Impact of lotilaner ophthalmic solution 0.25% on disease severity in patients with Demodex blepharitis and meibomian gland disease
Bridgitte Shen Lee, Elizabeth Yeu, Kavita Dhamdhere, Eric D. Donnenfeld

TL;DR
Lotilaner eye drops significantly improved eye disease severity in patients with Demodex blepharitis and meibomian gland disease compared to a placebo.
Contribution
Demonstrated that lotilaner ophthalmic solution improves meibomian gland disease severity in patients with Demodex blepharitis.
Findings
47% of lotilaner-treated patients achieved mild or better disease severity at Day 43, compared to 21% with vehicle.
By Day 85, 63% of lotilaner-treated patients reached mild severity versus 24% with vehicle.
Lotilaner showed significant grade improvement over vehicle at both 6 and 12 weeks with no serious adverse events.
Abstract
To evaluate the impact of lotilaner ophthalmic solution, 0.25%, compared to vehicle, on disease severity in patients with Demodex blepharitis and meibomian gland disease. This post-hoc analysis pooled data from two prospective, randomized, double-masked studies evaluating lotilaner ophthalmic solution, 0.25% (Ersa, N = 39) and vehicle (Rhea, N = 40) in Demodex blepharitis patients with meibomian gland disease. The study utilized a modified International Workshop on Meibomian Gland Dysfunction (IWMGD) severity scale, integrating meibomian gland secretion score (MGSS) and patient-reported visual analog scale for fluctuating vision (VASFLVIS), and categorized meibomian gland disease severity as Grade 1 (subclinical), Grade 2 (mild), Grade 3 (moderate), or Grade 4 (severe). The main outcome was changes in severity grades from baseline. At baseline, meibomian gland disease severity was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
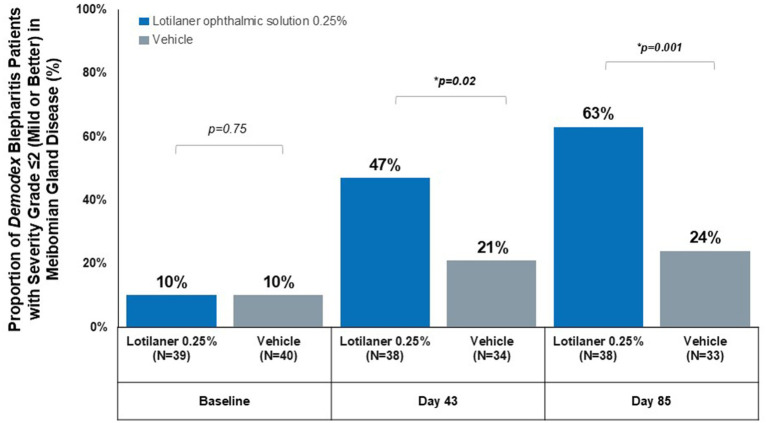 Figure 1
Figure 1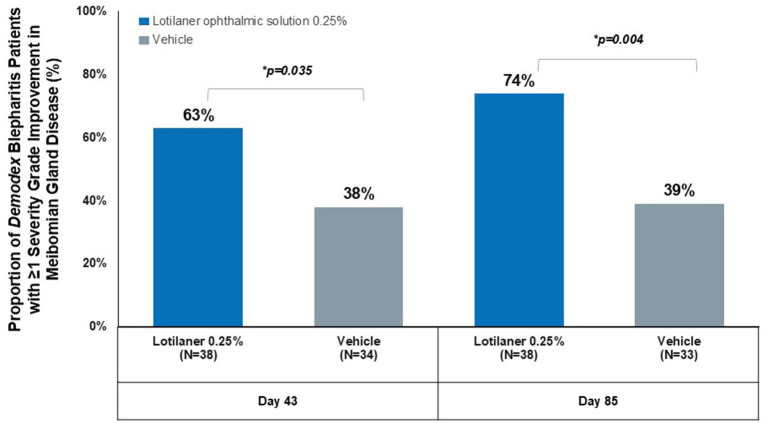 Figure 2
Figure 2| Severity grade | VASFLVIS criteria | MGSS criteria | Clinical interpretation |
|---|---|---|---|
| Grade 1 (subclinical) | <5 | >35 | Minimal to no symptoms and/or functional impairment |
| Grade 2 (mild) | ≥5 and ≤10 | ≥20 and ≤35 | Mild symptoms and/or mild functional impairment |
| Grade 3 (moderate) | >10 and <40 | >15 and <20 | Moderate symptoms and/or moderate functional impairment |
| Grade 4 (severe) | ≥40 | ≤15 | Severe symptoms and/or severe functional impairment |
| Characteristics | Lotilaner ophthalmic solution, 0.25% ( | Vehicle ( | |
|---|---|---|---|
| Age, years (mean ± SD) | 63.7 ± 14.7 | 63.4 ± 12.1 | 0.92 |
| Sex, | |||
| Female | 23 (59) | 23 (58) | 1.00 |
| Male | 16 (41) | 17 (43) | |
| Race, | |||
| White | 33 (84.6) | 34 (85.0) | 1.00 |
| African American/Black | 3 (7.7) | 3 (7.5) | |
| Asian | 3 (7.7) | 3 (7.5) | |
| MGSS (mean ± SD) | 21.9 ± 5.1 | 22.0 ± 4.8 | 0.93 |
| VASFLVIS (mean ± SD) | 46.5 ± 31.2 | 51.9 ± 30.5 | 0.4 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Surface and Contact Lens · Acne and Rosacea Treatments and Effects · Skin Protection and Aging
Introduction
Meibomian gland disease is a prevalent ocular surface disorder and the leading cause of evaporative dry eye disease (DED) (1). It affects as many as 70% of Americans over the age of 60 (2), and up to 40 million people in the United States (US) (3, 4). Meibomian gland disease is characterized by chronic, diffuse abnormalities of the meibomian glands in combination with alterations to lipid and protein components of glandular secretion that compromise tear film stability and ocular surface homeostasis (5, 6). The economic burden of meibomian gland disease and its associated DED approached $4 billion annually in 2011 in the US alone (4, 7). Further, meibomian gland disease and DED have significant impacts on quality of life and visual function (5, 8, 9).
The pathophysiology of meibomian gland disease is multifactorial. Some factors include glandular obstruction, bacterial colonization, inflammatory cascade activation, and parasitic infestations (10–12). Particularly, several recent studies have evaluated the role of parasitic infections from an epidemiologic standpoint. For example, Demodex infestations were reported in 57–89% of meibomian gland disease cases, as compared to 34–44% of controls without meibomian gland disease (10, 13, 14). Additionally, Luo et al. reported that symptomatic meibomian gland disease occurs in approximately 90% of patients with Demodex blepharitis, compared to 64% in dry eye patients without Demodex infestation (15). This bidirectional relationship suggests a pathogenic role for Demodex mites in meibomian gland disease. As the cause of meibomian gland disease is multifactorial, several different treatment modalities exist for its treatment. Currently, meibomian gland disease is managed through a diverse array of techniques like lid hygiene, lid scrubs, thermal pulsation systems with gland expression, light therapy, and microblepharoexfoliation, amongst many other modalities (16–18). However, these approaches neither treat Demodex blepharitis nor target mite infestation in the meibomian glands.
Lotilaner ophthalmic solution, 0.25% is the first and only FDA-approved drug for treating Demodex blepharitis (19). As a gamma-aminobutyric acid (GABA)-gated chloride channel inhibitor selective for mites, lotilaner 0.25% directly targets the root cause of Demodex infestation while demonstrating a favorable safety and tolerability profile (20). Previous clinical trials have established its efficacy in reducing collarettes, curing eyelid margin erythema, and achieving mite eradication (21, 22). The objective of this analysis was to apply a modified International Workshop on Meibomian Gland Dysfunction (IWMGD)-based severity grading scale to evaluate the changes in meibomian gland disease severity following treatment with lotilaner ophthalmic solution, 0.25%, compared to vehicle, in patients with Demodex blepharitis and concurrent meibomian gland disease.
Methods
Study design and population
The current study was a post-hoc analysis of a pooled study comprising two prospective, randomized, double-masked clinical trials: Ersa (NCT05454956) and Rhea (NCT06054217) that evaluated lotilaner ophthalmic solution, 0.25% and the corresponding vehicle formulation, respectively, in patients with Demodex blepharitis and meibomian gland disease. Ersa enrolled 39 patients across five US clinical sites from August 2022 to May 2023, while Rhea enrolled 40 patients across two US sites from August 2023 to March 2024. The two studies shared similar designs, eligibility criteria, and sample sizes, which allowed pooling once statistical equivalence was confirmed. All studies were conducted under institutional review board-approved protocols (Advarra IRB) and adhered to the Declaration of Helsinki. All participants provided written informed consent.
Eligibility criteria
Patients were required to meet all inclusion criteria in at least one eye: >10 upper lid lashes with collarettes, ≥1.0 mites/lash on epilated lashes from upper & lower eyelids combined, meibomian gland secretion score (MGSS) of 12–32 out of 45, Grade 1 or higher lower eyelid erythema, tear breakup time <10 seconds, ≥33% lower eyelid total gland area with intact partial to full meibomian glands on meibography, visual analog scale (VAS) score >40 for at least one patient-reported outcome (namely, fluctuating vision, itching, burning, or redness) one week prior to Day 1, and corrected distance visual acuity ≥0.7 logMAR on the Early Treatment of Diabetic Retinopathy Study (ETDRS) scale in each eye at Day 1.
Exclusion criteria included use of medications prior to Day 1 such as artificial tears (within 24 hours), antihistamines (within 30 days), cyclosporine/lifitegrast (within 60 days), any topical prostaglandin analog (within 6 months), isotretinoin (within 2 years), or other ocular/topical/systemic medications, drug delivery implants, corticosteroid, antibacterial, and/or antiparasitic treatment (within 14 days). Patients were excluded if they used any treatments for blepharitis within 14 days of Day 1, or any lid hygiene measures within 7 days of Day 1. Patients also had to be willing to forgo use of these measures for the study duration. Thermal pulsation treatments, intense pulsed light, meibomian gland probing, or therapeutic meibomian gland expression in either eye within 6 months were prohibited, as well as contact lens wear, artificial eyelashes, eyelash extensions and other cosmetic eyelashes or eyelid procedures within 7 days of enrollment. Patients with conditions or prior procedures that were deemed as confounding for study outcomes as per the opinion of the investigator were excluded, such as corneal transplant, a recent history of ocular surgery, eyelid abnormalities, ocular surface abnormality or disorder, punctal plugs, corneal disease, active ocular infection or inflammation other than blepharitis and meibomian gland disease, or systemic disease or medications known to cause dry eye. Patients with known hypersensitivities to lotilaner/any formulation components and pregnant/lactating patients were also excluded.
Treatment regimens
In the Ersa study, patients were randomized 1:1 to receive lotilaner ophthalmic solution, 0.25% either twice daily (n = 21) or three times daily (n = 18) for 12 weeks. In the Rhea study, patients were randomized to receive vehicle with varying regimens: twice daily (n = 12), three times daily (n = 11), or three times daily for 6 weeks followed by twice daily for 6 weeks (n = 17).
Assessments and severity scale
Meibomian gland assessment involved evaluation of 15 lower eyelid glands (5 consecutive glands in temporal, central, and nasal regions). Meibum quality was graded 0–3 (0 = no secretion, 1 = inspissated/toothpaste, 2 = cloudy, 3 = clear), with MGSS calculated as the sum of all 15 gland scores, yielding a score in the range of 0–45.
Patient-reported visual analog scale for fluctuating vision (VASFLVIS) was assessed using a 100-point numerical scale in which patients marked the point that best reflected their symptoms. The scale ranged from 0, indicating no discomfort, to 100, indicating maximal discomfort.
A modified IWMGD-based severity grading scale was developed by integrating both functional (MGSS) and symptomatic (VASFLVIS) parameters. The scale categorized meibomian gland disease severity into four grades: Grade 1 (subclinical): VASFLVIS <5 or MGSS >35; Grade 2 (mild): VASFLVIS ≥5 and ≤10 or MGSS ≥20 and ≤35; Grade 3 (moderate): VASFLVIS >10 and <40 or MGSS >15 and <20; and Grade 4 (severe): VASFLVIS ≥40 or MGSS ≤15 (Table 1).
Outcome measures
The present study measured the proportion of patients achieving meibomian gland disease severity Grade ≤2 (mild or better) and the proportion of patients demonstrating ≥1 grade improvement from baseline. Additional outcomes included changes in the individual components of the meibomian gland disease severity scale: MGSS and VASFLVIS.
Statistical analysis
Propensity scores were calculated using logistic regression with both baseline and disease characteristics as covariates (age, collarette score, eyelid erythema, MGSS, number of glands yielding any liquid secretion, number of glands yielding clear liquid secretion, and patient-reported outcomes) to confirm data interoperability. After confirming poolability, the intention-to-treat population included all randomized subjects, with the analysis eye defined as the eye meeting all inclusion criteria, or the eye with lowest baseline MGSS if both qualified. No significant differences were observed between different dosing regimens in either study, allowing combined analysis regardless of dosing frequency.
Continuous variables were analyzed using two-sample t-tests for between-group comparisons and paired t-tests for within-group changes from baseline. Categorical variables were assessed using chi-square tests. Statistical significance was set at p < 0.05.
Results
Baseline characteristics
A total of 39 patients participated in the Ersa (lotilaner-treated) study and 40 patients participated in the Rhea (vehicle-treated) study. One patient in the Ersa group was lost to follow-up due to investigator decision, and seven patients in the Rhea group were lost to follow-up due to a non-related adverse event (n = 1) and patient decision (n = 6). Mean age was 63.7 ± 14.7 years in the lotilaner group versus 63.4 ± 12.1 years in vehicle (p = 0.92). Baseline MGSS (21.9 ± 5.1 vs. 22.0 ± 4.8, p = 0.93) and VAS for fluctuating vision (46.5 ± 31.2 vs. 51.9 ± 30.5, p = 0.4) were comparable between groups (Table 2).
Meibomian gland disease severity outcomes
At baseline, meibomian gland disease severity distribution was identical between groups, with 10% of patients in each group classified as Grade ≤2 (mild or better) (p = 0.75).
By Day 43, 47% of lotilaner-treated patients achieved Grade ≤2 (Figure 1) compared to 21% of vehicle-treated patients (p = 0.02). The difference from baseline was even more apparent at Day 85, with 63% of lotilaner-treated patients achieving mild or better meibomian gland disease severity versus 24% in the vehicle group (p = 0.001).
Proportion of Demodex blepharitis patients with severity grade ≤2 (mild or better) in meibomian gland disease.
The proportion of patients demonstrating ≥1 grade improvement (Figure 2) was significantly higher at Day 43 (63% in lotilaner group vs. 38% in vehicle group, p = 0.035) and at Day 85 (74% vs. 39%, respectively; p = 0.004).
Proportion of Demodex blepharitis patients with ≥1 severity grade improvement in meibomian gland disease.
The lotilaner group demonstrated improvement from baseline in MGSS, improving by 26.9% at Day 43 (Δ + 5.7, p < 0.001) and 51.6% at Day 85 (Δ + 11.1, p < 0.001). Vehicle group changes were not statistically significant at either timepoint (p > 0.05). Between-group differences were statistically significant in favor of the lotilaner group at both Day 43 and Day 85 (both p < 0.001).
Lotilaner-treated patients also demonstrated statistically significant improvements from baseline in patient-reported fluctuating vision. Mean VASFLVIS in the lotilaner group improved by 52.3% at Day 43 (Δ − 22.9, p < 0.001) and by 71.8% at Day 85 (Δ − 32.0, p < 0.001). Vehicle group changes were lower at both timepoints: 22.7% at Day 43 (p = 0.010) and 40.7% at Day 85 (p < 0.001). Between-group comparisons were statistically significant in favor of the lotilaner group at Day 43 and Day 85 (both p < 0.01).
Safety profile
Ocular treatment-related adverse events occurred in 2 patients (5.1%) in the lotilaner group and in 7 patients (17.5%) in the vehicle group. In the lotilaner group, there was one case of conjunctivitis (2.6%) and one case of ocular discomfort (2.6%). In the vehicle group, ocular treatment-related adverse events included one case of conjunctival irritation (2.5%), one case of dry eye (2.5%), one case of eye irritation (2.5%), one case of instillation site irritation (2.5%), two cases of noninfective conjunctivitis by one patient (2.5%), one case of ocular hyperemia (2.5%), two cases of punctate keratitis (5.0%), and one case of reduced visual acuity (2.5%). No serious treatment-related adverse events were reported in either group.
Discussion
Demodex mites play a central role in the pathogenesis of meibomian gland disease through several mechanisms: mechanical blockage of gland orifices, consumption of epithelial cells and meibum, introduction of bacterial antigens, and activation of inflammatory pathways (10–12, 23). Reducing the mite burden can disrupt these processes and allow the glands to recover. The observed link between collarette grade, a marker of Demodex activity, and meibomian gland disease supports this mechanism (24). Treatments that directly target these mites, therefore, hold promise for improving meibum quality, gland function, and patient-reported outcomes.
This post-hoc analysis leverages a modified IWMGD-based severity grading scale to evaluate outcomes of lotilaner ophthalmic solution, 0.25% in patients with Demodex blepharitis and concomitant meibomian gland disease (9). The modified IWMGD-based severity grading scale incorporates both objective clinical signs and subjective patient-reported outcomes by integrating both gland function (MGSS) and patient-reported visual fluctuation (VASFLVIS). This dual-parameter approach acknowledges that meibomian gland disease severity may manifest predominantly through either functional impairment or symptomatic burden. We found that lotilaner ophthalmic solution, 0.25% not only improved individual parameters of gland function but also led to meaningful overall improvements: by 12 weeks, 74% of patients showed at least a one-grade reduction in meibomian gland disease severity.
The improvement in meibomian gland disease severity with lotilaner 0.25% over 12 weeks is an important finding. Benefits were clear at 6 weeks, and we observed an increase in magnitude at 12 weeks, suggesting that longer treatment may yield benefits. This is consistent with prior work showing that therapies such as thermal pulsation and intense pulsed light often require extended timeframes of ongoing treatment to achieve full effect in meibomian gland disease improvement (17, 25, 26). Eradicating Demodex mites may be an important initial step, with subsequent improvement of gland function observed after the underlying mite infestation is addressed.
The magnitude of improvement demonstrated in the lotilaner group was clinically meaningful: MGSS improved by over 50% after 12 weeks of treatment. Fluctuating vision, one of the most disabling symptoms of meibomian gland disease (27–29), improved over 70% at 12 weeks. The functional gain addresses one of the key drivers of evaporative dry eye and likely explains much of the symptom relief we observed (8, 9, 30). Safety findings were also favorable and were in line with prior literature (11, 19, 20). Overall, lotilaner ophthalmic solution, 0.25% was well-tolerated with no serious drug-related adverse events.
Limitations of this study include the small sample size and the relatively short study duration, which may not capture the full trajectory of improvement, as well as the post hoc pooled design. Prospective, independent studies evaluating a larger sample size may help validate the outcomes observed in this study. The study population included eyes that had at least 33% structural meibomian gland area intact and an MGSS between 12–32; the impact of more advanced gland atrophy or secretion dysfunction on recovery has yet to be determined. In addition, different dosing schedules were used in the studies. Despite this, our study possesses notable strengths including a randomized, double-masked design, consistent results across multiple outcomes, and the novel use of a clinically relevant grading scale.
In summary, lotilaner ophthalmic solution, 0.25% demonstrated statistically significant improvements in meibomian gland disease severity at 6 and 12 weeks in Demodex blepharitis patients with meibomian gland disease using a modified IWMGD-based severity grading scale. Lotilaner ophthalmic solution, 0.25% was well tolerated with a similar safety profile as the vehicle.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sheppard JD Nichols KK. Dry eye disease associated with Meibomian gland dysfunction: focus on tear film characteristics and the therapeutic landscape. Ophthalmol Ther. (2023) 12:1397–418. doi: 10.1007/s 40123-023-00669-1, 36856980 PMC 10164226 · doi ↗ · pubmed ↗
- 2Kim CK Carter S Kim C Shooshani T Mehta U Marshall K . Risk factors for Meibomian gland disease assessed by Meibography. Clin Ophthalmol. (2023) 17:3331–9. doi: 10.2147/OPTH.S 428468, 37937186 PMC 10627068 · doi ↗ · pubmed ↗
- 3Chester T Ferguson T Chester E. Localized heat treatment for meibomian gland dysfunction: a single-center retrospective analysis of efficacy over time. Optom Vis Sci. (2023) 100:625–30. doi: 10.1097/opx.0000000000002053, 37585853 PMC 10637300 · doi ↗ · pubmed ↗
- 4Mc Donald M Patel DA Keith MS Snedecor SJ. Economic and humanistic burden of dry eye disease in Europe, North America, and Asia: a systematic literature review. Ocul Surf. (2016) 14:144–67. doi: 10.1016/j.jtos.2015.11.002, 26733111 · doi ↗ · pubmed ↗
- 5Nichols KK. The international workshop on meibomian gland dysfunction: introduction. Invest Ophthalmol Vis Sci. (2011) 52:1917–21. doi: 10.1167/iovs.10-6997, 21450912 PMC 3072156 · doi ↗ · pubmed ↗
- 6Ou S Zhang L Wu Y Yang D Jiang N Mao T . Alterations in the composition of meibomian gland secretions in patients with meibomian gland dysfunction based on Raman spectroscopy. Front Med (Lausanne). (2025) 12:1717118. doi: 10.3389/fmed.2025.1717118, 41451082 PMC 12728007 · doi ↗ · pubmed ↗
- 7Yu J Asche CV Fairchild CJ. The economic burden of dry eye disease in the United States: a decision tree analysis. Cornea. (2011) 30:379–87. doi: 10.1097/ICO.0b 013e 3181 f 7f 363, 21045640 · doi ↗ · pubmed ↗
- 8Wei Z Liang J Cao K Wang L Baudouin C LabbéA . A multi-center study evaluating the correlation between meibomian gland dysfunction and depressive symptoms. Sci Rep. (2022) 12:443. doi: 10.1038/s 41598-021-04167-x, 35013413 PMC 8748897 · doi ↗ · pubmed ↗