Neonatal Netherton syndrome: Dermoscopic clues for early diagnosis
Suttikit Pikulpol, Parith Wongkittichote, Sanchawan Wittayakornrerk

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1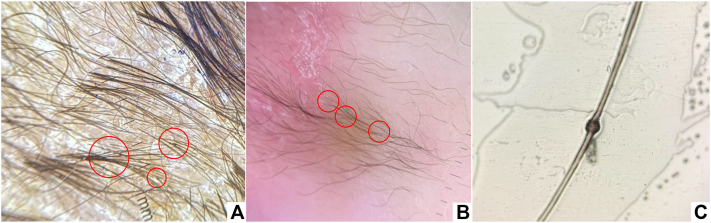 Figure 2
Figure 2 Figure 3
Figure 3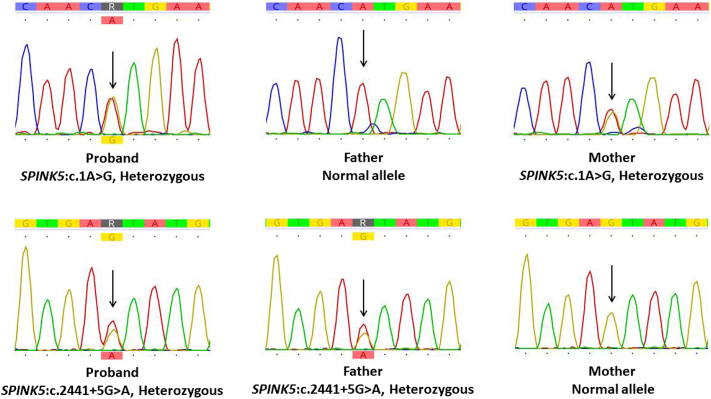 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSkin and Cellular Biology Research · Genetic and rare skin diseases. · Sympathectomy and Hyperhidrosis Treatments
Introduction
Netherton syndrome (NS) is a rare autosomal recessive disorder caused by loss-of-function mutations in the SPINK5 gene, which encodes lymphoepithelial Kazal-type-related protease inhibitor (LEKTI).1^,^2 It is characterized by a triad of congenital erythroderma or exfoliative dermatitis, hair shaft defects—most notably trichorrhexis invaginata (TI)—and atopic diathesis.1^,^3 The clinical presentation in neonates is often nonspecific, frequently leading to delayed diagnosis or misdiagnosis as other causes of neonatal erythroderma. Detection of TI, or “bamboo hair,” is pathognomonic for NS and provides a key diagnostic clue, although its recognition during the neonatal period remains uncommon.
Case report
A 30-day-old Thai female neonate was referred to our hospital for evaluation of progressive skin desquamation. She was born at 37 weeks of gestation via vaginal delivery, with a birth weight of 2715 g. Her perinatal course was complicated by moderate hypoxic-ischemic encephalopathy (HIE), for which she received therapeutic hypothermia for 72 hours. On day 6 of life, she developed ventilator-associated pneumonia. Tracheal aspirate cultures grew Stenotrophomonas maltophilia, and she was treated with intravenous levofloxacin for 10 days.
Since birth, the infant had diffused fine scaling and peeling of the skin, most prominent on the hands. By day 21 of life, her condition progressed to extensive exfoliative dermatitis. There was no family history of ichthyosis or other dermatologic disorders.
At a presentation to our hospital on day 30 of life, her vital signs were stable: temperature 36.5 °C, heart rate 160 bpm, respiratory rate 48 breaths/min, and blood pressure 99/60 mmHg. Growth parameters were below the third percentile (weight 2780 g; length 46 cm). Dermatologic examination revealed thick, yellowish, adherent scales over the scalp and face, patchy alopecia, and diffuse erythematous, scaly plaques on the trunk and extremities (Fig 1). Sparse scalp hair was noted, while nails and mucous membranes appeared normal.Fig 1. Exfoliative dermatitis with localized alopecia in 30 day-old-female infant.
Given the presence of neonatal exfoliative dermatitis with alopecia, further systemic evaluation was undertaken. A dermoscopic examination of the hair and eyebrows, also known as trichoscopy, revealed hair shaft abnormalities suggestive of TI (Fig 2, A and B), confirmed by light microscopy as “bamboo hair” (Fig 2, C), supporting a clinical diagnosis of Netherton syndrome.Fig 2. Trichoscopic images show trichorrhexis invaginata (red circle) of the scalp hair (A) and eyebrows (B). Microscopic image of trichorrhexis invaginata (C).
Laboratory investigations revealed peripheral eosinophilia (absolute eosinophil count of 1600 cells/μL; normal <700/μL), hypernatremia (serum sodium 153 mmol/L; normal 135-145 mmol/L), and elevated serum specific IgE (160 IU/mL; normal <15 IU/mL in infants). Supportive management included intravenous hydration for dehydration, thermal regulation through incubator humidity adjustment, and aggressive topical therapy with emollients (petroleum jelly and liquid paraffin). These interventions led to significant improvement in skin condition, normalization of electrolytes, and stabilization of body temperature (Fig 3). The patient was discharged home after 2 weeks of hospitalization. On follow-up in the outpatient clinic, her skin continued to improve with ongoing emollient therapy, and no significant infectious complications were observed.Fig 3. Clinical improvement following treatment.Fig 4. Sanger sequencing of the proband and the parents.
Exome sequencing was performed (the Illumina NovaSeq X Plus platform, South Korea). Variant analysis was guided by Human phenotype ontology terms “erythroderma,” and “ichthyosis,” to prioritize clinically relevant genetic variants. Two heterozygous variants in the SPINK5 gene were detected: c.1A>G (p.Met1?) and c.2441+5G>A. The variants are present in a trans configuration, with each parent identified as a heterozygous carrier through Sanger sequencing as shown in Fig 4.
Discussion
TI is considered pathognomonic for NS.2, 3, 4 The onset of hair shaft abnormalities in NS is variable and typically becomes more apparent after the first year of life, when hair growth is more developed.4, 5, 6, 7, 8 However, a few case reports have documented earlier detection during the neonatal or early infantile period. For instance, Okulu et al9 identified TI in a neonate with genetically confirmed NS using light microscopy, while Di Nora et al10 reported videodermoscopy findings of TI in a 1-month-old infant. These observations suggest that although TI often develops progressively, subtle hair shaft deformities may already be present during the neonatal period. Conversely, Burk et al6 observed a delayed onset of hair abnormalities—hair shafts appeared normal at ages 2 and 4 years but later demonstrated TI, which was identified by dermoscopy at 7 years of age. Nevertheless, the absence of TI in early life does not preclude a diagnosis of NS.
In our patient, generalized exfoliative dermatitis, growth retardation, and elevated serum IgE were observed—findings commonly associated with NS. However, these clinical features overlap with other causes of neonatal erythroderma, including congenital ichthyoses, severe atopic dermatitis, Omenn syndrome, and infections such as staphylococcal scalded skin syndrome or candidiasis.5 A distinguishing feature in this case was the early detection of hair shaft anomalies through dermoscopy, which played a pivotal role in narrowing the differential diagnosis.5, 6, 7, 8
Dermoscopy, a noninvasive and bedside-accessible tool, revealed abnormalities in both scalp and eyebrow hair, prompting further examination with light microscopy. However, its role in neonates remains underrecognized. Previous reports have rarely highlighted dermoscopy as a frontline diagnostic tool in this age group, despite its advantages: it is rapid, noninvasive, widely available, and feasible at the bedside. In our patient, dermoscopy provided a critical diagnostic clue that would otherwise have been missed, as skin biopsy in neonates is less desirable and hair sampling may be limited.
In our patient, exome sequencing identified compound heterozygous variants in SPINK5. The initiation codon change (c.1A>G) is predicted to cause loss of function due to decreased protein synthesis, as reported by et al.11 In addition, the splice-site variant (c.2441+5G>A) was predicted to cause splicing aberration using SpliceAI, as described by Jaganathan et al.12 Both variants are likely to result in loss of function of the SPINK5 protein, thereby confirming the diagnosis of Netherton syndrome.
This case underscores the potential of dermoscopy to bridge a diagnostic gap in neonatal erythroderma. To our knowledge, only a limited number of cases in the literature have emphasized the utility of dermoscopy in the neonatal period for diagnosing hair shaft abnormalities. Early recognition of NS is clinically important, as affected neonates are at high risk of dehydration, electrolyte imbalance, recurrent infections, and failure to thrive. Early supportive measures, as demonstrated here, may improve outcomes and prevent complications.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bellon N.Hadj-Rabia S.Moulin F.The challenging management of a series of 43 infants with Netherton syndrome: unexpected complications and novel mutations Br J Dermatol 1843202153253710.1111/bjd.1926532479644 · doi ↗ · pubmed ↗
- 2Chavanas S.Bodemer C.Rochat A.Mutations in SPINK 5, encoding a serine protease inhibitor, cause Netherton syndrome Nat Genet 252200014114210.1038/7597710835624 · doi ↗ · pubmed ↗
- 3Bitoun E.Chavanas S.Irvine A.D.Netherton syndrome: disease expression and spectrum of SPINK 5 mutations in 21 families J Invest Dermatol 1182200235236110.1046/j.1523-1747.2002.01603.x 11841556 · doi ↗ · pubmed ↗
- 4Smith V.V.Anderson G.Malone M.Sebire N.J.Light microscopic examination of scalp hair samples as an aid in the diagnosis of paediatric disorders: retrospective review of more than 300 cases from a single centre J Clin Pathol 581220051294129810.1136/jcp.2005.02758116311350 PMC 1770794 · doi ↗ · pubmed ↗
- 5Bittencourt M.J.Moure E.R.Pies O.T.Mendes A.D.DepráM.M.Mello A.L.Trichoscopy as a diagnostic tool in trichorrhexis invaginata and Netherton syndrome An Bras Dermatol 901201511411610.1590/abd 1806-4841.2015301125672309 PMC 4323708 · doi ↗ · pubmed ↗
- 6Burk C.Hu S.Lee C.Connelly E.A.Netherton syndrome and trichorrhexis invaginata—a novel diagnostic approach Pediatr Dermatol 252200828728810.1111/j.1525-1470.2008.00663.x 18429812 · doi ↗ · pubmed ↗
- 7Akkurt Z.M.Tuncel T.Ayhan E.Uçmak D.Uluca U.Uçak H.Rapid and easy diagnosis of Netherton syndrome with dermoscopy J Cutan Med Surg 184201428028210.2310/7750.2013.1310625008447 · doi ↗ · pubmed ↗
- 8Rakowska A.Kowalska-Oledzka E.Slowinska M.Rosinska D.Rudnicka L.Hair shaft videodermoscopy in netherton syndrome Pediatr Dermatol 263200932032210.1111/j.1525-1470.2008.00778.x 19706096 · doi ↗ · pubmed ↗