Knowledge, Attitudes, and Practices Regarding Breast Cancer and Its Prevention Among Female Doctors at a Tertiary Care Hospital in Pakistan
Safina Tanveer, Faiza Gul, Asma Rasool Peerzada, Ayesha Johar, Nida Mumtaz, Naveedul Haq, Safwa Nayab, Muhammad Bilal Elahi, Nawal Qadus, Ikram Ullah

TL;DR
This study explores breast cancer knowledge and screening practices among female doctors in Pakistan, finding that while they have strong symptom recognition and positive attitudes, their screening practices are suboptimal.
Contribution
The study provides new insights into breast cancer awareness and screening behaviors specifically among female doctors in Khyber Pakhtunkhwa province, Pakistan.
Findings
Female doctors showed strong knowledge of breast cancer symptoms but limited understanding of risk factors and screening methods.
Despite positive attitudes toward screening, only a minority of participants adhered to recommended screening practices.
Busy schedules and lack of institutional screening programs were the most commonly reported barriers to screening.
Abstract
Background and objectives Breast cancer is the leading cause of cancer mortality among women, yet screening remains underutilized in low-resource settings. Despite the central role of physicians in patient counselling, early detection, and guideline implementation, most research in Pakistan about breast cancer awareness has focused on nurses, medical students, or the general population. Evidence specifically examining female doctors, particularly in Khyber Pakhtunkhwa province, remains sparse. This study assessed breast cancer knowledge, attitudes, and screening practices among female doctors at a tertiary hospital in Peshawar, examined associations between knowledge and screening behavior, and identified perceived barriers to screening. Methods A cross-sectional survey was conducted among 188 female doctors at Khyber Teaching Hospital, Peshawar, Pakistan, in October 2025. Data were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
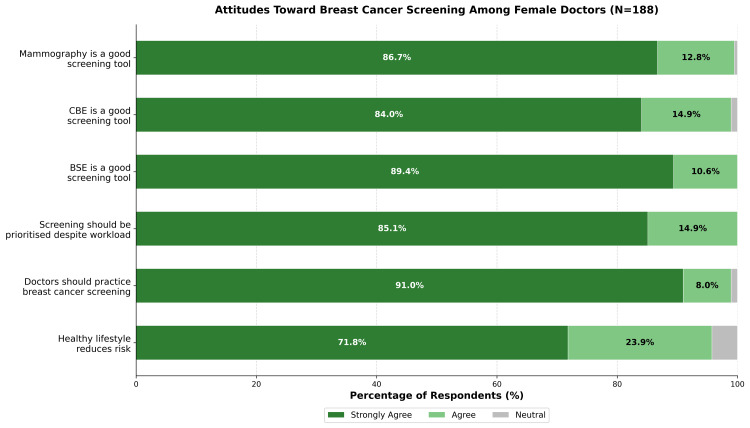 Figure 1
Figure 1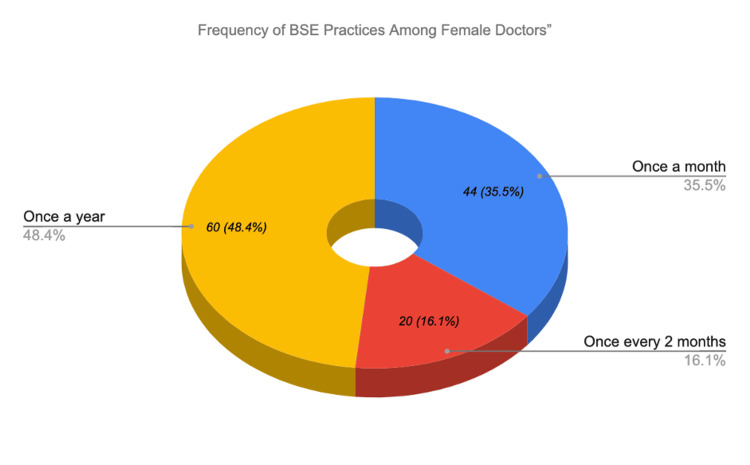 Figure 2
Figure 2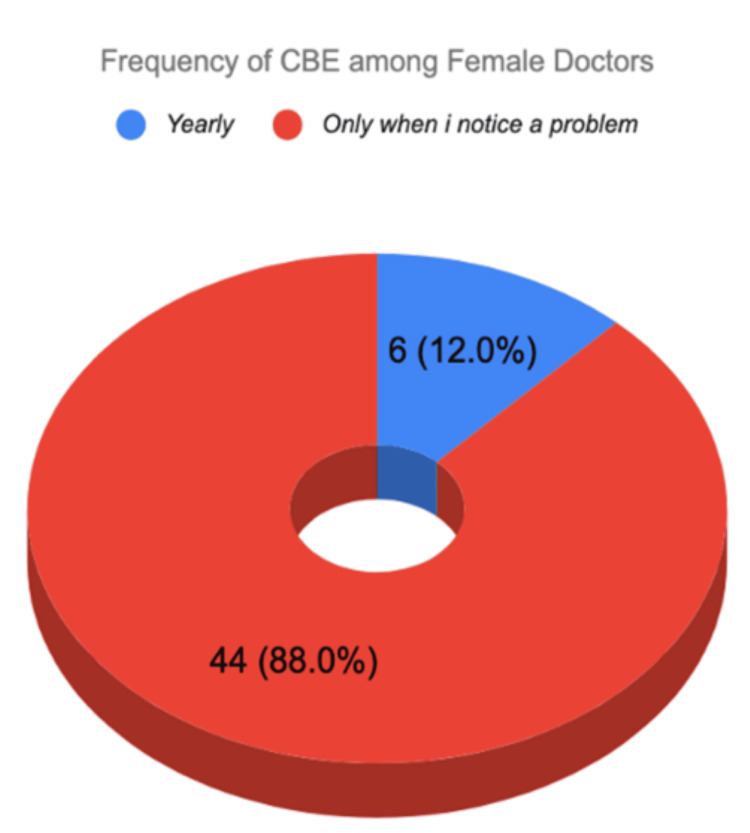 Figure 3
Figure 3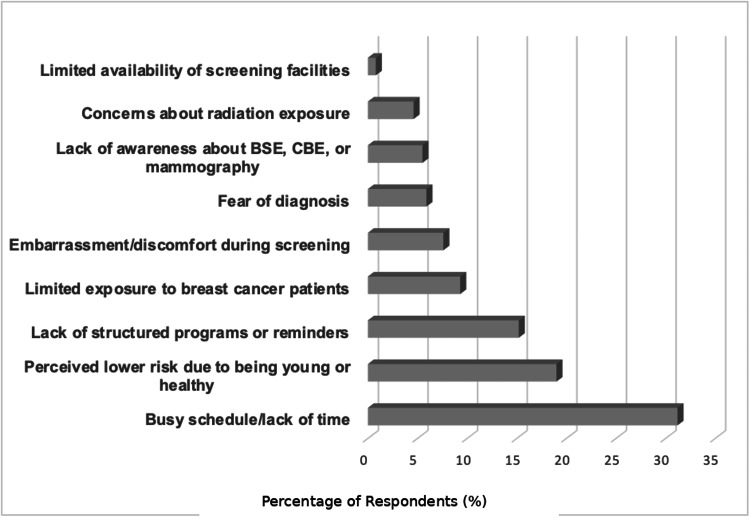 Figure 4
Figure 4| Characteristic | Category | N (%) |
| Age (years) | Mean ± SD (Range) | 27.47 ± 1.53 (24-33) |
| Designation | House officer | 31 (16.5%) |
| Postgraduate resident | 157 (83.5%) | |
| Department | Surgery | 66 (35.1%) |
| Medicine | 44 (23.4%) | |
| OBGYN | 31 (16.5%) | |
| Pediatrics | 14 (7.4%) | |
| Ophthalmology | 10 (5.3%) | |
| Radiology | 10 (5.3%) | |
| Dermatology | 6 (3.2%) | |
| Psychiatry | 4 (2.1%) | |
| Anesthesiology | 3 (1.6%) | |
| Marital status | Unmarried | 119 (63.3%) |
| Married | 67 (35.6%) | |
| Divorced/Widowed | 2 (1.1%) | |
| Family history | Yes | 49 (26.1%) |
| No | 139 (73.9%) | |
| First-degree relative* | 17 (9.0%) | |
| Second-degree relative* | 37 (19.7%) | |
| Registered with GP | Yes | 48 (25.5%) |
| No | 135 (71.8%) | |
| Prefer not to say | 5 (2.7%) |
| Knowledge Domain | Mean ± SD | Good N (%) | Fair N (%) | Poor N (%) |
| Risk factors (max: 10) | 5.67 ± 1.45 | 18 (9.6%) | 82 (43.6%) | 88 (46.8%) |
| Signs and symptoms (max: 5) | 4.76 ± 0.63 | 177 (94.1%) | 8 (4.3%) | 3 (1.6%) |
| Screening methods (max: 12) | 5.47 ± 1.92 | 4 (2.1%) | 85 (45.2%) | 99 (52.7%) |
| Total knowledge (max: 27) | 15.90 ± 2.73 | 6 (3.2%) | 154 (81.9%) | 28 (14.9%) |
| Knowledge Domain | Question | Correct Answer * | N (%) |
| Risk factors | Does having a history of breast cancer increase the risk of developing it again? | Yes | 183 (97.3%) |
| Does using Hormone Replacement Therapy increase the risk of breast cancer? | Yes | 148 (78.7%) | |
| Cigarette smoking increases the risk of breast cancer. | No | 164 (87.2%) | |
| Being overweight (BMI over 25) increases the risk of breast cancer? | Yes | 118 (62.8%) | |
| Does having dense breast tissue on a mammogram increase the risk of breast cancer? | Yes | 123 (65.4%) | |
| Having children later on in life or not at all increases the risk? | Yes | 135 (71.8%) | |
| Increasing age is a risk factor for breast cancer. | Yes | 149 (79.3%) | |
| Use of antiperspirants increases the risk of breast cancer. | No | 120 (63.8%) | |
| Disruptions in circadian rhythm (night shift work) increase the risk of breast cancer. | No | 112 (59.6%) | |
| <30 mins of moderate physical activity, 5 times a week, increases the risk of breast cancer. | Yes | 64 (34.0%) | |
| Signs and Symptoms | Nipple Discharge | Yes | 174 (92.6%) |
| Breast Skin Dimpling | Yes | 182 (96.8%) | |
| Pulling in of Nipple | Yes | 177 (94.1%) | |
| Change in the breast or nipple size and shape | Yes | 184 (97.9%) | |
| Lump in the breast or armpit | Yes | 184 (97.9%) | |
| Screening Methods | How many recognized screening methods are there for early detection of breast cancer? | 3 | 124 (66.0%) |
| The recognized screening methods? | BSE, CBE, Mammography | 18 (9.5%) | |
| At what age should women begin BSE? | 20 years | 107 (56.9%) | |
| How often should women perform BSE? | Monthly | 119 (63.3%) | |
| What is the best time to perform BSE? | 1 week after menstrual period | 88 (46.8%) | |
| At what age should women begin CBE? | 20 years | 86 (45.7%) | |
| How often should women perform CBE? | Yearly | 86 (45.7%) | |
| At what age should women with average risk begin mammography screening? | 40 years | 79 (42.0%) | |
| How often should mammography be performed by women? | Yearly | 112 (59.6%) |
| Practices | Response | N (%) |
| Do you actively monitor body weight? | Yes | 150 (79.8%) |
| No | 38 (20.2%) | |
| Do you engage in 30 mins of physical activity at least 5 times a week? | Always | 24 (12.8%) |
| Often | 51 (27.1%) | |
| Sometimes | 55 (29.2%) | |
| Rarely | 46 (24.3%) | |
| Never | 12 (6.3%) | |
| If you have children, did you or would you consider breastfeeding to reduce breast cancer risk? | Yes | 171 (91%) |
| No | 17 (9%) | |
| Do you practice BSE? | Yes | 120 (63.8%) |
| No | 68 (36.2%) | |
| Have you ever had CBE? | Yes | 50 (26.6%) |
| No | 138 (73.4%) | |
| Have you ever had mammography? | Yes | 5 (2.7%) |
| No | 164 (87%) | |
| Not applicable | 19 (10.1%) |
| Variables | 1 | 2 | 3 | 4 | 5 |
| 1. Risk factor knowledge | — | ||||
| 2. Signs/symptoms knowledge | 0.074 | — | |||
| 3. Screening knowledge | 0.018 | 0.217** | — | ||
| 4. Total attitude score | -0.004 | 0.016 | 0.067 | — | |
| 5. BSE frequency | -0.001 | -0.119 | -0.044 | 0.158* | — |
| Variable | BSE Yes (n=120) | BSE No (n=68) | U | p-value |
| Total knowledge | 15.95 ± 2.52 | 15.82 ± 3.10 | 4323.5 | 0.494 |
| Risk factor knowledge | 5.67 ± 1.44 | 5.66 ± 1.49 | 4174.5 | 0.789 |
| Screening knowledge | 5.56 ± 1.83 | 5.32 ± 2.07 | 4481.0 | 0.257 |
| Total attitude score | 29.01 ± 1.70 | 29.01 ± 1.77 | 4005.5 | 0.815 |
| Family History | No BSE n (%) | Yes BSE n (%) | Total |
| No family history | 58 (41.7%) | 81 (58.3%) | 139 |
| With family history | 10 (20.4%) | 39 (79.6%) | 49 |
| Barrier | BSE Yes (%) | BSE No (%) | χ² | p-value |
| Busy schedule | 69.2% | 75.0% | 0.465 | 0.496 |
| Perceived low risk | 42.5% | 39.7% | 0.048 | 0.826 |
| Lack of structured programs | 35.0% | 27.9% | 0.691 | 0.406 |
| Limited exposure to BCa | 16.7% | 19.1% | 0.051 | 0.822 |
| Embarrassment | 9.2% | 14.7% | 0.842 | 0.359 |
| Fear of diagnosis | 9.2% | 14.7% | 0.842 | 0.359 |
| Lack of awareness** | 5.8% | 19.1% | 6.720 | 0.010 |
| Radiation concerns | 5.0% | 11.8% | 1.984 | 0.159 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Cancer Incidence and Screening · BRCA gene mutations in cancer · Digital Radiography and Breast Imaging
Introduction
In 2020, breast cancer surpassed lung cancer to become the most commonly diagnosed malignancy worldwide and the leading cause of cancer mortality among women [1]. Although age-standardized incidence rates of breast cancer remain lower in Asia and Africa compared to Western nations, these regions account for nearly 72% of global breast cancer deaths [2]. This disparity reflects limited screening infrastructure, delayed diagnosis, and constrained treatment resources, resulting in substantially higher mortality-to-incidence ratios and late-stage presentation at diagnosis [3].
In Pakistan, one in four female cancer deaths is attributable to breast cancer, and between 1990 and 2019, incidence increased by over 300%, while mortality rose by 200%-300% [4]. Karachi, the country's largest metropolitan center, reports the highest breast cancer incidence in Asia [5]. These trends underscore the urgent need for enhanced awareness and early detection strategies.
Early detection significantly improves breast cancer survival. According to the American Cancer Society, established risk factors include increasing age, personal or family history, benign breast disease, dense breast tissue, early menarche, late menopause, hormone replacement therapy, obesity, and delayed or absent childbearing [6]. Common presenting symptoms include nipple discharge or bleeding, nipple inversion, changes in breast or nipple shape, skin dimpling, and any lump or thickening in the breast or axilla. Recognition of these risk factors and warning signs is fundamental to detecting disease at a treatable stage [7].
Three established screening modalities exist for early detection: breast self-examination (BSE), clinical breast examination (CBE), and mammography [8]. Mammography remains the gold standard, although its sensitivity is reduced in younger women due to breast tissue density [9]. The American Cancer Society recommends initiating screening at age 40, with annual mammography from age 45 [10]. However, disease patterns in Pakistan differ from those in the West; younger women are increasingly diagnosed despite having no identifiable risk factors [11]. This necessitates earlier screening, with annual mammography recommended from age 40 [11].
Despite the availability of effective screening methods, most Pakistani breast cancer patients present at advanced stages, primarily due to a lack of awareness and low socioeconomic status [12]. Pakistan allocates approximately 2.9% of its GDP to health, well below the global average of 7.2% [13,14], and screening facilities remain scarce: only 9.5% of urban and 4.8% of rural women utilize screening services, while radiological facilities are accessible to just 2.5% and 0.7%, respectively [8]. Where infrastructure for mammography is limited, awareness of risk factors, symptoms, and self-examination becomes critical. Given these constraints, improving breast cancer awareness represents the most feasible and cost-effective strategy for promoting early detection. However, beyond knowledge deficits, social and cultural barriers that delay help-seeking must also be addressed [12]. Identifying these gaps requires assessing Knowledge, Attitudes, and Practices (KAP), a framework endorsed by the World Health Organization for evaluating health awareness and behavior at the population level [15].
Despite the central role of physicians in patient counselling, early detection, and guideline implementation, studies assessing breast cancer knowledge and screening behavior in Pakistan have largely focused on nurses, medical students, or the general population. Evidence examining female doctors, particularly in Khyber Pakhtunkhwa province, remains sparse. This study aimed to (1) assess breast cancer knowledge across domains of risk factors, signs and symptoms, and screening methods; (2) evaluate attitudes toward breast cancer prevention and screening; (3) determine the prevalence and patterns of screening practices including BSE, CBE, and mammography; (4) examine the relationship between knowledge, attitudes, and screening behavior; and (5) identify perceived barriers to screening among female doctors at a tertiary care hospital in Peshawar, Pakistan.
Materials and methods
A descriptive cross-sectional survey was conducted in October 2025 among female doctors to evaluate their understanding of breast cancer. The study received approval from the Institutional Research and Ethical Review Board of Khyber Medical College, Peshawar, Pakistan (Approval No. 936/DME/KMC, dated: 06-10-2025). The target population consisted of registered female doctors working in various departments of Khyber Teaching Hospital, Peshawar. Sample size was calculated using the OpenEpi (Centers for Disease Control and Prevention (CDC) and Rollins School of Public Health, Emory University, Atlanta, Georgia, USA) sample size calculator for proportions, assuming a 95% confidence level, 5% margin of error, and a conservative estimate of 50% prevalence of adequate knowledge to maximize sample size. After inflating by 10% to account for non-response, the final required sample size was 223 participants.
Inclusion criteria comprised female doctors aged 25-55 years, working in the hospital, and willing to participate. Exclusion criteria included female paramedical staff, incomplete responses, and those who did not provide consent. A total of 188 completed responses were received within the designated data collection period, yielding a response rate of 84.3%. The remaining participants did not return the questionnaire within the stipulated timeframe and were excluded from analysis. Participants were recruited through non-probability convenience sampling. Female doctors were contacted via institutional email and WhatsApp (WhatsApp Messenger, Meta Platforms, Inc. (formerly Facebook, Inc.), Menlo Park, California, USA) and informed about the study objectives. Participation was voluntary, and electronic informed consent was obtained before commencing the survey.
The authors developed a structured, self-administered questionnaire after reviewing established literature on breast cancer risk factors, symptoms, screening recommendations, preventive behaviors, and barriers to screening. The questionnaire was pretested among 10 female doctors for clarity and comprehension, and minor modifications were made based on their feedback before data collection (Appendix A). A brief introduction and consent statement were provided at the beginning of the questionnaire, ensuring participants' confidentiality and voluntary participation. The instrument was divided into five sections: (1) demographic information, (2) knowledge assessment, (3) attitudes toward breast cancer prevention, (4) screening practices, and (5) perceived barriers to screening.
Section two assessed knowledge through 27 items across three domains: risk factors (10 items), signs and symptoms (five items), and screening methods (12 items). Each correct response scored 1 point; incorrect or don't know responses scored 0. A total score of <50% was categorized as poor knowledge, 50%-75% as fair knowledge, and >75% as good knowledge. Correct responses for knowledge items were determined based on established guidelines appropriate for the study context. Risk factor items were scored according to the American Cancer Society classification of breast cancer risk factors [6], which categorizes potential risk factors into four tiers: non-modifiable established factors, lifestyle-related established factors, factors with unclear effects, and disproven factors. Only factors classified within the first two tiers were scored as 'Yes' and regarded as established risk factors. For example, 'Cigarette smoking increases the risk of breast cancer' was scored as 'No' because the American Cancer Society (ACS) lists smoking under 'Factors with Unclear Effects.' Signs and symptoms items were based on the National Breast Cancer Foundation (NBCF) [7]. Screening method items were scored according to Pakistan's National Action Plan for Prevention and Control of Non-Communicable Diseases and Health Promotion (NAP-NCD) [8], which recommends breast self-examination, clinical breast examination, and mammography as appropriate screening modalities for early detection of breast cancer in Pakistan.
Section three assessed attitudes toward breast cancer prevention using six items rated on a five-point Likert scale (1=strongly agree to 5=strongly disagree). Responses were reverse-coded so that higher scores indicate more positive attitudes and summed to yield a total attitude score (range: 6-30). Section four assessed screening practices, including BSE (yes/no; if yes: frequency), CBE (yes/no; if yes: routine vs. symptomatic), mammography (yes/no), body weight monitoring, and physical activity levels. Section five assessed perceived barriers through a predefined checklist of 11 items. Respondents could select all applicable barriers. Each item was coded as a binary variable for analysis.
Statistical analysis
All responses were automatically compiled via Google Forms (Google LLC, Mountain View, California, USA) and analyzed using IBM SPSS Statistics version 31 (IBM, Armonk, New York, USA). Descriptive statistics, including frequencies and percentages, were used to summarize categorical variables, while means and standard deviations were calculated for continuous variables. Spearman's rank correlation coefficients were computed to examine relationships between knowledge, attitudes, and practices. Chi-square tests were performed to assess associations between categorical variables. Mann-Whitney U tests were used to compare knowledge and attitude scores between groups. All tests were two-tailed, and p<0.05 was considered statistically significant.
Results
A total of 188 female doctors participated in the study, with a mean age of 27.47 ± 1.53 years (range: 24-33 years). The majority were postgraduate residents (n=157; 83.5%), while 31 (16.5%) were house officers. Participants represented a broad range of specialties. Out of 188, 119 (63.3%) participants were unmarried, 67 (35.6%) were married, and one participant each (0.5%) was divorced and widowed. Regarding family history, 49 participants (26.1%) reported a family history of breast cancer: 17 (9.0%) in a first-degree relative and 37 (19.7%) in a second-degree relative, with five reporting both. The majority (n=139; 73.9%) had no family history. Table 1 presents the detailed demographic characteristics.
Knowledge assessment
Knowledge levels varied across the three assessed domains. The mean total knowledge score was 15.90 ± 2.73 out of a maximum of 27 points (58.9%). Knowledge of signs and symptoms was high, with a mean score of 4.76 ± 0.63 out of 5, and 177 out of 188 (94.1%) participants demonstrated good knowledge in this domain. Knowledge of screening methods was lower, with a mean score of 5.47 ± 1.92 out of 12; only four of 188 (2.1%) achieved good knowledge, while 99 of 188 (52.7%) demonstrated poor knowledge. Table 2 presents the knowledge score distributions by domain, and Table 3 presents the item-wise knowledge assessment.
Attitudes toward breast cancer prevention
Participants demonstrated positive attitudes toward breast cancer prevention, with a mean total score of 29.01 ± 1.72 out of 30 (range: 23-30). A ceiling effect was observed, with 112 of 188 (59.6%) achieving the maximum score and 166 of 188 (88.3%) scoring ≥28. Figure 1 illustrates the distribution of responses.
Distribution of Attitude Responses Toward Breast Cancer Prevention (N=188)Horizontal stacked bar chart showing distribution of responses on a five-point Likert scale. No respondents selected 'Disagree' or 'Strongly Disagree' for any attitude item. CBE: clinical breast examination, BSE: breast self-examination.
Breast cancer screening practices
BSE was practiced by 120 of 188 (63.8%) participants. Among those who practiced BSE, frequency varied: 44 of 120 (36.7%) performed it monthly, 20 of 120 (16.7%) every two months, and 56 of 120 (46.7%) yearly or less frequently. CBE uptake was lower, with only 50 of 188 (26.6%) having ever undergone the procedure. Among those who had CBE, 44 of 50 (88.0%) did so only when a problem was noticed rather than as routine screening, while only six of 50 (12.0%) had routine CBE. Mammography was reported by five of 188 (2.7%) participants. No participants were aged ≥40 years, the threshold at which routine mammography screening is recommended for average-risk women. The questionnaire did not distinguish between routine and diagnostic mammography, which represents a study limitation. Regarding general health practices, 150 of 188 (79.8%) reported monitoring their body weight. Regarding physical activity, 75 of 188 (39.9%) engaged in 30 or more minutes of physical activity always or often, while 113 of 188 (60.1%) did so sometimes or never. Table 4 and Figures 2, 3 illustrate BSE practice and frequency distribution.
Frequency of BSE Among Female DoctorsBSE: breast self-examination.
Frequency of CBE Among Female DoctorsCBE: clinical breast examination.
Perceived barriers to screening
Participants identified multiple barriers to breast cancer screening. The most frequently cited barrier was busy schedule or lack of time (134/188, 71.3%), followed by perceived low risk due to being young or healthy (78/188, 41.5%), absence of structured screening programs or reminders for doctors (61/188, 32.4%), limited exposure to breast cancer cases within their specialty (33/188, 17.6%), embarrassment or discomfort during screening (21/188, 11.2%), fear of receiving a serious diagnosis (20/188, 10.6%), lack of awareness about BSE, CBE, or mammography guidelines (20/188, 10.6%), and concerns about radiation exposure from mammography (13/188, 6.9%). Figure 4 presents the barrier frequencies.
Perceived Barriers to Breast Cancer Screening (N=188)BSE: breast self-examination, CBE: clinical breast examination.
Relationship between knowledge, attitudes, and practices
Spearman’s rank correlation analysis was performed to assess relationships between knowledge domains, attitudes, and BSE frequency. A significant positive correlation was found between signs/symptoms' knowledge and screening knowledge (ρ=0.217, p=0.003). A significant positive correlation was observed between total attitude score and BSE frequency (ρ=0.158, p=0.031). No significant correlation was found between total knowledge score and BSE frequency (ρ=-0.061, p=0.409). Table 5 presents the complete correlation matrix.
**Table 5: Spearman's Correlation Matrix for Knowledge, Attitudes, and BSE Frequency (N=188)*p < 0.05, p < 0.01; ρ=Spearman's correlation coefficient. BSE: breast self-examination.
Mann-Whitney U tests revealed no significant differences in knowledge or attitude scores between BSE practitioners (n=120) and non-practitioners (n=68). Total knowledge scores were similar between practitioners (15.95 ± 2.52) and non-practitioners (15.82 ± 3.10; U=4323.5, p=0.494). Similarly, no significant differences emerged for risk factor knowledge (p=0.789), screening knowledge (p=0.257), or total attitude scores (p=0.815). Table 6 presents these comparisons.
Factors associated with BSE practice
Chi-square analysis was performed to identify factors associated with BSE practice. Family history of breast cancer was significantly associated with BSE practice (χ²=6.238, df=1, p=0.013). Among participants with family history, 79.6% practiced BSE compared to 58.3% without family history. Table 7 presents this contingency analysis.
Barrier analysis by BSE practice status
Chi-square analysis was also performed to examine associations between individual barriers and BSE practice. Lack of awareness about screening guidelines was the only barrier significantly associated with non-practice of BSE (χ²=6.720, df=1, p=0.010). Among BSE non-practitioners, 19.1% cited lack of awareness as a barrier compared to only 5.8% of practitioners. Despite being the most frequently cited barrier overall, busy schedule was not significantly associated with BSE practice status (χ²=0.465, p=0.496). Table 8 presents the barrier analysis.
Table 8: Association Between Barriers and BSE Practicep<0.01=statistically significant, χ²: Chi-square value. BSE: breast self-examination, BCa: breast cancer.**
Discussion
In our study, participants demonstrated strong symptom recognition but poor overall breast cancer knowledge, with only 3.2% achieving good total knowledge scores. This mirrors national findings, where only 35% of female nurses in Karachi possessed adequate breast cancer awareness [16]. It also aligns with international evidence showing that symptom recognition consistently outpaces understanding of risk factors and screening protocols among healthcare workers [17-19]. A systematic review by Meshkani et al. confirmed this trend, noting that even healthcare professionals often demonstrate knowledge gaps comparable to the general population [20]. These findings underscore that medical training alone does not ensure comprehensive breast cancer literacy.
Attitudes toward screening were overwhelmingly positive, with most participants strongly endorsing BSE, CBE, and mammography as essential for early detection. However, a clear disconnect emerged between belief and behavior. While 63.8% reported practicing BSE, the quality of practice was inconsistent: only 36.7% performed it at the recommended monthly frequency, and only 46.8% demonstrated knowledge of correct timing. These findings contrast with Reisi et al., who found that 66.4% of Iranian female health workers performed BSE at the appropriate post-menstrual time [21], suggesting that awareness of both frequency and timing remains a gap in our population.
The low mammography uptake (2.7%) warrants contextualization within current international guidelines. The National Comprehensive Cancer Network (NCCN) recommends that average-risk women begin annual mammography at age 40, with clinical breast examinations every one to three years from age 25 to 39 [22]. Similarly, the European Society for Medical Oncology (ESMO) recommends biennial mammography for women aged 50-69, with conditional recommendations for younger age groups [23]. Given that no participants met the ≥40-year threshold for routine mammography, low uptake is expected for average-risk women. However, 49 participants (26.1%) reported a family history of breast cancer, and guidelines recommend individualized risk assessment for such women, which may include earlier imaging with mammography or MRI [22]. Whether these high-risk individuals received appropriate counseling or screening was beyond the scope of this study. Moreover, the suboptimal CBE uptake is concerning, with only 26.6% of participants having ever undergone the examination. This is particularly notable given that both NCCN and ESMO recommend clinical breast examination for women under 40 as a key component of breast awareness and early detection [22,23].
Total knowledge scores showed no significant association with BSE frequency, and Mann-Whitney U tests revealed no significant difference in knowledge between BSE practitioners and non-practitioners (p=0.494). Similarly, knowledge and attitude scores did not differ between those who practice BSE and those who do not. These findings challenge the conventional assumption that knowledge drives behavior, suggesting that higher knowledge levels do not translate into more frequent screening. Heena et al. reported comparable findings among Saudi healthcare professionals, where screening practices fell short despite medical training [18].
Barriers to screening were multifactorial, spanning personal, sociocultural, and system-level domains. Notably, lack of guideline awareness was the only barrier significantly associated with non-practice of BSE (p=0.010). Similar barriers, including affordability, unavailability of female physicians, and fear of diagnosis, have been reported across diverse settings [24,25], suggesting that these obstacles are systemic rather than population-specific. Family history emerged as a significant facilitator of BSE practice. Participants with affected relatives were significantly more likely to practice BSE than those without (79.6% vs. 58.3%, p=0.013), suggesting that personal relevance, rather than abstract knowledge, may be the stronger driver of preventive behavior.
These findings carry several implications. First, since knowledge alone did not translate into practice, educational programs must move beyond information delivery to address perceived susceptibility and provide structural support, such as workplace screening programs and reminder systems. Second, the significant association between family history and BSE practice suggests that systematic identification and counseling of women with affected relatives may be an effective, targeted intervention. Third, the finding that lack of guideline awareness was the only barrier significantly associated with non-practice highlights that even physicians require regular updates on current screening recommendations through continuing medical education. Finally, given that both NCCN and ESMO recommend CBE for women aged 25-39, healthcare institutions should facilitate access to clinical breast examination for their own female staff through dedicated wellness or occupational health programs. Qualitative approaches, such as interviews or focus groups, are needed to explore the psychological and contextual factors underlying the knowledge-practice gap. Multi-center studies across Pakistan would help determine the generalizability of these findings.
Strengths of this study include diverse representation across clinical specialties, comprehensive assessment of knowledge across multiple domains, and statistical analysis of knowledge-practice relationships beyond descriptive findings. The focus on female doctors who serve as both healthcare providers and role models addresses an important gap in the literature. Limitations include the single-center design, which may limit generalizability, and reliance on self-reported practices that may be subject to recall or social desirability bias. Additionally, the questionnaire did not distinguish between routine and diagnostic mammography.
Conclusions
This study demonstrates that female doctors at a tertiary care hospital in Peshawar possess strong awareness of breast cancer warning signs and favorable attitudes toward screening, yet their actual screening practices remain suboptimal. The absence of a significant correlation between knowledge and screening behavior suggests that educational interventions alone are unlikely to bridge this gap. Instead, women with a positive family history perceived themselves to be at higher risk and were therefore more likely to follow recommended breast cancer screening practices.
The low mammography uptake aligns with NCCN and ESMO recommendations, given the young age of participants, but the limited engagement with CBE and inconsistent BSE practice represents missed opportunities for early detection. Barriers such as busy schedules, perceived low risk, and lack of institutional screening programs highlight the need for workplace-based interventions that make screening accessible and routine rather than optional.
These findings call for a shift from knowledge-focused education to structured, institutional screening programs complemented by targeted counseling for at-risk individuals. Female doctors are uniquely positioned as both healthcare providers and role models. Investing in their screening behaviors carries implications that extend well beyond individual health.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Awareness regarding breast cancer amongst women in Pakistan: a systematic review and meta-analysis P Lo S One Abdul Rehman M Tahir E Ghulam Hussain H Khalid A Taqi SM Meenai EA 019202410.1371/journal.pone.0298275 PMC 1091966938452109 · doi ↗ · pubmed ↗
- 2World Health Organization: The Global Breast Cancer Initiative (GBCI): empowering women, building capacity, providing care for all 11 2025 2025 https://www.who.int/initiatives/global-breast-cancer-initiative
- 3Assessment of knowledge and practice of breast self-examination among reproductive age women in Akatsi South district of Volta region of Ghana P Lo S One Dadzi R Adam A 014201910.1371/journal.pone.0226925 PMC 693683831887161 · doi ↗ · pubmed ↗
- 4Global trends and forecasts of breast cancer incidence and deaths Sci Data Xu Y Gong M Wang Y Yang Y Liu S Zeng Q 3341020233724490110.1038/s 41597-023-02253-5PMC 10224917 · doi ↗ · pubmed ↗
- 5Breast cancer knowledge and perception among healthcare professionals and senior medical students at Bolan Medical Complex Hospital Quetta, Pakistan J Pak Med Assoc Gul P Mansoor M Gul P Arshad Z 243224367020203347555810.47391/JPMA.323 · doi ↗ · pubmed ↗
- 6American Cancer Society: Breast cancer risk and prevention 12 2025 2025 https://www.cancer.org/cancer/types/breast-cancer/risk-and-prevention.html
- 7National Breast Cancer Foundation Inc: Breast cancer signs and symptoms 11 2025 2025 https://www.nationalbreastcancer.org/breast-cancer-symptoms-and-signs
- 8Heartfile: National action plan for prevention and control of non-communicable diseases and health promotion in Pakistan 11 2025 2004 https://www.heartfile.org/pdf/NA Pmain.pdf 15745323 · pubmed ↗