Lumbar Pseudogout Mimicking Pyogenic Spondylitis in an Older Patient: A Diagnostic Pitfall in Emergency Care
Masaatsu Kuwahara, Hideaki Imanaka

TL;DR
An elderly patient's severe back pain was initially suspected to be an infection but was diagnosed as rare lumbar pseudogout after a biopsy revealed calcium crystals.
Contribution
This case emphasizes the importance of considering lumbar pseudogout as a differential diagnosis in older adults with acute spinal inflammation.
Findings
Lumbar pseudogout can mimic pyogenic spondylitis in older patients, leading to diagnostic challenges.
Definitive diagnosis of pseudogout requires identification of calcium pyrophosphate dihydrate crystals via biopsy or synovial fluid analysis.
Corticosteroid therapy was effective in treating the patient's lumbar pseudogout despite renal dysfunction.
Abstract
Lumbar pseudogout, or calcium pyrophosphate dihydrate deposition disease (CPPD), is an uncommon manifestation of a crystal-induced arthropathy that typically affects peripheral joints. Spinal involvement, particularly in the lumbar region, is rare and may closely mimic infectious conditions such as pyogenic spondylitis. An 85-year-old man was hospitalized for pneumococcal pneumonia and subsequently developed severe low back pain on day 7 of admission. Although his pneumonia improved with antimicrobial therapy, inflammatory markers remained elevated, raising suspicion of pyogenic spondylitis. Computed tomography and magnetic resonance imaging of the lumbar spine demonstrated compression fractures and inflammatory changes at the L2/3 intervertebral disc but were insufficient to establish a definitive diagnosis. A diagnostic intervertebral disc biopsy was therefore performed, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
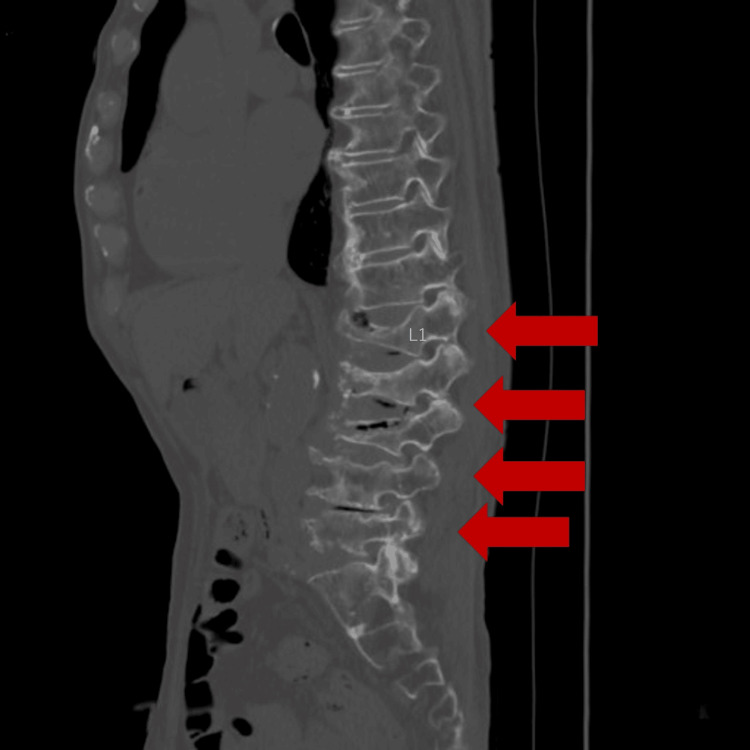 Figure 1
Figure 1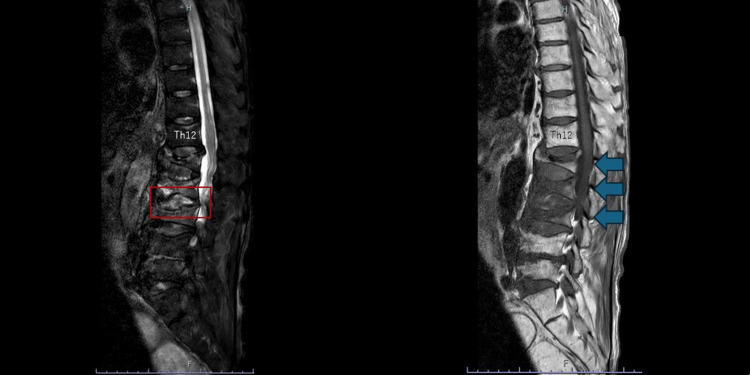 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGout, Hyperuricemia, Uric Acid · Dermatological and Skeletal Disorders · Spondyloarthritis Studies and Treatments
Introduction
Lumbar pseudogout, or calcium pyrophosphate dihydrate deposition disease (CPPD), is a crystal-induced arthropathy caused by the deposition of calcium pyrophosphate crystals in articular cartilage, fibrocartilage, ligaments, and other periarticular tissues. Since its first description in 1962, CPPD has been recognized as a common condition, particularly in older adults, and it most commonly affects peripheral joints such as the knees and wrists. In contrast, spinal involvement is uncommon; most reported cases involve the cervical spine, particularly in the form of crowned dens syndrome. Lumbar involvement is considerably rarer and remains underrecognized in clinical practice [1,2].
Lumbar CPPD predominantly affects older adults and presents with a wide range of symptoms, including acute low back pain, sciatica, fever, and neurologic deficits. Unlike gout, which is caused by monosodium urate crystal deposition and more commonly affects peripheral joints, CPPD-related spinal disease often lacks characteristic clinical features. It may closely mimic infectious or neoplastic conditions. Because clinical manifestations and imaging findings frequently resemble those of pyogenic spondylitis, metastatic spinal tumors, lumbar disc herniation, or spinal canal stenosis, establishing an accurate diagnosis is often challenging [3,4].
Although computed tomography (CT) and magnetic resonance imaging (MRI) may demonstrate calcifications or mass-like lesions within the intervertebral discs, facet joints, or ligamentum flavum, these findings are nonspecific, and differentiation from infectious or malignant etiologies remains difficult. Delayed or incorrect diagnosis may result in unnecessary antimicrobial therapy or invasive interventions; therefore, recognition of lumbar CPPD as a potential differential diagnosis is clinically significant, particularly in older patients presenting with acute inflammatory back pain.
This report describes a case of lumbar pseudogout in an 85-year-old man who developed severe low back pain during treatment for pneumococcal pneumonia.
Case presentation
Patient background and chief complaint
An 85-year-old man with a medical history of hypertension, left breast cancer (luminal A subtype without metastasis), currently treated with oral tamoxifen, and lumbar compression fractures was admitted to our hospital for treatment of pneumococcal pneumonia (A-DROP score, 2). Although his pneumonia improved with antimicrobial therapy, his low back pain gradually worsened during hospitalization.
Current medical history
On admission, the patient tested positive for pneumococcal antigen in urine and was diagnosed with pneumococcal pneumonia. Streptococcus pneumoniae was later identified on sputum culture. Treatment consisted of intravenous ceftriaxone (2 g/d) for seven days and oral azithromycin (250 mg/d) for three days. His respiratory status improved; however, on day 7 of hospitalization, his low back pain progressively worsened.
Differential diagnoses included pyogenic spondylitis, a new lumbar compression fracture, and metastatic breast cancer. Because blood tests showed elevated inflammatory markers, pyogenic spondylitis was considered the most likely diagnosis, and further evaluation was pursued.
Physical examination
Physical examination revealed localized tenderness over the midline lumbar region. Neurological examination of the lower extremities, including assessment of muscle strength, sensory function, deep tendon reflexes, and straight leg raising, revealed no focal neurologic deficits.
Laboratory and imaging findings
Laboratory testing demonstrated a white blood cell count of 12,610/µL (reference range, 3360-8800/µL) with a neutrophil fraction of 83.5%, indicating a left shift. The C-reactive protein level was 14.66 mg/dL. Blood cultures obtained at the time of exacerbation of low back pain were negative. A CT of the lumbar spine (Figure 1) and an MRI of the lumbar spine (Figure 2) were performed as part of the diagnostic evaluation.
Lumbar spine CTCompression fractures were identified from Th12 to L5 (arrows).CT: computed tomography
Lumbar spine MRI showing T2-weighted fat-suppressed images (left) and T1-weighted images (right)On T2-weighted fat-suppressed images, the L2/3 intervertebral disc demonstrates high signal intensity. On T1-weighted images, decreased signal intensity of the bone marrow from L1 to L3 is observed, consistent with acute compression fractures.MRI: magnetic resonance imaging
MRI demonstrated findings suggestive of acute compression fractures as well as inflammatory changes at the L2/3 intervertebral disc. Because pyogenic spondylitis could not be excluded based on these imaging findings, a diagnostic intervertebral disc biopsy was performed.
Treatment and clinical course
Given the elevated inflammatory markers and imaging findings, an open intervertebral disc biopsy was performed. Histopathological examination and microbiological cultures of the aspirated material showed no bacterial growth; however, calcium pyrophosphate dihydrate crystals were identified under polarized light microscopy following routine staining. These findings established the diagnosis of lumbar pseudogout.
Because Japan is considered an intermediate tuberculosis burden country, tuberculosis was included in the differential diagnosis; however, tuberculosis-specific interferon-γ release assays were negative, effectively excluding tuberculous arthritis.
Initial treatment consisted of oral nonsteroidal anti-inflammatory drugs (indomethacin, 200 mg/d for seven days). Although the patient’s pain showed a tendency toward improvement, continuation of NSAIDs was deemed unsafe because he subsequently developed renal dysfunction, with blood urea nitrogen increasing from 28.2 mg/dL (reference range, 8-20 mg/dL) to 45.2 mg/dL and serum creatinine rising from 1.82 mg/dL (reference range, 0.65-1.07 mg/dL) to 2.73 mg/dL. Therapy was therefore switched to intramuscular triamcinolone acetonide (40 mg, single dose), resulting in rapid improvement of symptoms.
Discussion
Diagnostic challenges
In this case, diagnostic complexity arose from the overlapping clinical presentations of lumbar pseudogout and pyogenic spondylitis. Both conditions may present with severe back pain and elevated inflammatory markers, making differentiation difficult. The patient’s recent history of pneumococcal pneumonia further complicated the clinical picture and initially supported suspicion of infectious spondylitis.
Role of imaging
CT and MRI each have distinct advantages and limitations in evaluating spinal disorders. CT is widely available and effective for assessing osseous structures, vertebral deformities, and calcifications. In contrast, MRI provides superior soft-tissue contrast and is essential for evaluating bone marrow edema and inflammatory changes.
In the present case, these modalities were complementary: CT contributed to the assessment of vertebral morphology and the exclusion of gross structural abnormalities, whereas MRI was required to evaluate disc involvement and to assess for acute fracture and metastatic disease. Nevertheless, even with combined imaging, differentiation between pyogenic spondylitis and crystal-induced inflammatory disease remained difficult, necessitating histopathological confirmation.
Importance of crystal identification
Previous literature indicates that although imaging modalities may suggest CPPD, definitive diagnosis generally relies on identification of calcium pyrophosphate dihydrate crystals under polarized light microscopy, most commonly in synovial fluid, which remains the diagnostic gold standard when clinical or imaging findings are inconclusive [5-8].
In the present case, synovial fluid analysis was not feasible because the lesion was confined to the intervertebral disc. Instead, a diagnostic intervertebral disc biopsy was performed, and polarized light microscopic examination of the biopsy specimen demonstrated calcium pyrophosphate dihydrate crystals, thereby establishing the diagnosis of lumbar pseudogout.
Treatment and prognosis
The primary treatments for pseudogout include nonsteroidal anti-inflammatory drugs and colchicine. In the present case, continuation of NSAIDs was not feasible because of renal dysfunction; however, the patient’s symptoms improved rapidly after initiation of systemic corticosteroid therapy. Although spontaneous improvement cannot be excluded in a single case, corticosteroids appeared to be clinically effective in this patient. Previous reports have described favorable responses to corticosteroid therapy in patients with severe pseudogout or in those for whom NSAIDs are contraindicated [9,10].
Conclusions
This case highlights the importance of considering lumbar pseudogout in older adults presenting with acute low back pain and elevated inflammatory markers, particularly when pyogenic spondylitis is suspected. Although imaging studies help exclude alternative diagnoses, the definitive diagnosis of CPPD relies on identification of calcium pyrophosphate crystals, most commonly via synovial fluid analysis. In the present case, the diagnosis was established by crystal identification in an intervertebral disc biopsy specimen. Awareness of this diagnostic principle may facilitate timely diagnosis and appropriate management of lumbar pseudogout.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lumbar extradural pseudogout mass manifesting as radiculopathy: a case report J Multidiscip Healthc Lo PC Yue CT Kung WM 159315981420213423444710.2147/JMDH.S 316738 PMC 8253935 · doi ↗ · pubmed ↗
- 2Trauma induced calcium pyrophosphate deposition disease of the lumbar spine Case Rep Rheumatol Greca I Ben Gabr J Perl A Bryant S Zaccarini D 321835020202020 https://doi.org/10.1155/2020/32183503209530610.1155/2020/3218350 PMC 7035534 · doi ↗ · pubmed ↗
- 3Calcium pyrophosphate dihydrate crystal deposition disease (pseudogout) of lumbar spine mimicking osteomyelitis-discitis with epidural phlegmon Am J Orthop (Belle Mead NJ) Mikhael MM Chioffe MA Shapiro GS 6467422013 https://pubmed.ncbi.nlm.nih.gov/24078961/24078961 · pubmed ↗
- 4Lumbar spinal involvement in calcium pyrophosphate dihydrate disease: a systematic literature review Int J Gen Med Ben Tekaya A Nacef L Bellil M 763976561520223622631010.2147/IJGM.S 360714 PMC 9550172 · doi ↗ · pubmed ↗
- 5European league against rheumatism recommendations for calcium pyrophosphate deposition. Part I: Terminology and diagnosis Ann Rheum Dis Zhang W Doherty M Bardin T 5635707020112121681710.1136/ard.2010.139105 · doi ↗ · pubmed ↗
- 6The value of synovial fluid assays in the diagnosis of joint disease: a literature survey Ann Rheum Dis Swan A Amer H Dieppe P 4934986120021200632010.1136/ard.61.6.493PMC 1754135 · doi ↗ · pubmed ↗
- 7Calcific tendinopathy of the rotator cuff: pathogenesis, diagnosis, and management J Am Acad Orthop Surg Uhthoff HK Loehr JW 183191519971079722010.5435/00124635-199707000-00001 · doi ↗ · pubmed ↗
- 8Accuracy of synovial fluid analysis compared to histology for the identification of calcium pyrophosphate crystals: an ancillary study of the OMERACT US Working Group - CPPD subgroup Reumatismo Sirotti S Gutierrez M Pineda C 1061107320213434221110.4081/reumatismo.2021.1403 · doi ↗ · pubmed ↗