Improving the management and outcomes of preschool wheeze: protocol of a prospective multicentre cohort study
Anne B Chang, Stephanie T Yerkovich, Steven McPhail, Hiran Selvadurai, Vikas Goyal, Shane George, Gabrielle B McCallum, Peter S Morris, Hannah O’farrell, Lesley Versteegh, Jonathan Grigg, Margaret McElrea, Sophie Worley, Terase Yerkovich, Leanne Elliot-Holmes, Joanna Williams

TL;DR
This study aims to improve asthma diagnosis in preschool children by using a digital device called WheezeScan to objectively detect wheezing and its response to treatment.
Contribution
The study introduces WheezeScan as a novel tool to objectively assess wheeze and its reversibility in preschool children, potentially improving asthma diagnosis and management.
Findings
Using WheezeScan may increase definitive asthma diagnoses in preschool children.
The study will assess if WheezeScan improves quality of life without increasing healthcare costs.
Abstract
Preschool wheeze and asthma are associated with substantial morbidity and impaired future lung function. Yet, wheeze is unreliably reported with high disagreement (>50%) between parental and physician observations. Objectively defining wheeze and its reversibility could enable an earlier asthma diagnosis and improve preschool wheeze management. Our primary aim is to determine in preschool children (aged 0.5–6 years) suspected of asthma whether adding WheezeScan to routine clinical assessment (vs assessment without WheezeScan) improves the diagnosis of asthma. Our primary hypothesis is that using WheezeScan in preschool children suspected of asthma is associated with increased definitive asthma diagnoses in this age group. Our secondary aims are to (a) examine the effect of using WheezeScan on patient-reported outcomes (PROs) and (b) healthcare costs. Our secondary hypothesis is that…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
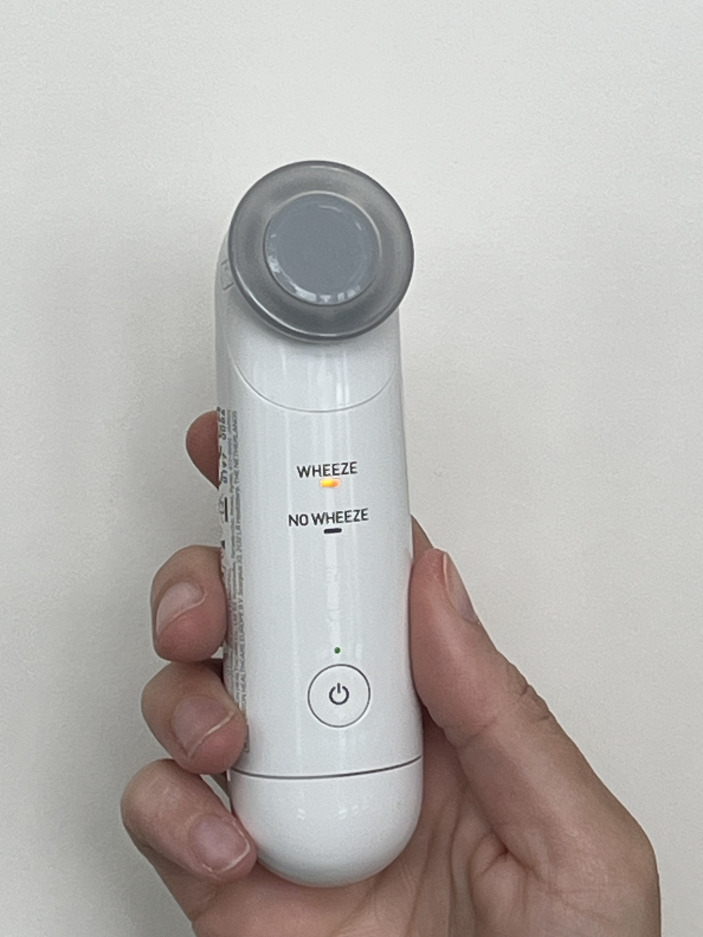 Figure 1
Figure 1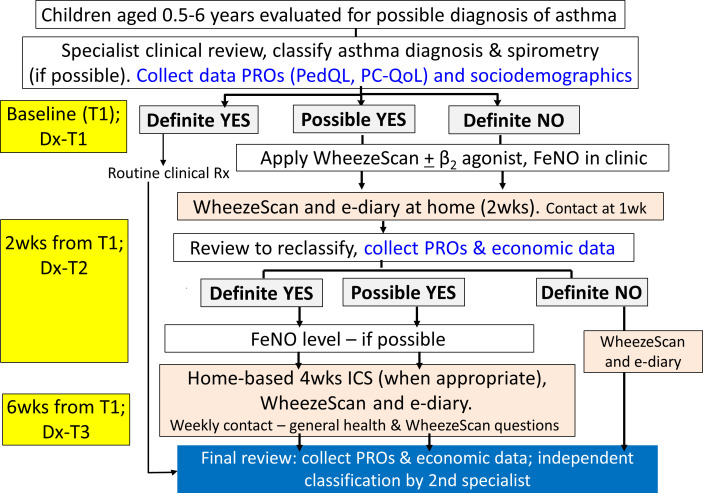 Figure 2
Figure 2| Assessment | Baseline (T1) | From baseline | |
|---|---|---|---|
| 2 weeks | 6 weeks | ||
| Window: | ±4 days | ±4 days | |
| Screening for eligibility | ✓ | ||
| Informed consent | ✓ | ||
| Sociodemographic and medical history | ✓ | ||
| Medical chart review | ✓ | ||
| Clinical assessment | ✓ | ✓ (optional) | ✓ (optional) |
| Classify asthma (yes/possible/no) | ✓ (primary specialist clinician) | ✓ (primary specialist clinician) | ✓ (primary and independent specialist clinicians) |
| PedsQL | ✓ | ✓ | ✓ |
| PC-QoL | ✓ | ✓ | ✓ |
| Health surveillance questions | ✓ | ✓ | |
| Spirometry (if aged >4 years); | ✓ | ✓ (if seen) | ✓ (if seen) |
| FeNO (if aged >4 years) once during study, if possible | ✓ | ✓ (if seen) | ✓ (if seen) |
| Analyse WheezeScan data | ✓ | ✓ | |
| Parent WheezeScan utilisation question | ✓ | ||
| NASSS-informed qualitative interviews | ✓ | or ✓ | |
| Collect results for full blood count, RAST, IgE (if available as part of clinical request) | ✓ | or ✓ | |
| Contact parent—general health and WheezeScan questions about any problems encountered | Every week between T1 and T3 | ||
- —http://dx.doi.org/10.13039/501100000925National Health and Medical Research Council
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAsthma and respiratory diseases · Delphi Technique in Research · Respiratory and Cough-Related Research
Introduction
Wheeze is a continuous, usually high-pitched, breath sound accompanied by a prolonged expiratory phase in the respiratory cycle. It originates from air turbulence in the lower airways due to partially obstructed intrathoracic airways causing flow limitation.1 Important aetiologies in young children are acute lower respiratory infections (including bronchiolitis), asthma, an inhaled foreign body and other lower airway disorders. Up to 50% of children have had an episode of wheeze by the time they reach school age, with 30–40% experiencing further wheezing episodes.2 Irrespective of the underlying wheezing pathobiology, wheeze symptoms cause substantial morbidity3 and economic cost.2 In the USA, preschoolers with recurrent wheeze have approximately two times the rate of outpatient physician and emergency department visits for wheeze exacerbations and more than five times the hospitalisation rate of older children with known persistent asthma.4 Furthermore, preschool wheeze is also associated with future impaired lung function trajectories, even when the wheeze is transient.5
When children are old enough to perform spirometry, many with a history of recurrent wheeze as preschoolers demonstrate a clear pattern of reversible airway obstruction (RAO) after receiving an inhaled short-acting β_2_-agonist (SABA) and/or inhaled corticosteroids, thereby suggesting they have underlying asthma.6 7 A systematic review and meta-analysis8 that included 19 studies (n=1022 children) concluded ‘inhaled SABA treatment for acute wheeze/asthma symptoms showed beneficial effects in young children and infants’. The meta-analysis found treatment with inhaled SABAs in preschoolers with wheeze decreased respiratory and wheeze scores, decreased respiratory rate and increased oxygen saturation.8 Within 60 min of administering SABA, the standardised mean difference between groups (all favouring those on SABA) was: decreased respiratory score (−2.05 points, 95% CI −2.50 to –1.59), decreased respiratory rate (−0.86, 95% CI −1.30 to –0.41), increased oxygen saturation (0.56, 95% CI 0.16 to 0.95), decreased respiratory work (−0.80, 95% CI −1.60 to –0.00) and decreased wheezing score (−1.07, 95% CI −1.80 to –0.33). In the subgroup analyses of children aged <2 years, the systematic review found similar significant effects for all outcomes.8 Thus, it is unsurprising that preschool children with recurrent wheeze and symptomatic improvement following SABA treatment will be diagnosed with asthma and, in some cases, their history of wheeze may date back to infancy.9 Under these circumstances, asthma therapies are generally used, although there is substantial variability between guidelines,3 probably due in part to the lack of evidence and problems with objectively defining wheeze.
Nevertheless, current guidelines for diagnosing asthma recommend objective confirmation with spirometry or peak flow,1012 although the exact criteria vary among guidelines. Effectively, the change in spirometry or peak flow represents objective documentation of RAO, the hallmark for diagnosing asthma. Lung function indices are rarely available for young children, and so in preschoolers, finding clinical evidence suggestive of RAO (ie, resolution of dyspnoea or wheeze with inhaled SABA)13 14 is often used as a surrogate measure. Nevertheless, this approach remains controversial as it requires accurate and objective detection of wheeze but often relies on parental detection and reporting.3
Despite the importance of detecting wheeze, there are high levels of disagreement (>50%) between parental and physician reporting of wheeze.15 This may cause underdiagnosis or overdiagnosis of asthma and lead to overuse or underuse of medications, children undergoing unnecessary procedures and high parental anxiety.16 17 Crucially, failing to recognise wheeze can delay diagnosis, especially if wheeze is recurrent, as it can defer appropriate treatment, which may lead to ongoing exacerbations, doctor visits, hospitalisations and an increased burden on parents/caregivers. In contrast, early recognition and treatment of asthma improves symptoms and quality of life (QoL).1012
While detecting wheeze and its reversibility with SABA is not the sole predictor in the diagnostic journey for asthma in preschool children, it is still a crucial step. Addressing the poor reliability of detecting wheeze in young children15 18 is a clear clinical gap. Recently, this gap was highlighted by the European Respiratory Society (ERS) Taskforce statement on preschool wheezing disorders.5 Its importance is even greater in settings where reporting of respiratory symptoms is more challenging, such as in disadvantaged First Nations communities19 and in settings where there are diverse cultures and languages spoken.18
Reliable and objective detection of wheeze using digital technology in clinics during face-to-face visits and at home when applied by parents could lead to improved diagnosis from detecting wheeze that responds to asthma treatments. There are now clinically validated tools that can objectively define wheeze. One such tool is the WheezeScan (figure 1, Omron Healthcare, Japan), which is the world’s first clinically validated device20 that uses artificial intelligence to detect and differentiate wheeze from other breath sounds in young children aged 4 months to 7 years.21 For our study, we chose WheezeScan as its design is user-friendly, ergonomic, light and portable, allowing parents to have it with them at all times and to remove any uncertainty when breathing distress occurs. In a pilot study from Germany involving 20 children, parents detected wheeze in 22/708 (3.1%) routine two times per day recordings, but WheezeScan indicated wheeze was present in 140/708 (19.8%) of the recordings.20
WheezeScan (Omron Healthcare, Japan). WheezeScan is the device we are using in our study. It is the world’s first clinically validated device20 that uses artificial intelligence to detect and differentiate wheeze from other breath sounds in young children aged 4 months to 7 years.
In addition to detecting wheeze accurately to allow an earlier and more objective diagnosis of asthma in preschool children,5 having patient-reported outcomes (PROs) as trial endpoints is important for adoption of effective best practice, which is also relevant to patients and their families. PROs include parent’s perception of their own and their child’s QoL, and in the case of WheezeScan with its ease of use. Disadvantaged Indigenous children and those with cultural and language barriers have a higher burden of respiratory illnesses than other children in the community22 and, for equity, studies should make every effort to include these children, irrespective of obstacles that may arise.
Therefore, with so many gaps5 in the understanding and management of preschool wheeze, both clinicians and parents are left confused over whether or not wheeze is present in young children, if it indicates underlying asthma and, if so, how it should be treated.16 Our study addresses several of these key clinical and end-user identified gaps.
Aims and hypotheses
Our primary aim is to determine in preschool children (aged 0.5–6 years) suspected of asthma whether adding WheezeScan to routine clinical assessment (vs assessment without WheezeScan) improves the diagnosis of asthma. Our primary hypothesis is that using WheezeScan in preschool children suspected of asthma is associated with increased definitive asthma diagnoses in this age group.
Our secondary aims are to examine the effect of using WheezeScan on: (a) PROs and (b) healthcare costs. Our secondary hypothesis is that using WheezeScan in preschool children suspected of asthma is associated with improved QoL without incurring additional healthcare costs.
Additionally, we aim to evaluate the perceived usefulness of WheezeScan for parents/caregivers using a qualitative evaluation.
Methods and analysis
Design
We are undertaking a prospective multicentre cohort study. Recruitment commenced from 1 February 2024 and is continiuing.
Study settings and participants
Study sites
Our study sites are the: Queensland Children’s Hospital (Brisbane, Queensland and including Indigenous outreach clinics in rural and remote Queensland), Gold Coast University Hospital (Gold Coast, Queensland), Children’s Hospital at Westmead (Sydney, New South Wales) and Royal Darwin Hospital (Darwin, Northern Territory), all in Australia.
Inclusion criteria
Children (aged 0.5–6 years) undergoing review by paediatric specialists for suspected asthma (≥2 reported wheeze episodes, chronic (>4 weeks) dry cough or exertional breathlessness) and have ongoing symptoms.
Exclusion criteria
Exclusion criteria are: (a) current chronic wet cough, (b) previous specialist-diagnosed asthma, (c) previously enrolled, (d) unable to complete PROs or (e) participating in another trial with an active intervention that may affect or bias findings.
Recruitment
Eligible children are identified from general paediatric and respiratory clinics and the emergency department at each study site. At each site, those fulfilling the inclusion criteria are invited to participate in the study and informed consent is sought before enrolment. On obtaining informed consent, baseline data are collected, and a specialist clinical review is performed. The study flow is presented in figure 2 and the outline of procedures is summarised in table 1.
Study flow of our cohort study. Dx, diagnosis; FeNO, fractional exhaled nitric oxide; ICS, inhaled corticosteroids; PC-QoL, Parent Cough-Specific Quality-of-Life29; PedQL, Paediatric Quality-of-Life Inventory V.428; PROs, patient reported outcomes; wks, weeks.
Study protocol
Data collection
Data are recorded by good clinical practice (GCP) trained researchers on case report forms as per our many trials.2327
At baseline (timepoint 1 (T1))
We are collecting study PROs (Paediatric Quality-of-Life Inventory V.4 (PedsQL)28 (in all children) and Parent Cough-Specific Quality-of-Life (PC-QoL)29 (if chronic cough present) questionnaires, as done previously23 and sociodemographic and clinical data (eg, age, sex, family/household size, personal and family history of atopy, ethnicity (eg, First Nations), medications used, tobacco or e-cigarette exposure and immunisation history) from the parents/caregivers, medical notes and the Australian Immunisation Register.
As per routine practice, children are assessed clinically by a paediatric specialist, most of whom are respiratory specialists. Those who are classified as ‘definite yes’ receive routine clinical treatment and are not seen again until timepoint 3 (T3). All children have the WheezeScan applied and if wheeze is present, the child is given 400 µg (four puffs) of inhaled SABA (using a spacer±mask), the standard dose to define presence/absence of a bronchodilator response.11 After 10 min, the WheezeScan is used again to determine whether wheeze is still present and the results recorded. Whenever possible, fractional exhaled nitric oxide (FeNO) is measured, but the clinician is blinded to the result.
A member of the research team then teaches the parents/caregivers of those classified as ‘possible’ and ‘definite no’ how to use the WheezeScan and the e-diary, both of which are to be used routinely two times per day for the next 2 weeks and when wheeze is suspected by the parents/caregivers (eg, postphysical activity). The parents/caregivers are asked to give 400 µg of inhaled SABA (using a spacer±mask) if wheeze is detected and to then reapply WheezeScan 10 min later to determine and record whether RAO is present. If wheeze is still present, the parents are asked to give a further 400 µg of inhaled SABA (as above), and then to reapply WheezeScan again 10 min later, and record whether RAO is present.
Follow-up (timepoint 2 (T2))
The data from the children monitored by the WheezeScan are reviewed 2 weeks after the baseline visit. WheezeScan and e-diary data are analysed and used for reclassification of the ‘asthma’ diagnosis (Dx-T2). The ‘definite yes’ and ‘possible’ groups following the second reclassification step then commence, when considered clinically appropriate, 4 weeks of inhaled corticosteroid (fluticasone 100 µg two times per day, using a spacer±mask). The ‘definite no’ group continues in the study using the WheezeScan and administering 400 µg of inhaled SABA (using a spacer±mask) if wheeze is detected and then reapplying the WheezeScan 10 min later to determine and record whether RAO is present. As above, the SABA and WheezeScan steps may be repeated once. Also, at T2, PROs are collected.
Final visit (timepoint 3 (T3))
6 weeks post-T1, the children are then again reclassified using WheezeScan data and response to inhaled corticosteroids, the latter if used following T2 (Dx-T3). Also, at T3, PROs and economic data from all study participants are collected.
At the end of the study, a second independent respiratory specialist reviews clinical data, including available FeNO results and WheezeScan data, from all participating children and based on this information classifies the asthma diagnosis in the child (labelled as the independent classification [i-]). The independent person is blinded to the treating clinician’s assessment.
In addition, parents/caregivers of those who used the WheezeScan are also asked to give feedback on the usefulness of the device, using a Likert scale question. The question, framed with advice from our consumer’s group, is as follows: ‘The WheezeScan is useful in managing my child’s wheezing problems?’ The Likert scale ranges from 1 (strongly disagree) to 5 (strongly agree).
Study exit criteria are: consent withdrawn or intolerance of SABA or inhaled corticosteroids (as determined by study site doctors or treating clinicians).
Outcomes and endpoints
Asthma classifications
- At T1, asthma classification is defined by the treating specialist clinician using clinical parameters.
- For other timepoints (T2 and T3).‘Definite yes’= presence of RAO defined by disappearance of wheeze using WheezeScan after 400 µg of inhaled SABA.‘Definite no’= no wheeze documented.‘Possible’=wheeze without clear response post-SABA or does not fit into the definite ‘yes’ or ‘no’ category.
- Independent classification by a second specialist after reviewing the data at T3.‘i-Asthma’= resolution of symptoms with treatment using WheezeScan data supported by FeNO >25ppb (if available).11‘i-no’= no effect of treatment.‘i-possible’= neither ‘yes’ nor ‘no’. Agreement between clinician and WheezeScan detection of wheeze at T1.PROs (PedsQL,28 PC-QoL29 (if chronic cough present)).Healthcare resource use and costs (healthcare system and family perspectives).Likert scale question relating to usefulness of WheezeScan at T3.See online supplemental file 1 for further description.
Endpoints
Primary
Proportion of children with a definite diagnosis (yes/no) of asthma from T3 to T1, based on the classification provided by the treating specialist clinician.
Secondary
Concordance of the asthma classification between the treating and independent specialist clinicians.Agreement between the clinical and WheezeScan detection of wheeze.Difference in PROs between the timepoints (T3−T1, T3−T2); subanalysed in accordance with whether inhaled corticosteroids were used.Composite measure of the ‘usefulness of WheezeScan’. We will consider WheezeScan clinically useful if: (a) WheezeScan assisted in a definite diagnosis (yes/no) or (b) PRO outcomes are superior in the WheezeScan-based versus independent asthma classification groups and (c) did not incur (net) healthcare costs during the study period.Healthcare resource use among the various classified groups (primary horizon at T3).
Data monitoring, management and analyses
Database management is based in Brisbane, as with our previous/current multicentre studies,232530 and is also GCP adherent. Study data are stored and managed using REDCap electronic capture tools hosted at the Queensland University of Technology server, with an additional layer of security provided by multifactor authentication. Missing data will not be imputed. A detailed statistical analysis plan will be developed prior to the analyses. This includes adjusting for potential biases (eg, age), if necessary.
Analyses
For the primary aim we will compare the proportions using McNemar’s test.
For the secondary aims:
Concordance of asthma classification (definite yes, definite no, possible) between the treating clinician and the independent specialist will be undertaken using weighted Kappa. Likewise, concordance between clinician and WheezeScan detected wheeze will be undertaken using Cohen’s Kappa.Change in PROs scores will be presented as means and SD and assessed by paired t-tests (assuming normal distribution) and the proportions with scores above the minimal clinically important difference (MCID) for each PRO in each group defined at T3 compared with T1.Composite measure of ‘usefulness of WheezeScan’ will be described and presented as numbers and percentages.Healthcare resource use associated with respiratory healthcare will be costed using actual costs (when known) or market rates from the perspectives of the healthcare system provider and families for each pathway (figure 2). Uncertainty estimates will be generated using bootstrap resampling (10 000 replications).
We anticipate reporting the last two secondary aims in a separate paper, as there will be a delay in the healthcare resource use analysis.
Sample size estimates
Our sample size is 102 children. This is based on conservative estimates of 15% being diagnosed with asthma at T1 and 30% at T3, with a correlation between the paired observations of 25%, which provides power>80% to detect a difference of 15% between the proportions. We will replace children with incomplete data and thus we expect to have complete data from 102 children. We conservatively estimate that 33% of children in our target group (preschool children with recurrent wheeze) have asthma (defined as RAO) and when adequately treated will be two times as likely to have significantly improved PRO above their MCID compared with when not treated due to wheeze misclassification known to be >50% in this age group.15
Discussion
Our study fulfils a large unmet clinical need and research gap identified by our parents and Parent Advisory Group, as well as by Australian31 and international surveys of clinicians and/or parents/caregivers.16 Our study is based on using a novel digital tool, WheezeScan, which objectively detects wheeze in children. Currently, physicians determine if wheeze is present based on either their own observations when the child is seen in clinic, or on parental reports. Both approaches are problematic. First, these scenarios rely on understanding wheeze and then detecting its presence. The ability to detect wheeze on auscultation is dependent on physician expertise, with respiratory physicians being the most accurate, while the error rate for other specialist physicians is as much as 30%.32 Second, a clinical assessment takes only minutes, which may not reflect the child’s state in the prior days and weeks. Third, many groups have shown the disconnect between parental understanding and detection of wheeze compared with that of physicians, with studies revealing >50% of parental wheeze reports are inaccurate.15 Furthermore, parents frequently misidentified other respiratory noises (eg, rattles or upper airway sounds) as wheeze,33 and some parents stated they were unable to hear or detect wheeze in their children.34 Thus, the need for objective confirmation of the presence or absence of wheeze is obvious, especially in scenarios which influence clinical decision-making and treatment.
Our diagnostic approach (presence of asthma based on wheeze-defined RAO) is informed by a large international survey undertaken by the European Academy of Allergy & Clinical Immunology.16 The survey identified ‘the most pressing problem with the diagnosis of wheezing in preschoolers is lack of diagnostic tools’.16 It also found that response to treatment was the most favoured method for making a diagnosis for preschool wheeze.16
The lack of diagnostic tools provides a common clinical challenge faced by clinicians managing recurrent wheeze in preschool children. Our project’s primary aim is to address this problem by objectively showing wheeze reversibility with SABA administration. As spirometry cannot be reliably obtained in most preschoolers, detecting wheeze reversibility clinically is used to represent RAO, the hallmark of asthma and where inhaled corticosteroids improve clinical outcomes (hospitalisations, recurrent episodes and symptoms).35
Potential study limitations
Potential limitations include the definition of RAO and its role in the classification of asthma. This is because defining RAO for the diagnosis of asthma in our target study population of preschoolers (aged 0.5–6 years) with recurrent wheeze is controversial and preschool wheeze is a heterogenous condition.5 Current ERS/American Thoracic Society (ATS) guideline criteria for defining bronchodilator responses (which indicates RAO) in adults rely on spirometry measured lung function indices where there is a >10% predicted increase in forced expiratory volume in one second (FEV_1_) or forced vital capacity, 15 min post administration of SABA.10 However, the ERS/ATS guideline does not specify the dose of SABA.10 Furthermore, guidelines in children differ; for example, the ERS clinical practice guideline for diagnosing asthma in children aged 5–16 years defines bronchodilator response as an increase in FEV_1_ of ≥12% and/or 200 mLs after a 400 µg dose of inhaled SABA.11 The 2024 Global Initiative for Asthma (GINA) guideline definition is a FEV_1_ increase of ≥12% post 200–400 µg of inhaled SABA (ie, volume change is not mentioned).12 Unfortunately, reliable spirometry is usually not possible in preschool-aged children and thus in our study, we are relying solely on objectively defined resolution of wheeze post-SABA to define RAO. Nevertheless, the definition of asthma used in our study’s target population (see inclusion and exclusion criteria) is consistent with the 2025 GINA guidelines as summarised by Venkatesan.36
Another limitation is our prospective cohort design rather than a randomised controlled trial (RCT). As such, our outcomes are at risk of bias. However, as far as we are aware, it is the first such study enabling a diagnosis of asthma based on objectively defined resolution of wheeze post-SABA and then for clinicians to initiate inhaled corticosteroids when clinically appropriate. Our design is therefore different to a recent RCT involving 167 children aged 4–48 months with a doctor diagnosis of wheezing in the preceding 12 months.37 This found no significant differences in their main outcomes (wheeze control and QoL) between the group who received the WheezeScan for at-home use for 120 days compared with ‘usual care’. However, the WheezeScan group had fewer unscheduled doctor visits (mean 1.6, SD 2.5) than the controls (mean 2.2, SD 3.3).37
Lastly, although the study duration was limited to 6 weeks, this timeframe should be sufficient to assess the primary outcome. Importantly, our study is not focused on children with established asthma. To determine the impact of using WheezeScan for asthma-specific outcomes requires a different study, which we are currently undertaking38 in parallel with this one.
Significance statement
Recurrent wheeze in preschoolers is associated with substantial morbidity3 and economic cost.2 Furthermore, their morbidity is greater than in older children with persistent asthma, as they have two times the rate of outpatient physician and emergency department visits for wheeze exacerbations and more than five times the hospitalisation rate.4 Moreover, preschool wheeze is also associated with future impaired lung function trajectories, even when the wheeze is transient.5 In this protocol paper, we describe our study that addresses the clinical problem of wheeze being unreliably detected in preschoolers and consequently the possibility of preschool asthma being under-diagnosed. By employing a user-friendly ergonomic device employing artificial intelligence to objectively detect wheeze and its response to SABA, our study has the potential to improve asthma diagnosis (from detecting wheeze that responds to asthma treatments) and QoL in preschoolers with recurrent wheeze.
Trial oversight
The study is monitored by the study sponsor, the Queensland University of Technology. We do not have an independent data safety and monitoring board.
Patient and public involvement
Our study is codesigned with parents of children with preschool wheeze and our Parent Advisory Group in Brisbane. It was also discussed with, and supported by, the First Nations Reference Group (Darwin) and a representative from the Asthma Foundation of the Northern Territory, the region in Australia with the highest proportion of Indigenous Australians. As suggested by these consumer groups, we included PROs as an outcome measure. Since there is no validated questionnaire specific to preschool wheeze, we are using two validated PROs, a generic health-related QoL (PedsQL)28 and in children with a chronic cough, the PC-QoL,29 as research tools, which we have used previously.23 39 Two parents and a representative from the Asthma Foundation of the Northern Territory are invited to all our investigator meetings (held every 4–8 weeks) and ‘parents voice’ is a standing item in all these meetings.
Dissemination
We will publish the results in a major medical journal and share the outcomes with the academic and medical community, funding and relevant patient organisations, including the Darwin First Nations Reference Group. Authorship eligibility guidelines will be used. We will not use professional writers. We currently do not have any plans to grant public access to the full protocol, participant-level dataset or statistical code.
Supplementary material
10.1136/bmjresp-2025-003606online supplemental file 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Meslier N Charbonneau G Racineux JL Wheezes Eur Respir J 199581942810.1183/09031936.95.081119428620967 · doi ↗ · pubmed ↗
- 2Fitzpatrick AM Bacharier LB Guilbert TW et al Phenotypes of Recurrent Wheezing in Preschool Children: Identification by Latent Class Analysis and Utility in Prediction of Future Exacerbation J Allergy Clin Immunol Pract 201979152410.1016/j.jaip.2018.09.01630267890 PMC 6401237 · doi ↗ · pubmed ↗
- 3Ruszczyński M Ambrożej D Adamiec A et al Preschool wheezing and asthma in children: A systematic review of guidelines and quality appraisal with the AGREE II instrument Pediatric Allergy Immunology 2021329210510.1111/pai.1333432816386 · doi ↗ · pubmed ↗
- 4Moorman JE Akinbami LJ Bailey CM et al National surveillance of asthma: United States, 2001-2010 Vital Health Stat 20123515824252609 · pubmed ↗
- 5Makrinioti H Fainardi V Bonnelykke K et al European Respiratory Society statement on preschool wheezing disorders: updated definitions, knowledge gaps and proposed future research directions Eur Respir J 202464240062410.1183/13993003.00624-202438843917 · doi ↗ · pubmed ↗
- 6Stokes JR Bacharier LB Prevention and treatment of recurrent viral-induced wheezing in the preschool child Annals of Allergy, Asthma & Immunology 20201251566210.1016/j.anai.2020.05.01832454096 · doi ↗ · pubmed ↗
- 7Fainardi V Santoro A Caffarelli C Preschool Wheezing: Trajectories and Long-Term Treatment Front Pediatr 2020824010.3389/fped.2020.0024032478019 PMC 7235303 · doi ↗ · pubmed ↗
- 8Storgaard Petersen R Hallas H Brustad N et al Short-term efficacy of inhaled short-acting beta-2-agonists for acute wheeze/asthma symptoms in preschool-aged children: a systematic review and meta-analysis Thorax 2025803495710.1136/thorax-2024-22276040122609 · doi ↗ · pubmed ↗