Isolated pectoralis minor tear at the costal origin: a case-based review of the literature
Nezih Ziroglu, Ali Can Koluman

TL;DR
This paper reports the first case of a pectoralis minor tear at the costal origin, expanding the known injury patterns and emphasizing the importance of MRI for accurate diagnosis.
Contribution
The paper presents the first documented case of a pectoralis minor tear at its costal origin, expanding the anatomical understanding of such injuries.
Findings
A 46-year-old male's MRI revealed a partial tear of the pectoralis minor at the costal origin, with associated rib bone marrow edema.
Eleven previously reported cases of isolated pectoralis minor tears occurred in athletes and involved different regions, not the costal origin.
Conservative treatment with analgesics and physiotherapy resolved symptoms in six weeks, supporting non-surgical management.
Abstract
Isolated tears of the pectoralis minor (PMi) are rare and often misdiagnosed as pectoralis major or costochondral injuries. Since the first report in 2004, only eleven cases have been described in the English-language literature, all involving the myotendinous junction or coracoid insertion. A tear at the costal origin has not previously been reported. A 46-year-old male developed acute anterior chest pain after pulling a heavy hospital bed. Physical examination revealed focal tenderness over the third to fifth ribs and pain with resisted internal rotation. Magnetic resonance imaging demonstrated a partial tear of the pectoralis minor at its costal origin with associated rib bone marrow edema, while the coracoid insertion and pectoralis major were intact. The patient was treated nonoperatively with analgesics and a structured physiotherapy program emphasizing scapular stabilization,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1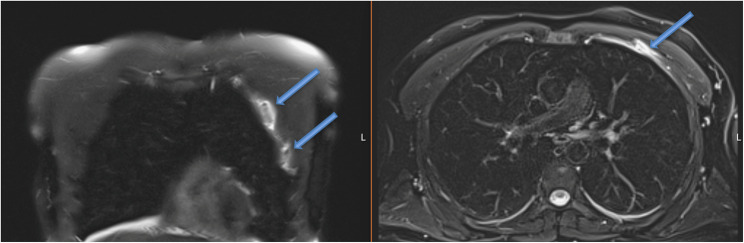 Figure 2
Figure 2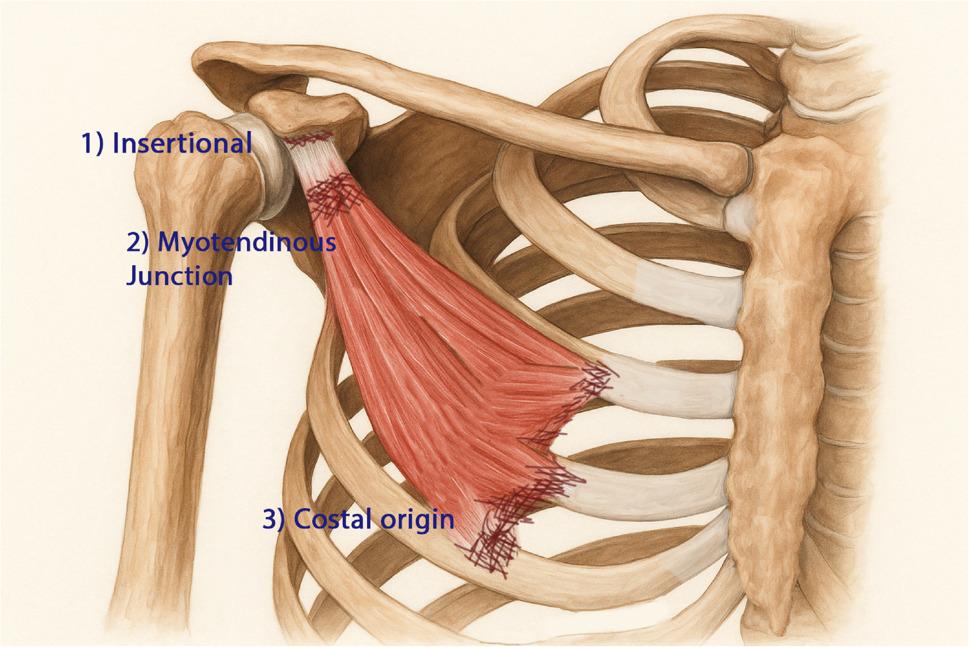 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder Injury and Treatment · Pectus Deformity Diagnosis and Treatment · Spine and Intervertebral Disc Pathology
Introduction
Tears of the pectoralis major are well recognized, particularly among athletes involved in contact or resistance-based sports. In contrast, isolated tears of the pectoralis minor (PMi) are rare and frequently overlooked because of the muscle’s deep location beneath the pectoralis major and its limited contribution to gross shoulder motion. As a result, PMi injuries are often misdiagnosed as pectoralis major strains, costochondral injuries, or nonspecific anterior chest wall pain [1–3].
The pectoralis minor originates from the third to fifth ribs near the costochondral junction and inserts onto the medial border of the coracoid process. Its primary function is scapular stabilization, drawing the scapula anteriorly and inferiorly along the thoracic wall, while it also assists rib elevation during deep inspiration [4, 5]. These biomechanical roles expose the muscle to eccentric traction forces, particularly during sudden scapular retraction or resisted upper extremity loading.
Since the first isolated PMi tear described by Mehallo in 2004 [3], eleven cases have been reported in the English-language literature [1–3, 6–11]. Most injuries occurred in contact or overhead athletes following direct impact or forced abduction–external rotation. Reported tear locations have been limited to the myotendinous junction or the coracoid insertion, and all patients were successfully treated nonoperatively, achieving full functional recovery within 2–12 weeks [1–3, 6–11].
Two narrative reviews published in 2019 by Vance et al. and Genel and Kieser further confirmed that all previously reported PMi tears were sports related and confined to the myotendinous or insertional regions [6, 11]. To date, a tear involving the costal origin of the pectoralis minor has not been described.
The present report describes the first documented costal origin tear of the pectoralis minor, associated with rib bone marrow edema following a low-energy, non-sporting mechanism, and provides an updated review of all reported cases.
Case presentation
A 46-year-old right-hand-dominant male school teacher, who regularly performed recreational pull-up exercises but was otherwise healthy, presented with acute-onset pain in the left anterior chest wall after attempting to pull a heavy hospital bed base. He described a sudden, sharp pain localized to the left pectoral region, without radiation, paresthesia, or an audible pop at the time of injury. The pain was predominantly activity related and was mildly exacerbated at the end of deep inspiration.
He denied any prior trauma, recent infection, corticosteroid use, or underlying systemic disease. There was no history of similar symptoms. Written informed consent was obtained from the patient for publication of this case report and the accompanying images.
Physical examination
Inspection revealed no visible ecchymosis, deformity, swelling, or contour asymmetry of the anterior chest wall. Palpation elicited marked focal tenderness over the third to fifth ribs near the costochondral junction and adjacent intercostal regions, while costovertebral angle tenderness was absent. Mild tenderness was noted over the coracoid process.
Active and passive shoulder range of motion was nearly full. Internal rotation produced mild discomfort, whereas external rotation was painless and symmetric. Strength testing demonstrated pain during resisted internal rotation and a painful lift-off maneuver without objective weakness; subsequent MRI confirmed an intact subscapularis tendon. Belly-press and bear-hug tests were pain-free, and the contour of the pectoralis major muscle was symmetric and intact.
Overall, the combination of focal costal tenderness, preserved pectoralis major contour, and pain provoked by deep, sub-pectoral maneuvers suggested a deeper anterior chest wall lesion consistent with pectoralis minor injury (Fig. 1).
Fig. 1. Clinical photographs of the anterior chest wall demonstrating preserved pectoralis major muscle contour without visible ecchymosis or deformity
Imaging studies
Magnetic resonance imaging (MRI) of the left shoulder demonstrated a partial tear of the pectoralis minor muscle at its costal origin, involving the third and fourth costochondral junctions. Associated bone marrow edema was present in the adjacent ribs, consistent with a traction-related injury mechanism. The coracoid insertion of the pectoralis minor and the pectoralis major muscle were intact.
Additional findings included mild subacromial impingement and low-grade signal changes of the long head of the biceps tendon, without evidence of rotator cuff tear or labral pathology (Fig. 2).
Fig. 2. Coronal STIR demonstrates adjacent rib edema. Axial PD-FS MRI shows a partial pectoralis minor tear at the costal origin (arrows) near the 3rd–4th costochondral junction
Management and outcome
The patient was managed nonoperatively with short-term oral analgesics and a structured, progressive physiotherapy program. Shoulder immobilization was intentionally avoided to minimize the risk of stiffness.
During the initial phase (weeks 0–2), activities provoking anterior chest wall pain were restricted. Overhead loading, resisted internal rotation, and forceful scapular retraction were avoided. Gentle, pain-free shoulder range-of-motion exercises were permitted, along with postural correction and breathing control exercises.
In the intermediate phase (weeks 2–4), active range-of-motion exercises were progressively advanced. Scapular stabilization exercises focusing on the serratus anterior and lower trapezius were initiated, while direct stretching or strengthening of the pectoralis minor was deferred until pain resolution.
During the final phase (weeks 4–6), gradual strengthening exercises and functional activities were introduced, including controlled scapular retraction and return-to-activity drills as tolerated.
At six weeks, the patient reported complete resolution of pain with full restoration of shoulder range of motion and strength, allowing return to work and recreational activities without limitation. At the three-month follow-up, he remained asymptomatic with symmetric strength and range of motion, and no evidence of recurrent pain or functional deficit.
Review of the literature
Literature search strategy
A structured literature search was conducted in the PubMed and Scopus databases (last search: October 6, 2025) using the following Boolean search strategy: (“pectoralis minor” AND (“tear” OR “rupture” OR “injury”)). Reference lists of all eligible articles were manually screened to identify additional relevant cases. Studies were included if they reported isolated pectoralis minor tears confirmed by magnetic resonance imaging or intraoperative findings. Reports describing combined pectoralis major injuries or nonspecific anterior chest wall conditions were excluded.
The search yielded 198 records, of which nine primary articles and two review articles met the inclusion criteria. Each review article contained one additional unique case, resulting in a total of eleven previously reported patients with isolated pectoralis minor tear published between 2004 and 2021 [6, 11].
Table 1. Summary of previously reported cases of isolated pectoralis minor tear (2004–2021) Data source: pubmed and scopus (search date: October 6,* 2025). Only isolated PMi tears with MRI confirmation included*YearAuthor (Ref)Age/SexMechanism of InjuryLevel of TearImaging FindingsManagementClinical Outcome2004Mehallo[12]40 / FDirect impact (football)MyotendinousMRI: edema, P.Major intactConservativePain-free at 2 wks2009Zvijac et al.[3]Late 20s / Pro football players (n = 2)Blocking / contactMyotendinousMRI-confirmed MTJ tearConservativeReturn 3–4 wks2010Kalra & Neri[2]25 / M/ Pro hockey playerCollisionInsertional (coracoid)Tendon retraction at coracoidConservativeFull in 4 wks2012Li et al.[1]17 / M/ HS footballTackle / FOOSHInsertionalPartial tear at coracoidConservativeRecovery by 12 wks2016Örücü et al.[8]HD patientSpontaneousMyotendinousLocalized edemaConservativeAsymptomatic2018Colazo et al.[10]24 / MMotor vehicle collisionInsertional (partial)Focal signal near coracoidConservativeFull recovery2018McNeilan et al.[9]27 / M/ NFL quarterbackFall on outstretched armMyotendinousMTJ edemaConservativeReturn 1 wk2019Vance et al.[11]24 / FNon-contact side-plankMyotendinousMTJ edemaConservativeFull in 6 wks2019Genel & Kieser[6]21 / MRugby tackleMyotendinousMRI: MTJ tear; P.Major intactConservativeReturned to play at 4 wks2021Loske et al.[7]30 / MOccupational overuseInsertionalTear + subclavian vein thrombosisConservative + anticoag.Mild venous sequelae2025Present case46 / MLow-energy pulling (non-sport) Costal origin tear Partial tear at 3rd–4th costochondral junction + rib marrow edemaConservativeFull in 6 wksZvijac et al. reported two athletes; total previously reported cases = 11. Including the present case, total = 12 [3]Across reported cases, most injuries occurred in young athletes during contact or eccentric-loading activities. Tear location predominantly involved the myotendinous junction [3, 8, 9, 11, 12] or the coracoid insertion [1, 2, 7, 10]. Diagnostic delay was frequently noted, likely related to the deep anatomical position of the pectoralis minor beneath the pectoralis major. In all cases, MRI was essential for confirming tear location and excluding concomitant pectoralis major injury [1–3, 6, 7, 9, 11, 12]. Management was uniformly nonoperative, with return to full activity or sport typically achieved within 2–12 weeks (Table 1). Vascular involvement was reported in a single case, presenting as subclavian vein thrombosis, which also responded to conservative management combined with anticoagulation therapy [7]
Position of the present case
Unlike previously reported cases limited to myotendinous or insertional involvement, the present patient exhibited a tear at the costal origin of the pectoralis minor, accompanied by adjacent rib bone marrow edema following a low-energy, non-sporting mechanism. This finding broadens the recognized anatomical spectrum of pectoralis minor tears and underscores the potential for diagnostic uncertainty when anterior chest wall pain is localized near the costochondral junction rather than the coracoid process.
Discussion
Isolated tears of the PMi represent an uncommon clinical entity and are frequently overshadowed by injuries of the pectoralis major or rotator cuff. Owing to its deep anatomical location beneath the pectoralis major and its close relationship to the coracoid process, clinical diagnosis is often challenging and delayed.
To date, eleven cases of isolated PMi tear have been reported in the English-language literature, all involving either the myotendinous junction or the coracoid insertion. The present report represents the twelfth documented case overall and the first involving the costal origin, thereby expanding the recognized anatomical and clinical spectrum of this rare injury.
Mechanism and anatomical considerations
The PMi functions as a dynamic stabilizer of the scapula, drawing it anteriorly and inferiorly during protraction and forward elevation [4, 5]. Sudden or excessive traction, particularly when the scapula is fixed against the thoracic wall, may generate eccentric loading across the muscle’s attachment sites.
In previously reported cases, such traction most commonly occurred during blocking, tackling, or forced abduction–external rotation in contact or overhead sports [1–3, 9–12]. The case described by Genel and Kieser [6], involving a rugby player with a myotendinous tear sustained during a tackle, exemplifies this high-load injury mechanism.
In contrast, the present patient sustained injury during a low-energy, non-sporting pulling maneuver while attempting to move a hospital bed. This observation suggests that even submaximal contraction may result in PMi injury when the rib cage is fixed and the scapula retracts abruptly, generating tensile overload at the costal origin. The tendon–bone interface near the costochondral junction may therefore represent a vulnerable site under such conditions. The presence of adjacent rib bone marrow edema on MRI further supports a traction-related injury mechanism at the proximal attachment.
From an anatomical perspective, PMi tears can now be categorized into three distinct levels:
- Insertional (coracoid process) – reported by Kalra [2], Li [1], and Loske [7];
- Myotendinous junction – reported by Mehallo [12], Zvijac [3], Örücü [8], McNeilan [9], Vance [11], and Genel & Kieser [6];
- Costal origin (costal attachment) – the current case (first documented).
This tripartite classification provides a more comprehensive framework for understanding injury patterns and mechanisms and may facilitate future reporting consistency (Figure 3).
Fig. 3. Schematic classification of isolated pectoralis minor tears
Diagnostic implications
Because the PMi lies deep to the pectoralis major, tears rarely produce visible deformity. Pain is typically localized to the anterior shoulder or upper chest and may be misattributed to costochondritis, pectoralis major strain, or intercostal pathology [2, 3, 12]. In the present case, maximal tenderness over the third to fifth ribs near the costochondral junction suggested a more inferior lesion than those reported previously.
Magnetic resonance imaging remains the diagnostic modality of choice, allowing precise localization of the tear and reliable exclusion of concomitant pectoralis major or rotator cuff pathology [1–3, 6]. Recognition of associated rib bone marrow edema, as observed in this case, may further raise suspicion for a costal origin injury. Although rare, clinicians should also remain alert to potential neurovascular complications, as subclavian vein thrombosis has been reported in association with PMi tear.
Ultrasonography may allow dynamic assessment of superficial soft tissue injuries and has been reported as useful in selected pectoralis major pathologies. However, evaluation of the pectoralis minor muscle is technically challenging due to its deep anatomical location beneath the pectoralis major and proximity to the thoracic wall, making sonographic visualization highly operator dependent. In contrast, magnetic resonance imaging provides superior soft tissue contrast and reliable delineation of tear location, extent, and associated findings, such as adjacent rib bone marrow edema, as demonstrated in the present case. For these reasons, MRI remains the preferred imaging modality for suspected isolated pectoralis minor tears.
Management and prognosis
Across all previously reported cases, management of isolated PMi tears has been uniformly nonoperative, consisting of rest, activity modification, physiotherapy, and gradual return to activity. Even professional athletes achieved full return to sport within weeks, and no patient required surgical intervention.
Although no standardized rehabilitation protocol has been established for isolated PMi tears, prior reports consistently describe conservative treatment with early pain-limited range of motion and progressive return to function. The phased rehabilitation approach used in the present case was intentionally conservative, emphasizing activity modification, avoidance of early resisted internal rotation or forceful scapular retraction, and delayed strengthening. This strategy aligns with the principles implicitly described in the existing literature while providing greater clinical detail to guide management.
The consistently favorable outcomes reported to date likely reflect the PMi’s secondary role in shoulder biomechanics, with limited contribution to power generation or joint stability [5]. The complete recovery observed in the present patient within six weeks further supports the effectiveness of conservative management across different tear locations.
Clinical relevance
This case broadens the recognized anatomical spectrum of PMi tears to include the costal origin and highlights that such injuries may arise from low-energy, non-sporting mechanisms. Clinicians should consider this diagnosis in patients presenting with anterior chest wall pain, preserved pectoralis major contour, and focal costal tenderness. Early MRI evaluation can confirm the diagnosis, prevent unnecessary investigations or interventions, and facilitate appropriate conservative rehabilitation.
Limitations
This report has several limitations. First, it describes a single patient, which limits the generalizability of the findings. Second, follow-up was limited to three months, and longer-term outcomes could not be assessed. Finally, although a detailed rehabilitation protocol is presented, no standardized rehabilitation guidelines exist for isolated pectoralis minor tears, and treatment strategies are largely based on limited case reports.
Conclusion
Isolated tear of the pectoralis minor is a rare and frequently underrecognized injury that may mimic pectoralis major or costochondral pathology. Including the present report, twelve cases have been described in the literature, all of which were successfully managed without surgical intervention.
The present case describes a costal origin tear of the pectoralis minor associated with adjacent rib bone marrow edema following a low-energy, non-sporting mechanism, thereby expanding the recognized anatomical spectrum of this injury. Accurate diagnosis with magnetic resonance imaging is essential to avoid misdiagnosis and to exclude concomitant pathology. Based on available evidence, conservative rehabilitation remains an effective treatment approach, with favorable functional outcomes reported across different tear locations.
Supplementary Information
Supplementary Material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.