
| Free thyroxine (free T4) | 17.2 pmol/L | 8.2–21 pmol/L |
| Free triiodothyronine (free T3) | 3.2 pmol/L | 3.1–6.8 pmol/L |
| IgA | 910 mg/dL | 600–1570 mg/dL |
| IgE | 847 (↑) UI/mL | <100 UI/mL |
| IgG | 271 mg/dL | 50–373 mg/dL |
| IgM | 101 mg/dL | 40–325 mg/dL |
| Serum ferritin | 312 ng/mL | 15–150 ng/mL |
| Serum iron | 64 µg/mL | 37–145 µg/mL |
| Serum protein electrophoresis | No monoclonal peaks | — |
| Total iron-binding capacity | 164 mg/dL | 228–360 mg/dL |
| Transferrin saturation | 39% | >20% |
| Triglycerides | 129 mg/dL | <150 mg/dL |
| TSH | 1.25 mIU/L | 0.27–4.2 mIU/L |
| Vitamin B12 | 219 pg/mL | 191–663 pg/mL |
| β2-microglobulin | 1.3 µg/mL | 0.8–2.2 µg/mL |
| Parameter | Result | Reference value |
| Immunology/Autoimmunity | ||
| Anti-cardiolipin antibodies (IgG/IgM) | Negative | — |
| Anti-myeloperoxidase antibody | <0.2 U/mL | <3.5 U/mL |
| Anti-phospholipid antibodies (IgG/IgM) | Negative | — |
| Anti-thyroglobulin | <12 | <12 |
| Anti–dsDNA antibody (IIF) | <1:10 | <1:10 |
| Anti–proteinase 3 antibody | <0.2 U/mL | <3 U/mL |
| Antineutrophil cytoplasmic antibodies | <1:20 | <1:20 |
| Antinuclear antibodies (IIF) | <1:80 | <1:80 |
| Extractable nuclear antigen (ENA) screen (dsDNA, SS-A/Ro, SS-B/La, Sm, RNP, Scl-70, centromere, Jo-1, fibrillarin, RNA Pol III, PM-Scl, PCNA, Mi-2, ribosomal P) (FEIA) | Negative | Negative |
| Rheumatoid factor | 4 UI/mL | <14 UI/mL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVector-borne infectious diseases · Viral Infections and Vectors · Thermal Regulation in Medicine
Introduction
Acute spinal cord injury (SCI) remains a life-threatening event, radically transforming mobility and sensation. Among the less frequently recognised complications of high cervical or upper thoracic SCI is a phenomenon known colloquially as quad fever - defined as an extreme, non-infectious hyperpyrexia (often exceeding 40.8 °C) occurring in individuals with quadriplegia or high paraplegia following SCI [1,2].
Despite heterogeneous definitions, uncertain etiology, and the limited number of reported cases, quad fever is consistently associated with a substantially increased mortality, with reported rates reaching up to 28.6% [1,3].
Unlike typical febrile responses driven by infection or inflammation, this central thermoregulatory failure appears to stem from autonomic dysfunction and impaired hypothalamic-spinal pathways, rendering traditional antipyretic strategies largely ineffective [1,4].
Although fever of any cause is frequent after SCI - reported in up to 60% of patients - the neurogenic or non-infectious subset remains under-recognised, with estimated incidences ranging from 2.6% to 27.8% [4,5].
What complicates management is that quad fever is often a diagnosis of exclusion [4]. Patients typically present with persistent high-grade fever, negative microbiological studies, and no identifiable infectious cause. Consequently, misdiagnosis is common, leading to unnecessary antibiotic use and delayed recognition of the true thermoregulatory dysfunction [6].
In light of these challenges, this article aims to present a detailed clinical case of quad fever following high cervical traumatic SCI, outlining diagnostic reasoning, therapeutic interventions, and outcomes.
Case presentation
A 72-year-old woman with no relevant past medical history was admitted to the emergency department after an accidental fall from approximately 2 m, resulting in head and neck trauma. On physical examination, her Glasgow Coma Scale (GCS) score was 15, and vital signs were within normal limits, with the patient afebrile. Cardiopulmonary auscultation was unremarkable. The initial neurological assessment revealed acute flaccid tetraparesis (Medical Research Council Muscle Scale 0/5) below the C4 motor level and C5 sensory level; deep tendon reflexes were absent, and plantar reflexes were bilaterally absent.
She underwent magnetic resonance imaging (MRI) of the head and neck, which revealed prevertebral hematomas at C2 and C5, likely related to injury of the anterior longitudinal ligament, as well as a linear fracture of the anteroinferior aspect of the C4 vertebral body with minimal adjacent bone edema. There was also evidence of a C6-C7 disc rupture and mild expansion of the spinal cord at C4-C5, consistent with spinal cord edema/contusion (Figure 1). A diagnosis of American Spinal Injury Association (ASIA) Impairment Scale grade A spinal cord injury was made, and she was transferred to a tertiary neurosurgical unit, where she underwent anterior cervical decompression and fusion at C4-C5 using a titanium plate and an iliac crest autograft. The procedure was uneventful.
Sagittal T2-weighted MR images of the cervical spine.(A) and (B) demonstrate a prevertebral hematoma anterior to the mid-cervical vertebral bodies, with maximal thickness measurements of 10.6 mm and 8.6 mm in different sagittal planes (arrows), and associated spinal cord edema/contusion (arrow tip) at the C4–C5 level.
Twelve hours postoperatively, she developed a fever of 40.9 °C, for which empirical broad-spectrum antibiotic therapy with piperacillin-tazobactam and vancomycin was initiated; however, the fever persisted. Antipyretic agents were ineffective, and the only interventions that produced partial defervescence were physical cooling measures, including ice packs and cold bladder irrigation. Due to ongoing daily fever spikes (Figure 2), an internal medicine consultation was requested.
Daily maximum temperature trend during hospitalization.Line graph showing the daily maximum recorded temperatures between September 11 and October 26, 2021. The patient initially presented with marked hyperpyrexia, with temperatures exceeding 40 °C, followed by a persistent pattern of high fever consistent with non-infectious fever after cervical spinal cord injury. Bromocriptine 5 mg twice daily was initiated on October 20, after which a progressive decline in temperature was observed, with resolution of fever in the days that followed.
During hospitalization, there was no evidence of cough, chest pain, dyspnoea, gastrointestinal or genitourinary symptoms, nor any history of recurrent fever, arthralgia, rash, xerostomia, xerophthalmia, oral ulcers, asthenia, anorexia, weight loss, or night sweats. She reported no relevant epidemiological exposures or recent drug use. On examination, she was haemodynamically stable, with no episodes of dysautonomia reported and no altered mental status (GCS 15). The remainder of the physical examination was unremarkable, including no lymphadenopathy, cutaneous rashes, mucosal enanthems, or clinical signs of arthritis.
Given the postoperative fever of undetermined origin, a stepwise diagnostic workup for infectious, inflammatory, and neoplastic causes was undertaken. Drug-related hyperthermia was ruled out.
Hematologic and inflammatory studies revealed a normocytic anemia on blood smear, with C-reactive protein, erythrocyte sedimentation rate, and procalcitonin remaining within normal limits. Peripheral blood immunophenotyping demonstrated a small lymphoid population without immunophenotypic abnormalities, providing no evidence of an underlying lymphoproliferative disorder.
Biochemical evaluation showed normal ACE, complement fractions (C3c and C4), creatine kinase, serum iron, transferrin saturation, triglycerides, vitamin B12, and β2-microglobulin. Immunoglobulin A, G, and M levels were also within the normal range, whereas immunoglobulin E was increased. Serum protein electrophoresis did not reveal any monoclonal component. Iron studies showed slightly elevated serum ferritin with reduced total iron-binding capacity (Table 1). Comprehensive microbiological evaluation of blood and urine, including fungal and mycobacterial studies, was also negative.
Extended serologic testing indicated past exposure to hepatitis A virus, cytomegalovirus, and Epstein-Barr virus. Human immunodeficiency virus (HIV) type 1 and type 2 (HIV-1 and HIV-2) antibodies were non-reactive. Tests for rickettsial diseases, typhoid fever, brucellosis (Widal, Wright, Rose Bengal), and toxoplasmosis immunoglobulin M (IgM) were negative. A peripheral blood zoonosis PCR panel (Anaplasma, Ehrlichia, Borrelia, Babesia, Coxiella, Rickettsia) was likewise negative. The interferon-gamma release assay for tuberculosis was negative. Autoimmune screening yielded negative results (Table 2).
Chest radiography and contrast-enhanced computed tomography (CT) of the chest were unremarkable, with no evidence of pulmonary embolism. Abdominal and pelvic CT revealed no abscesses or intra-abdominal foci. Transthoracic echocardiography showed normal valvular structures without vegetations. Duplex ultrasonography of the lower extremities excluded deep vein thrombosis. A lumbar puncture was performed, with no evidence of central nervous system infection.
Bone marrow aspirate and biopsy showed slightly hypocellular smears diluted with peripheral blood but no morphological abnormalities; Leishmania testing was negative. A comprehensive zoonosis panel (Anaplasma, Ehrlichia, Borrelia, Babesia, Coxiella, Rickettsia, tick-borne encephalitis virus) was negative, and bone marrow cultures were sterile. Flow cytometry revealed a small lymphoid population without immunophenotypic abnormalities suggestive of a lymphoproliferative disorder. The bone core was scant but demonstrated granulocytic hypoplasia without additional morphologic alterations.
Because of the elevated serum IgE, hypersensitivity to the titanium implant was considered. Standardised epicutaneous patch testing with a metals panel, including titanium, yielded negative results.
Repeat cervical MRI performed postoperatively demonstrated expected postoperative changes, without evidence of spondylodiscitis, epidural collection, or hardware complications (Figure 3). Fluorodeoxyglucose positron emission tomography (FDG-PET) demonstrated isolated homogeneous splenic hypermetabolism without splenomegaly, interpreted as reactive reticuloendothelial activity rather than occult malignancy.
Postoperative magnetic resonance imaging of the cervical spine.(A) Coronal T1-weighted image demonstrating expected postoperative changes following anterior cervical decompression and fusion, without evidence of epidural collection, spondylodiscitis, or hardware-related complications (arrow). (B) Sagittal STIR-weighted image showing hyperintense signal within the spinal cord at the C4–C5 level, consistent with spinal cord edema/contusion (arrow).
A diagnostic naproxen challenge did not produce defervescence, making neoplastic fever less likely. A five-day course of oral corticosteroids also failed to modify the temperature curve. Given the early postoperative onset, persistent fever despite antipyretics, and exclusion of infectious, inflammatory, and neoplastic causes, central fever secondary to cervical spinal cord injury was diagnosed. Bromocriptine 5 mg twice daily was initiated enterally, leading to defervescence within 24 hours and sustained apyrexia thereafter. No adverse effects were observed.
The patient was discharged in good general condition. She subsequently continued a structured physiatric rehabilitation programme appropriate for traumatic spinal cord injury. At follow-up, environmental temperature control, adequate hydration, and prevention of secondary complications were emphasised.
Discussion
Quad fever poses a diagnostic and therapeutic challenge in patients with high SCI. The present case illustrates how this rare form of neurogenic hyperpyrexia can emerge early after cervical trauma, mimic postoperative infection, and persist despite exhaustive investigation, antipyretic administration, empirical antimicrobial therapy, and physical cooling measures. In line with previous reports in which higher temperature elevations correlated with greater impairment on the ASIA scale, our case reflects this relationship precisely [1].
Recognition of this entity requires a high index of suspicion, particularly when fever remains refractory to standard interventions and no infectious, inflammatory, or neoplastic source is identified.
In our patient, the onset of hyperpyrexia within 12 hours post-surgery, coupled with the absence of local or systemic infection, normal inflammatory markers, and sterile microbiological cultures, pointed toward a central thermoregulatory origin. The extensive diagnostic workup - including serologic testing, bone marrow evaluation, advanced imaging, and exclusion of hypersensitivity reactions to titanium hardware - reflects the difficulty of confirming this diagnosis by exclusion alone. Such an approach is consistent with prior reports emphasising the need for systematic elimination of alternative etiologies before diagnosing quad fever [4,7,8].
Although the pathogenesis of quad fever has yet to be established, several hypotheses exist. Autonomic imbalance is a recognised consequence of cervical and high thoracic SCI, and disordered temperature control appears to fall within this spectrum, although the precise intermediary pathways are unclear [4]. The anterior hypothalamus serves as the central “thermostat” of the body, integrating input from thermal sensors and chemical mediators, such as cytokines and interleukins, and adjusting body temperature through vasomotor responses. When the central nervous system is damaged, disruption of the afferent and efferent connections between this region and the rest of the neuraxis may significantly impair this regulatory loop. One proposed explanation for the resulting episodes of severe hyperthermia is sympathetic dysregulation, leading to impaired vasodilation and an inability to sweat adequately at appropriate thermal setpoints [4,9].
Pharmacologic management of neurogenic hyperpyrexia remains largely empirical. Bromocriptine, a dopamine receptor agonist, was chosen in our case based on its potential to modulate hypothalamic dopaminergic activity and restore thermal balance. The rapid and sustained defervescence observed following initiation of bromocriptine supports previous observations describing its efficacy in this setting [9]. In contrast, antipyretics and corticosteroids failed to influence the temperature curve, consistent with reports indicating that central hyperthermia is unresponsive to conventional antipyretic mechanisms [2,10].
Environmental control, early recognition, and prompt initiation of targeted therapy appear to be key determinants of favourable outcomes [11]. Pharmacologic modulation, when effective, may reduce reliance on invasive strategies and improve patient comfort. Importantly, the benign postoperative appearance of the surgical site and the absence of systemic signs of infection should prompt clinicians to consider this diagnosis before escalating antibiotics unnecessarily.
The significance of early diagnosis extends beyond immediate fever control. Persistent hyperpyrexia in patients with SCI is associated with increased metabolic demand, cardiovascular instability, and secondary neuronal injury [6]. By avoiding these consequences, early recognition and appropriate treatment may improve neurological and functional recovery trajectories. Our patient’s initial stabilisation and clinical improvement after targeted therapy align with prior case reports describing favourable outcomes when quad fever is promptly identified and managed.
Nevertheless, several uncertainties remain. There are no standardised diagnostic criteria, and the true incidence of quad fever likely remains underestimated due to overlap with infectious fever syndromes. Prospective studies are needed to delineate risk factors, clarify underlying mechanisms, and establish evidence-based therapeutic protocols. Until then, clinician awareness remains the cornerstone of effective management.
Conclusions
Quad fever remains a challenging and unsettling diagnosis, both for clinicians and for patients already facing the life-changing impact of high cervical spinal cord injury. Our case illustrates how a sustained, unexplained fever can trigger an exhausting cascade of investigations, invasive procedures, and empirical treatments before a central thermoregulatory cause is considered. Recognising this entity early - particularly when inflammatory markers are normal, cultures remain sterile, and standard antipyretics are ineffective - can help avoid unnecessary antibiotic exposure, reduce iatrogenic harm, and refocus care on what the patient most needs: comfort, stability, and a clear explanation of what is happening to their body.
At the same time, this experience highlights a broader gap in our knowledge. There are no validated diagnostic criteria, and guidance on treatment is limited to small series and case reports. In our patient, bromocriptine provided a simple, well-tolerated, and remarkably effective therapeutic option, allowing her temperature to normalise and enabling meaningful participation in rehabilitation. Larger studies are needed to clarify the mechanisms, refine diagnostic pathways, and define evidence-based management strategies. Until then, maintaining a high index of suspicion, listening carefully to the patient’s narrative, and working in close multidisciplinary collaboration remain essential to improving outcomes for individuals living through this rare but serious complication of spinal cord injury.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Unraveling quad fever: severe hyperthermia after traumatic cervical spinal cord injury Chin J Traumatol Watson CC Shaikh D Di Giacomo JC 27322620233517728810.1016/j.cjtee.2022.01.006PMC 9912181 · doi ↗ · pubmed ↗
- 2Disorders of temperature regulation Compr Ther Lee-Chiong TL Jr Stitt JT 697704211995 https://europepmc.org/article/med/87891338789133 · pubmed ↗
- 3Fatal fever of unknown origin in acute cervical spinal cord injury: five cases J Spinal Cord Med Ulger F Dilek A Karakaya D Senel A Sarihasan B 3433483220091981063610.1080/10790268.2009.11760788 PMC 2718819 · doi ↗ · pubmed ↗
- 4Neurogenic fever after acute traumatic spinal cord injury: a qualitative systematic review Global Spine J Savage KE Oleson CV Schroeder GD Sidhu GS Vaccaro AR 607614620162755600210.1055/s-0035-1570751 PMC 4993608 · doi ↗ · pubmed ↗
- 5Fever during rehabilitation in patients with traumatic spinal cord injury: analysis of 392 cases from a national rehabilitation hospital in Turkey J Spinal Cord Med Unsal-Delialioglu S Kaya K Sahin-Onat S Kulakli F Culha C Ozel S 2432483320102073779710.1080/10790268.2010.11689701 PMC 2920117 · doi ↗ · pubmed ↗
- 6Non-infectious fever after acute spinal cord injury in the intensive care unit J Spinal Cord Med Ülger F Pehlivanlar Küçük M ÖztürkÇE Aksoyİ Küçük AO Murat N 3103174220192902749910.1080/10790268.2017.1387715 PMC 6522917 · doi ↗ · pubmed ↗
- 7QUAD fever: beware of non-infectious fever in high spinal cord injuries BMJ Case Rep Goyal J Jha R Bhatia P Mani RK 02017201710.1136/bcr-2017-219937 PMC 553490728630243 · doi ↗ · pubmed ↗
- 8Quad fever in a case of cervical cord injury—a rare case report Asian J Neurosurg Ali S Ganesan D Sundaramoorthy V 85871720223587385110.1055/s-0042-1748784 PMC 9298584 · doi ↗ · pubmed ↗