Efficacy of cemiplimab and lenvatinib combination in metastatic cutaneous squamous cell carcinoma: A case report
Camille Decaestecker, Océane Babin De Lignac, Vivien Hébert, Raphaël Janela-Lapert

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
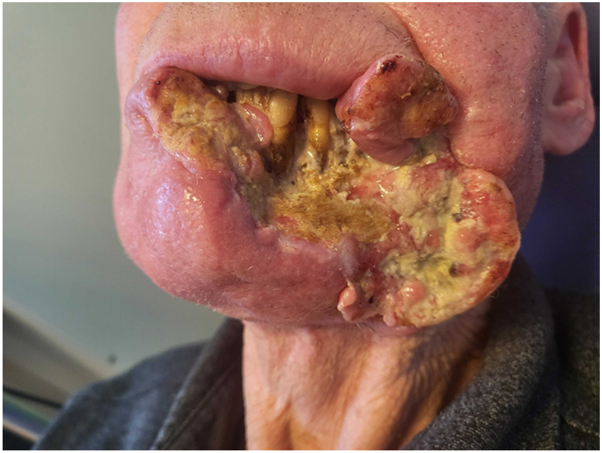 Figure 1
Figure 1 Figure 2
Figure 2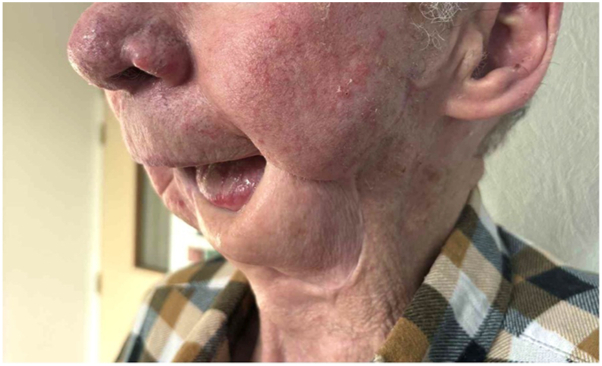 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNonmelanoma Skin Cancer Studies · Melanoma and MAPK Pathways · Cancer Diagnosis and Treatment
Introduction
Cutaneous squamous cell carcinoma (cSCC) accounts for approximately 20% of all skin cancers.1 Its prevalence and incidence are steadily increasing, primarily due to population aging and sun exposure habits. The risk of locoregional metastases (lymph node or in-transit), and more rarely distant metastases, is estimated at 2% to 5% at 5 years.2 First-line treatment of metastatic cSCC is based on anti-PD-1 immunotherapy (pembrolizumab or cemiplimab), with an efficacy rate of approximately 60%.3 Other therapeutic options include radiotherapy, chemotherapy (platinum-based agents), and EGFR inhibitors (cetuximab). The therapeutic efficacy of lenvatinib, a tyrosine kinase inhibitor in combination with anti-PD1-agents has been documented across several metastatic malignancies, including endometrial, renal, gastric, and melanoma cancers.4, 5, 6 Notably, the combination of pembrolizumab and lenvatinib had also demonstrated clinical benefit efficacy in head and neck squamous cell carcinoma.7 We report the case of metastatic cSCC resistant to conventional therapies that responded to the combination of cemiplimab and lenvatinib.
Case report
A patient in their 70s had been followed for 3 years for a cSCC of the lower lip, initially treated surgically with incomplete excision. Local and parotid recurrence developed, treated with radiotherapy and cetuximab. A grade III anaphylactic reaction occurring 60 minutes after initiation of the first cetuximab infusion at a dose of 800 mg, contraindicated further administration of the drug. Ongoing local and retromandibular lymph node progression led to the initiation of cemiplimab at a dose of 350 mg every 3 weeks. After 14 cycles, PET-CT imaging revealed disease progression, with increased hypermetabolic activity involving the skin and subcutaneous tissues of the lip, along with osseous invasion of the ipsilateral horizontal ramus of the mandible. Given the contraindication to further radiotherapy, related to prior irradiation complicate by osteoradionecrosis, and the impossibility of surgical management, monotherapy with carboplatin at a dose of 800 mg every 4 weeks was initiated. Treatment was discontinued after 5 cycles due to poor tolerance, marked by severe thrombocytopenia and cemiplimab was reintroduced. Because of the rapid progression of the initial lesion (Fig 1), lenvatinib 20 mg daily was added to cemiplimab. After 2 months of combination therapy, a complete response was observed, with full remission of the tumor and resolution of lymphadenopathy on PET-CT imaging. The response time supports the efficacy of the cemiplimab and lenvatinib combination in this patient. However, at 5 months, impaired healing with bone exposure prompted several biopsies, which revealed bone necrosis, granulation tissue and ulcerated epithelium, with no evidence of malignancy (Fig 2). Lenvatinib, known to impair wound healing, was discontinued. The osteoradionecrosis was managed with a segmental mandibulectomy and reconstruction of the orofacial defect using a pectoralis major myocutaneous flap. Histopathologic examination of the resected specimen revealed no evidence of recurrent or residual carcinoma (Fig 3). At 17 months following discontinuation, no recurrence was observed (Fig 4).Fig 1. Rapid and destructive local progression after 5 cycles of cemiplimab monotherapy.Fig 2. Complete oncologic response with osteoradionecrosis after 5 months of combined cemiplimab and lenvatinib therapy.Fig 3. Ongoing complete response on cemiplimab monotherapy, 17 months after lenvatinib discontinuation.Fig 4. Clinical and therapeutic history.
Discussion
The efficacy of anti-PD-1 agents in metastatic cSCC has been well established. However, therapeutic options remain limited in cases of treatment failure, often yielding poor long-term outcomes and unfavorable tolerability profiles. Lenvatinib is a tyrosine kinase inhibitor with anti-angiogenic properties, which may account for its potential to impair wound healing.8 The rationale for its use in combination therapy for refractory cSCC is based on the marked neovascularization frequently observed in this cancer type, particularly in patients with no remaining standard treatment options. To our knowledge, this is the first reported case of a metastatic cSCC achieving a complete response with the combination of lenvatinib and cemiplimab. This therapeutic approach may represent a promising option in the context of treatment-refractory cSCC. Although, caution is advised due to reported risks of impaired wound healing associated with lenvatinib, particularly in patients with cSCC who frequently undergo radiotherapy.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stratigos A.J.Garbe C.Dessinioti C.European interdisciplinary guideline on invasive squamous cell carcinoma of the skin: part 1. epidemiology, diagnostics and prevention Eur J Cancer 1282020608210.1016/j.ejca.2020.01.00732113941 · doi ↗ · pubmed ↗
- 2Iancu D.Fulga A.Vesa D.Metastatic patterns and treatment options for head and neck cutaneous squamous cell carcinoma (Review)Mol Clin Oncol 20620244010.3892/mco.2024.273938756868 PMC 11097132 · doi ↗ · pubmed ↗
- 3Fung T.Samlowski W.Meoz R.Effectiveness and toxicity of cemiplimab therapy for advanced cutaneous squamous cell skin cancer in a community oncology practice Cancers (Basel)175202582310.3390/cancers 1705082340075670 PMC 11899135 · doi ↗ · pubmed ↗
- 4Mo D.C.Luo P.H.Huang S.X.Wang H.L.Huang J.F.Safety and efficacy of pembrolizumab plus lenvatinib versus pembrolizumab and lenvatinib monotherapies in cancers: a systematic review Int Immunopharmacol 91202110728110.1016/j.intimp.2020.10728133338862 · doi ↗ · pubmed ↗
- 5Arance A.de la Cruz-Merino L.Petrella T.M.Phase II LEAP-004 study of lenvatinib plus pembrolizumab for melanoma with confirmed progression on a programmed cell death protein-1 or programmed death ligand 1 inhibitor given as monotherapy or in combination J Clin Oncol 4112023758510.1200/JCO.22.0022135867951 · doi ↗ · pubmed ↗
- 6Albiges L.Gurney H.Atduev V.Pembrolizumab plus lenvatinib as first-line therapy for advanced non-clear-cell renal cell carcinoma (KEYNOTE-B 61): a single-arm, multicentre, phase 2 trial Lancet Oncol 248202388189110.1016/S 1470-2045(23)00276-037451291 · doi ↗ · pubmed ↗
- 7Chen T.H.Chang P.M.H.Yang M.H.Combination of pembrolizumab and lenvatinib is a potential treatment option for heavily pretreated recurrent and metastatic head and neck cancer J Chin Med Assoc 844202136136710.1097/JCMA.000000000000049733496513 PMC 12966077 · doi ↗ · pubmed ↗
- 8Cheng C.Nayernama A.Christopher Jones S.Casey D.Waldron P.E.Wound healing complications with lenvatinib identified in a pharmacovigilance database J Oncol Pharm Pract 25820191817182210.1177/107815521881710930501381 · doi ↗ · pubmed ↗