Breast Cancer Brain Metastases: Current Understanding and Future Directions
Mohammad Alabdulrahman, Gordon R. Daly, Sindhuja Naidoo, Lea Stuart, Sami Almasri, Ali Benour, Jason McGrath, Minatoullah Habaka, Gavin P. Dowling, Cian M. Hehir, Arnold DK. Hill, Damir Varešlija, Leonie S. Young

TL;DR
This paper reviews recent progress in understanding how breast cancer spreads to the brain, highlighting new mechanisms and diagnostic tools that could improve treatment.
Contribution
The paper synthesizes recent findings on metastatic mechanisms and introduces novel diagnostic approaches for breast cancer brain metastases.
Findings
JAK–STAT signaling, homologous recombination deficiency, and c-MYC are implicated in BCBM progression.
Tumor cells adapt through neuronal mimicry and metabolic reprogramming, interacting with astrocytes and microglia.
Receptor discordance occurs in up to one-third of cases, potentially affecting systemic therapy choices.
Abstract
To examine recent advances in understanding breast cancer brain metastases (BCBM), with emphasis on metastatic mechanisms, tumour-microenvironment interactions, receptor discordance between primary breast tumours and brain metastases, diagnostic innovations, and therapeutic strategies. The review sought to clarify how these developments inform precision management and identify priorities for future research. Studies implicate JAK–STAT signalling, homologous recombination deficiency, c-MYC, PI3K/AKT/mTOR, and RET in BCBM progression. Tumour cells adapt via neuronal mimicry, metabolic reprogramming, and crosstalk with astrocytes and microglia. Receptor discordance between primary breast cancers and brain metastases occurs in up to one-third of cases and may alter systemic therapy. Emerging tools including liquid biopsy, spatial transcriptomics, and radiomics offer minimally invasive…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
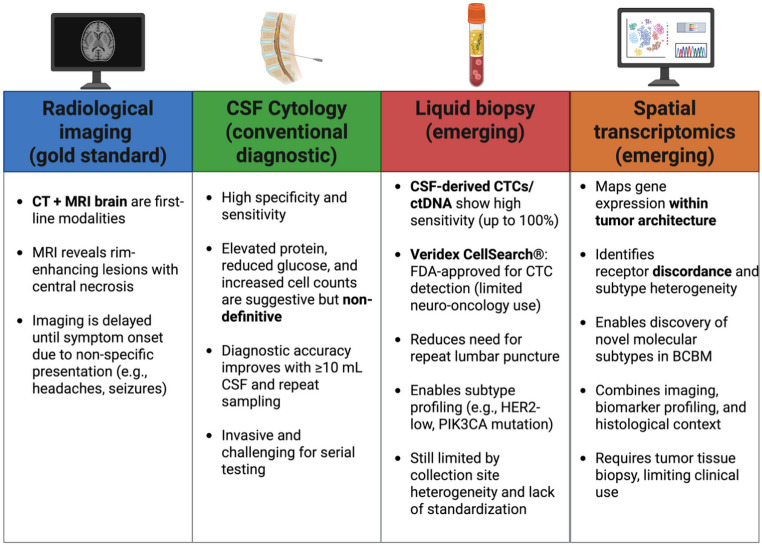 Figure 1
Figure 1- —Royal College of Surgeons in Ireland (RCSI)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBrain Metastases and Treatment · Glioma Diagnosis and Treatment · Cancer-related cognitive impairment studies
Introduction
Brain metastases occur in up to 40% of patients with breast cancer and remain a major cause of morbidity and mortality despite advances in systemic control and neuroimaging [1, 2]. Breast cancer brain metastases (BCBM) present unique clinical and biological challenges, arising from both the intrinsic aggressiveness of certain breast cancer subtypes and the distinct selective pressures of the central nervous system microenvironment. Once tumour cells reach the brain, they must adapt to its specialised neural and vascular niche, remodel the blood brain barrier, and engage in dynamic interactions with astrocytes, microglia, and neurons. These processes are increasingly recognised within the growing field of cancer neuroscience. Such adaptations are driven by diverse oncogenic pathways, genomic instability, and changes in receptor status, which together influence both disease progression and therapeutic response. At the same time, novel diagnostic approaches such as liquid biopsy and spatial transcriptomics, together with evolving systemic and local treatments including targeted agents, immunotherapy, and brain penetrant drugs, have the potential to influence management strategies, although their clinical roles remain under evaluation. This review synthesises current knowledge of metastatic mechanisms, receptor discordance, diagnostic advances and treatment developments, while examining how computational modelling and neurobiological insights may work together to guide future precision strategies in BCBM.
Established Metastatic Pathways
Plasticity and Microenvironment Interactions
JAK/STAT Pathway
The Janus kinase/signal transducer and activator of transcription is an important regulator of the microenvironment surrounding BCBM. Under normal conditions, the JAK/STAT3 pathway acts in promoting the activation of A2 reactive astrocytes (RA), which are implicated in scar-formation following ischemia [3]. This pathway is also involved in the initiation of astrogliogenesis and subsequently the maturation of astrocytes during developmental stages of the brain [3]. The role of JAK/STAT3 in metastasis has been a topic of exploration across recent studies such as that of Priego et al., who demonstrated the elevated expression of activated STAT3 and its promotion of metastases in both human and mouse samples [4]. The secretomes of these STAT3 expressing RAs include several immunosuppressive molecules such as vascular endothelial growth factor-A (VEGF-A), lipocalin-2, programmed cell death ligand 1 (PD-L1), and tissue inhibitor of metalloproteinases-1 (TIMP-1) [4]. Taken together with the observed reinforcement of the extracellular matrix of these cells, they may contribute to an immunosuppressive microenvironment that impedes immune cell access, particularly to the access of CD8 + cytotoxic T cells [4]. Moreover, STAT3 + RAs demonstrate elevated expression of CD74 + macrophage migration inhibitory factor (MIF) and increased binding to CD74 + microglia, establishing a form of “cross-talk” between microglia and RAs, which results in the upregulation of the nuclear factor (NF)–κB signalling pathway and supporting an environment permissive to metastatic progression in experimental models [5].
DNA Repair and Genomic Instability
Homologous Recombination Repair Deficiency (HRD)
The homologous recombination repair pathway (HRR), is a complex pathway, comprised of multiple genes that contribute to high-fidelity repair of damaged DNA. HRD and has been linked with the development of brain metastasis and shown to be more prevalent when brain metastasis develops. Abnormalities within this pathway, particularly relating to repair genes such as BRCA1/2, PALB2, RAD51C, ATM, CHEK2 and many other genes, have been associated with an increased risk of developing breast cancer [6, 7]. HRD status has crucial implications for therapeutic response to both PARPis and platinum-based chemotherapies [8, 9].
Studies have reported increased levels of HRD in BCBM compared to primary breast cancer and that HRD may be present independent of somatic and germline mutations in HRD pathway genes [10, 11]. These studies highlight two plausible causes for this phenomenon: (1) clonal selection of primary tumour cells with higher HRD scores, the greater the instability, the more potential for the cells to adapt to new microenvironments within the brain; (2) genomic instability develops due to an unidentified mechanism, as the metastases develop [10, 11].
These studies highlight the presence of HRD in BCBM, independent of primary tumour mutations, and the role that HRD plays in the progression of breast cancer to the brain. Further research into the gene abnormalities within the HRR pathway, will provide an opportunity for novel therapeutics, to be used and developed based on the deficiencies and abnormalities of genes within the HRR pathway [12]. Recent studies explore therapeutic agents that target some of the known mutations which have been evaluated in clinical trials for their efficacy in HRD-positive BCBM [13].
The OlympiAD trial has successfully highlighted the benefit of olaparib and talazoparib, both of which are PARP inhibitors (PARPis) that target HRD-positive metastatic breast cancer, in patients with BRCA1/2 mutations [14]. Similarly, the EMBRACA trial explored the overall survival of patients with metastatic breast cancer, treated with talazoparib vs. chemotherapy. Talazoparib is approved in the US, EU, and other countries for Human Epidermal growth factor Receptor 2-negative (HER2-), locally advanced or metastatic breast cancer with BRCA1/2 mutations [15]. Newer PARPis such as AZD9574 and pamiparib have exhibited increased BBB penetrance in pre-clinical in vivo studies promoting increased drug deliverance, while reducing toxic side effects. These findings suggest potential for future clinical application, pending validation [16, 17].
Current ongoing clinical trials such as NCT06458712 are investigating the impact of DSB2455 monotherapy in patients with HRD positive advanced malignancies, including BCBM [18]. DSB2455 is a PARP inhibitor with strong CNS penetrance, the results of this clinical trial are expected to clarify whether CNS-penetrant PARPis offer clinical benefit [18]. Research on the effects of individual and/or combined targeted therapies on BCBM is important to continue expanding effective treatment options for patients [10]. Further areas of interest include: novel agents targeting the HRR repair pathways, such as ATR and WEE1 inhibitors [19]. Ongoing research to determine their potential clinical applicability to brain metastases has not yet been addressed but holds promise for future application in BCBM [19].
c-MYC
The MYC gene, specifically the c-MYC isoform, plays an important role in breast cancer progression and metastasis, including to the brain. Because of its role as a transcription factor, c-MYC regulates genes involved in cell proliferation, metabolism, and apoptosis [20]. Overexpression of c-MYC is often observed in aggressive breast cancers and is associated with poor prognosis. In the context of brain metastases, c-MYC has been shown in preclinical models to enhance the invasive capacity of breast cancer cells, facilitating their colonization in the brain microenvironment [20].
Furthermore, c-MYC contributes to metabolic reprogramming of cancer cells, promoting aerobic glycolysis and lipid metabolism, which are essential for tumour growth and survival in the brain environment. This ‘reprogramming’ supports the energy demands of rapidly proliferating metastatic cells and aids in their adaptation to the brain niche [21]. Additionally, c-MYC influences the tumour microenvironment by promoting angiogenesis and immune evasion, further supporting metastatic progression [20, 21].
Interestingly, while c-MYC drives metastasis, it also renders brain-metastatic breast cancer cells more susceptible to certain therapies, such as TRAIL-induced apoptosis, suggesting a potential for therapeutic applications [22]. A recent cohort study of 42 BCBM samples were analysed using whole exome sequencing (WES) and total RNA sequencing and showed evidence of increased expression of MYC gene in BCBM samples in comparison to primary tumour samples [23].
A recent phase 1 clinical trial on the use of OMO-103, a MYC inhibitor, on solid tumours, including triple negative breast cancer (TNBC) was published [24]. This trial reported preliminary antitumour activity of OMO-103, including in combination with chemotherapy, immunotherapy and personalised approaches, citing the importance of continued investigation into the use of MYC inhibitors [24]. There are currently no preclinical investigations into the use of this targeted therapy in breast cancer, further specific studies into the use of MYC inhibitors is needed to gain insight into the potential clinical applicability in other BC subtypes and BCBM.
ARID1A
AT-rich interactive domain-containing protein 1 A (ARID1A) codes for key proteins in the SWI/SNF chromatin remodelling complex, an important complex for gene expression and chromatin remodelling [25]. Inactivating mutations in ARID1A despite being found in only 2.5% of all breast cancers, are found in 12% of treatment resistant metastatic breast cancer suggesting a possible role in breast cancer metastasis [26]. The rationale behind this is that ARID1A regulates EMT activity; therefore, deactivation of ARID1A leads to increased cell proliferation, migration, invasion, angiogenesis, and reduces sensitivity to some chemotherapy [27].
Along with chemotherapy ARID1A is importantly implicated in the response to endocrine therapy via key interactions with various transcription factors. For instance, ARID1A helps maintain ER signalling, making it essential for the responsiveness of drugs.
that target oestrogen including tamoxifen [28]. Tamoxifen-bound ER primarily represses gene expression by binding to enhancer regions and signalling for ARID1A to recruit histone deacetylase 1 (HDAC1), an important histone-modifying enzyme that silences gene expression. When ARID1A is lost, HDAC1 recruitment fails, histone acetylation increases, and the chromatin remains active, leading to ER therapy resistance [26]. Thus, ARID1A mutations have been linked to more aggressive tumour behaviour, worsening prognosis and potentially a subsequent increased risk for brain metastasis.
Given these mechanistic insights, there is currently very limited research into therapies specifically targeting ARID1A enriched BCBM. However, several early-phase trials are underway with an ongoing clinical trial (NCT05490472), assessing the use of Aurora A kinase inhibitor JAB-2485 monotherapy in patients with advanced Estrogen Receptor-Positive (ER+) breast cancer, TNBC, and ARID1A mutant solid tumours [29]. Additionally, clinical trial (NCT04957615) is in phase II trial studies on the use of nivolumab on patients with metastatic malignant solid tumours and unresectable solid tumours with ARID1A mutations and CXCL13 expression [30]. While both studies include patients with brain metastases, there is a clear criteria of exclusion for patients with active progression of their brain metastases. The result of these ongoing clinical trials are expected to provide insight provide insight into the clinical relevance of targeted agents for the ARID1A mutation and their efficacy against cancers with this mutation in advanced solid tumours. There are currently no ongoing studies into the use of targeted therapeutics in specifically BCBM patients with ARID1A mutations. These trials may inform future studies evaluating whether targeted agents could benefit ARID1A-altered BCBM.
Receptor-driven Targeted Axes
PI3K/AKT/mTOR
Another well-known pathway that is activated in 43–70% of patients with BCBM, is the PI3K/AKT/mTOR pathway [31]. PI3K is a lipid kinase family, with Class I being the most relevant in BCBM [32]. Upon the activation of PI3K, PIP2 converts to PIP3, which subsequently results in signalling via AKT and mTORC1 leading to cell growth and survival [32]. The mechanistic target of rapamycin (mTOR) functions as a critical oncogenic driver in multiple malignancies. As a serine/threonine kinase, mTOR integrates signals from growth factors, nutrients, and cellular energy status to regulate proliferation, protein synthesis, and survival [33]. In breast cancer, aberrant activation of the PI3K/AKT/mTOR axis, often due to PIK3CA mutations or PTEN loss, leads to constitutive mTOR signalling, enhancing metastatic potential [34]. In the brain microenvironment, where metabolic constraints and immune evasion are crucial for tumour survival, mTOR activity supports cellular adaptation and outgrowth [35]. Its role as an oncogene is further highlighted by evidence linking mTOR hyperactivation with poor prognosis and resistance to therapy [36]. These findings justify continued exploration of mTOR-targeted therapies, especially brain-penetrant inhibitors, in managing breast cancer brain metastases [31].
A preclinical study using WES of 86 matched BCBM samples, were analysed. Alterations in the PI3K/AKT/mTOR pathway was detected in the BCBM samples [37]. There were 43 alterations in the 37 cases that occurred in 10 of the total 15 genes that were evaluated [37]. 14 of the 43 alterations were detected only within the BCBM samples, and 24 were shared between primary tumour and BCBM, the remaining 5 were found only in the primary sample [37]. A further analysis of the four cases with PI3K mutations, showed that all metastatic sites shared the PIK3CA mutation and were treated with a PI3K inhibitor, with no evidence of intracranial disease progression for 8 months [37]. This was further supported in another preclinical study using dual PI3K/mTOR inhibitors (GDC-0084) and establishing their use as inhibitors of the metastatic process [31]. PIK3CA-mutant and wild type breast cancer cell lines, as well as in vivo GDC-0084 on BCBM xenograft mouse models were used [31]. This study highlighted the role of GDC-0084, which inhibited only the wild-type cell line in vitro, while in-vivo treatment showed significant inhibition of growth of the PIK3CA-mutant [31].
Furthermore, the recent development of MEN1611, an investigational drug agent that blocks the PI3K protein in cancer cells, has been investigated in clinical trials such as the B-Precise-01 trial. B-Precise-01 (NCT03767335) investigated the use of MEN1611 in combination with trastuzumab, with or without fulvestrant, for the treatment of metastatic or advanced HER2 + breast cancer. The results of this trial highlight the positive response against the HER2+/PIK3CA-mutated advanced or metastatic breast cancer, as well as the duration of response in this patient group [38]. Another clinical trial of note targeting the PI3K mutation is the SABINA trial which is currently an ongoing phase II clinical trial investigating the efficacy and safety of MEN1611 monotherapy or in combination with eribulin in HR/HER2 negative PIK3CA/PTEN-altered, unresectable advanced or metastatic metaplastic BC patients [39]. The results of this clinical trial will provide new insight into the PI3CA mutation and its role in BCBM, as well as the clinical significance of targeted therapies such as MEN1611.
RET
RET is a specific oncogene, with three main isoforms RET9, RET51 and RET43. RET9 and RET51 have been expressed in multiple breast cancer cell lines, with varying degrees of expression and signal transduction [11]. RET has primarily been studied in ER + breast cancer, with ER activation inducing RET expression, thus driving cell proliferation [11].
A recent study assessed RET function in a cohort of patients with primary and brain metastatic tumours [40]. In vivo models, organoid models and brain organotypical cultures were used, with RNA sequencing [40]. This study showed a statistically significant level of RET in brain metastases in ER + breast cancer [40]. Subsequently RET overexpression augmented the processes in cell adhesion, using epidermal growth factor receptors (EGFR) to subsequently deliver a “pro-brain metastatic phenotype” [40]. This novel finding specifically with regard to the actions and functions of RET in BCBM, has shown the statistically significant role of the RET oncogene in regulating the colonization and outgrowth of BCBM. Gattelli et al. used in vivo inhibition of RET in a metastatic breast cancer model, showing inhibited tumour growth and metastatic potential [41]. These findings further supported the possible role of RET in the metastatic pathway of BCBM [41]. While the exact mechanisms are not completely understood in subtypes other than ER + breast cancer, there is significant evidence supporting the role of the RET oncogene in the metastatic pathway of breast cancer [41].
There are no current clinical trials that specifically investigate targeted therapies against BCBM with known RET mutations. The LIBRETTO-431 trial was conducted in patients with non-small cell lung cancer (NSCLC), 42 of the 192 patients had brain metastases. 82% of the patients with brain metastases who were given selpercatinib demonstrated intracranial response. selpercatinib is a highly selective, brain penetrant RET-kinase inhibitor [42]. Furthermore, patients with RET positive NSCLC that were treated with selpercatinib experienced longer progression-free survival in comparison to those receiving chemotherapy with or without pembrolizumab [42]. Additionally, the LIBRETTO-001 trial focused specifically on brain metastases originating from NSCLC, highlighting the efficacy of selpercatinib in shrinking metastases [43]. The overexpression of the RET gene is of functional importance, raising the possibility that RET inhibitors such as selpercatinib and pralsetinib could benefit BCBM patients with RET alterations, although this requires dedicated clinical studies.
HER3
HER3 is a protein receptor from the EGFR tyrosine kinase family, which is known to be expressed at higher levels in metastatic breast cancer in comparison to primary tumour samples [44]. HER3 has two ligands, namely heregulin (HRG) and neuregulin-1 (NRG1), with HRG being more commonly expressed in the brain [45]. A recent study using luminal breast cancer cell lines in vivo, highlighted the activity of HRG. HRG secretion in the brain promotes the dimerization of HER2/3 thus promoting the metastatic process [45].
Newer studies show that although the HER3 protein does not cause tumorigenesis directly, the HER2:HER3 heterodimer has significant ability to mediate HER-2 tumorigenesis in breast cancer [46]. This heterodimerization has become a key therapeutic target, with monoclonal antibodies developed to disrupt this process and potentially prevent the progression of BCBM.
There are currently 3 ongoing clinical trials on the use of HER3-Dxd, which is an antibody-drug conjugate. ICARUSBREAST02 (NCT06298084) investigates HER3-Dxd monotherapy and in combinations, in patients with advanced inoperable breast cancer [47]. NCT06172478 is ongoing and investigates HER3-Dxd monotherapy in advanced solid tumours, including breast cancer [48]. The two studies aforementioned had strict criteria regarding BCBM, with patients included only if they had clinically inactive BCBM.
Additionally, NCT04338747 is a phase IIa study of dendritic cell vaccines against HER2/HER3 and pembrolizumab in patients with asymptomatic brain metastases from TNBC or HER2 + BC or HR + BC [49]. This clinical trial may highlight the potential impact of immunotherapy against HER3 BCBM, the results of this may guide further clinical studies into targeted therapies for BCBM possessing HER3 mutations.
BCBM: Advances in Diagnostics
The following section will provide a brief overview of the current ‘gold standard’ diagnostic methods by evaluating their efficacy, advantages, and limitations, followed by an exploration of emerging diagnostic approaches for BCBM (Fig. 1).
Fig. 1. The figure gives an overview of current and emerging diagnostic approaches for brain metastases. Created from https://www.biorender.com/
BCBM often presents with non-specific clinical symptoms, leading to a delay in diagnosis until the tumor burden is large enough to cause compressive effects. The diagnostic evaluation typically includes a comprehensive medical history, physical examination and neuroimaging. Additionally, cerebrospinal fluid (CSF) cytomorphological analysis, and, where necessary, tissue biopsy may be performed to assess changes in receptor status [2]. Commonly patients present with headaches, seizures, cognitive impairments, or focal neurological deficits [2]. CT followed by MRI brain are first-line imaging investigations in patients suspected to have BCBM [50]. MRI findings of rim-enhancing lesions with central non-enhancing regions are characteristic of the disease [51].
CSF abnormalities suggestive of metastatic brain or leptomeningeal disease, such as elevated cell counts, reduced glucose levels, and increased protein concentrations are not definitive markers [52]. CSF cytomorphological analysis, while highly specific for detecting solid tumours, suffers from low sensitivity due to the typically low volume of malignant cells in CSF. Older retrospective work reported a sensitivity of only 59% for a single CSF sample in patients later confirmed to have BCBM at autopsy, but this underestimates current diagnostic potential [53]. More recent studies have demonstrated substantially higher diagnostic accuracy with advanced approaches. For example, one prospective study by Darlix et al. showed 100% sensitivity and 77.3% specificity for circulating tumour cell (CTC) detection in CSF among patients with confirmed leptomeningeal or intraparenchymal metastatic breast cancer, aligning with previous reports of sensitivities of 78–100% and specificities of 84–100% [54, 55]. Le Rhun et al. successfully identified CTCs in 5 mL of CSF using the Veridex CellSearch^®^ system, which employs ferromagnetic EpCAM antibodies and remains the only FDA-approved methodology for enumerating CTCs in patients with breast, prostate, colorectal, or lung cancers [56, 57]. Importantly, CTC assays reduce the need for multiple CSF samples, addressing a major limitation of conventional cytology [58, 59]. Current guidelines still recommend analysing at least 10 mL of CSF and performing repeated sampling to optimize diagnostic accuracy [60, 61], but these advances suggest that liquid biopsy methods may help overcome some of the historic limitations of cytology. Despite these advantages, CSF collection is invasive and poses challenges for repeated sampling. Furthermore, the heterogeneity of CSF composition based on collection site (e.g., thoracic vs. lumbar spine) necessitates a standardized sampling protocol [62]. Longitudinal sampling at different diagnostic stages, during treatment, and in follow-up care could enable more comprehensive analyte monitoring and assessment of recurrence. However, further research is required to establish the optimal role of liquid biopsies in BCBM diagnostics, whether as a primary diagnostic tool, a surveillance strategy, or both.
Beyond CTCs, liquid biopsy approaches also include analysis of cell-free DNA (cfDNA) and circulating tumour DNA (ctDNA), which are under active investigation, with limited current clinical validation in BCBM [63]. While widely utilized in oncology for prognostication, treatment stratification, and post-therapy surveillance, their application in neuro-oncology remains limited [64].
A promising second avenue for future diagnostic advancements is the field of spatial transcriptomics. Despite significant progress, cancer treatment still encounters many challenges, including drug resistance, recurrence, and metastasis. High-throughput transcriptomics, commonly referred to as RNA sequencing, has enabled the identification of numerous alterations in gene expression across various tumor types [59]. However, traditional bulk sequencing methods lack the resolution necessary to capture details of the tumor microenvironment and cellular heterogeneity [65, 66]. Similarly, techniques such as single-cell RNA sequencing face limitations, including the dissociation of cells from their original spatial context within the tissue. Spatial transcriptomics can mitigate some of these limitations by combining biomarker analysis, imaging, genetic sequencing, and bioinformatics to map gene expression within intact tissue samples. This approach reveals the spatial distribution of diverse cell types within tissues and elucidates the interactions between these cell populations, providing a more comprehensive understanding of the tumor microenvironment and its complexity [62]. For example, a study utilizing spatial transcriptomics analyzed the genetic landscape of brain metastases originating from TNBC. The researchers compared the molecular characteristics of primary TNBC tumors with their corresponding brain metastases, uncovering distinct genetic profiles between the tumor cells and the surrounding tumor microenvironment. This comprehensive analysis provided insights into the molecular subtypes present in BCBM, highlighting the heterogeneity between primary and metastatic sites [67]. Specific application of spatial transcriptomics in BCBM is used in the identification of molecular subtypes of breast cancer, as frequently the metastatic lesion will differ from the primary cancer [68]. Not only does this allow for a better understanding of the specific tumor microenvironment, but high-resolution single-cell transcriptome sequencing, combined with spatial analysis, enables the visualization of cellular heterogeneity in both primary and metastatic breast cancer. This approach facilitates both the identification of metastasis-related cell subsets and also contributes to a better understanding of the metastatic process and improves diagnostic accuracy [69]. Furthermore, spatial transcriptomics has been applied to identify new breast cancer subtypes by analyzing the spatial distribution of gene expression within tumors. This approach provides insights into tumor heterogeneity and supports the development of individualized treatment strategies, specific to the metastatic subtype [68].
Spatial transcriptomics, however, does not come without its current limitations: the need for invasive testing, high cost, long turn-around times, and lack of standardization process to name a few [59, 70]. A comparison of these diagnostic tools is provided in Table 1.
Table 1. Comparison of diagnostic toolsSensitivityInvasivenessSpatial ResolutionCostCSFHighHighN/ALowLiquid BiopsiesHighLowN/ALowSpatial TranscriptomicsUndetermined, predominantly used as a research toolVery highHigh, varies with technique usedHigh
Receptor Discordance between Primary Tumour and Brain Metastasis
Receptor discordance, defined as the variation in ER, progesterone receptor (PR), HER2 status between primary breast cancer and metastatic sites, is a well-documented phenomenon in metastatic breast cancer (MBC) [71–73]. This biological and clinical challenge is particularly relevant in BCBM, where receptor discordance between primary and metastatic sites remains a clinically significant issue. Although rates of discordance in BCBM are not consistently higher than those observed in other metastatic sites such as bone, changes in receptor status have been reported in a substantial proportion of cases, with one large multicentre study reporting an overall discordance rate of 36.3% and receptor-specific rates of 16.7% for ER, 25.2% for PR, and 10.4% for HER2 [74, 75]. These shifts can directly influence therapeutic strategies and highlight the broader importance of reassessing receptor status in BCBM.
Supporting this, two meta-analyses have highlighted significant discordance rates: ER discordance was observed in 19–20% of cases, PR discordance in 30–33%, and HER2 discordance in 8–10%. Notably, brain metastases exhibit an ER discordance rate of approximately 20.8%, reflecting a substantial shift in receptor expression profiles within the central nervous system (CNS) microenvironment, and subtype switching has been observed in nearly one-quarter of patients, often involving hormone receptor loss or HER2 gain [72, 75]. Importantly, 14.8% of patients who were HER2- at baseline developed HER2 + brain metastases, creating potential therapeutic opportunities, while receptor loss, particularly ER- has been associated with worse survival outcomes [75].
Several mechanisms contribute to receptor discordance in metastatic breast cancer, including technical variability in immunohistochemical (IHC) staining, tumour heterogeneity, and clonal evolution under therapeutic pressure. Bone and brain metastases, in particular, are susceptible to these alterations, likely due to distinct microenvironmental influences and selective pressures favouring specific tumour subpopulations.
- Tumour Heterogeneity and Clonal Selection: The existence of intra-tumour heterogeneity suggests that primary breast tumours comprise diverse cellular subpopulations with variable receptor expression. As metastases develop, certain clones may be preferentially selected, leading to a receptor status distinct from that of the primary tumour [73, 76–79].
- Therapeutic Influence: Systemic therapies, particularly endocrine and HER2-targeted treatments, may drive receptor conversion. Endocrine therapy, for instance, can induce loss of ER expression, rendering initially hormone receptor-positive (HR+) tumours hormone receptor-negative (HR−). Similarly, HER2-targeted agents such as trastuzumab can alter HER2 expression, affecting treatment responsiveness [80–85]. Emerging data also point to a distinct pattern of HER2-low discordance, wherein some metastatic lesions exhibit low-level HER2 expression despite a HER2- primary tumour. This phenomenon has important therapeutic relevance, particularly with the advent of novel agents targeting HER2-low disease [86].
- Microenvironmental Adaptation: The CNS presents a unique metastatic niche, characterized by the blood-brain barrier, differential immune surveillance, and metabolic constraints. These factors may drive adaptive changes in tumour cell receptor expression, promoting discordance [72, 75, 87, 88].
Prospective studies, including the DESTINY and BRITS trials, have assessed the impact of re-biopsy in metastatic breast cancer, revealing that treatment decisions were altered in 14.2% of patients based on receptor reassessment [89, 90]. In the context of BCBM specifically, these modifications can be particularly consequential, as receptor loss has been linked to inferior survival while HER2 acquisition may improve outcomes [75]. However, whether these modifications translate into improved overall survival remains debated, necessitating further investigation.
Advancing Therapeutic Strategies in BCBM
Radiation Based Therapies
The treatment of brain metastases from breast cancer is often complex due to the varying presentations of the disease and the evolving array of treatment options. Traditional treatments like whole-brain radiotherapy (WBRT) have, to some extent, fallen out of favor with the rise of more targeted approaches such as stereotactic radiosurgery (SRS) and hippocampal-avoidant whole-brain radiotherapy (HA-WBRT). The ASCO-SNO-ASTRO guidelines recommend SRS for patients with 1–4 lesions and HA-WBRT for patients with a projected survival of 4 months or more who do not have hippocampal lesions [91]. Guidelines from EANO-ESMO align with these recommendations, advising WBRT primarily for patients with more than ten brain lesions, those with uncontrolled extra-CNS disease, or individuals with a life expectancy of less than three months [92]. For all other cases, treatment recommendations include surgery combined with SRS or stereotactic radiotherapy, surgery with pharmacotherapy, or pharmacotherapy alone, depending on the patient’s condition and tumor characteristics [92].
This progressive shift away from WBRT is not unfounded. WBRT often results in cognitive decline lasting 5–8 months and, in some cases, 9–15 months, with a greater risk of long-term effects. In contrast SRS has been shown to impair cognitive function, the effects are typically limited to 1–4 months, after which most patients return to baseline cognitive levels [93]. The reduced cognitive impact, combined with other therapeutic benefits, has been a significant factor driving the shift from WBRT.
WBRT has also been supplanted in certain circumstances by HA-WBRT. Using the Montreal Cognitive Assessment (MoCA) grading system, a randomized controlled study compared the cognitive function of patients receiving WBRT to those receiving HA-WBRT for brain metastases from breast and lung cancers [94]. The results showed significantly higher MoCA scores in the HA-WBRT group [94]. The use of HA-WBRT is expected to grow, as it offers many of the same benefits as WBRT but with fewer side effects. Ongoing trials are further investigating its value in treating brain metastases (NCT03075072) [95].
Despite these advancements, WBRT retains a niche role. It remains valuable for managing microscopic tumours, preventing recurrences, and enhancing the effects of other treatments, such as surgery. A study comparing WBRT combined with SRS to SRS alone found significantly lower recurrence rates and improved overall survival in the combined treatment group [96]. DERGO guidelines also recommend WBRT as an option for patients with 5–10 brain metastases (with a cumulative volume of less than 15 mL) and for those with a limited number of brain metastases (5–10 lesions, cumulative volume < 15 mL) following resection. Additionally, WBRT is advised for patients with multiple symptomatic lesions when hippocampal avoidance is not feasible, demonstrating WBRT’s maintained relevancy in treatment [97].
Systemic Therapies with Clinical Evidence in BCBM
Alongside advancements in radiation techniques, combinations between various systemic therapies and radiation therapies are being explored to optimize patient outcomes. A study assessed irinotecan and temozolomide in 30 patients, nearly all of whom had brain metastases from various breast cancer subtypes. Most of these patients had previously undergone SRS or WBRT and had experienced disease progression. Following the initiation of the drug regimen, only one patient showed further disease progression, and effectiveness was observed across all cancer subtypes [98]. This demonstrates the proven clinical benefit of combining systemic therapies with radiotherapy in BCBM patients.
HER2 + Disease
Treatments targeting HER2 + brain metastases have also been progressing. Tucatinib, for example, was recently studied in combination with trastuzumab and capecitabine. In a trial involving 291 patients with brain metastases, the tucatinib group demonstrated significantly improved survival outcomes (21.6 months versus 12.5 months in the control group treated with placebo, trastuzumab, and capecitabine) [99]. The National Comprehensive Cancer Network guidelines also list this as a preferred treatment regimen for patients previously treated with anti-HER2 drugs [100]. Thus, tucatinib remains a valuable option for difficult-to-target metastases and an important tool for combination therapy.
Trastuzumab-deruxtecan has also been shown to be a highly effective treatment for HER2 + brain metastases. In a population of 15 patients, the drug had a response rate of 73.3% with 13.3% of patients experiencing complete responses and 60% of patients. Additionally, treatment was overall well tolerated, and quality of life was not impaired [101]. These findings suggest that trastuzumab-deruxtecan offers a promising therapeutic option for patients with HER2‑positive BCBM, potentially improving outcomes in this difficult-to-treat population. Furthermore, DESTINY-Breast12, a large prospective clinical trial demonstrated trastuzumab-deruxtecan to have a 12 month progression-free survival of 61.6% for HER2 + with BCBM and low discontinuation rates from adverse events [102]. Further exemplifying the potency of Trastuzumab Deruxtecan, the recent DESTINY-Breast09 Trial demonstrated that Trastuzumab Deruxtecan plus Pertuzumab for HER2 + metastatic breast cancer was superior to the standard first-line therapy of a trastuzumab, pertuzumab, and a taxane (median progression-free of 40.7 vs. 26.9 months) [103]. Although the trial did not explicitly examine intracranial efficacy, they found that progression-free survival benefit was consistent across BCBM patients and state future intent to evaluate intracranial efficacy [103]. Despite the proven potency of trastuzumab, it and other drugs can be improving their ability to penetrate the BBB [104]. To address this challenge, studies are attempting strategies to enhance penetration, including combining trastuzumab with other treatments such as IA NEO100, an agent designed to increase BBB permeability [104]. IA NEO aims to enhance CNS activity reversibly opening the BBB, though further research is needed to assess its use in a clinical environment [104].
Other FDA approved agents for HER2 + BCBM include capecitabine in combination with trastuzumab and tucatinib [105]. This combination is approved for patients with unresectable or metastatic HER2 + disease after failing one line of anti HER2 regimens [105]. This approval was based on the HER2CLIMB trial which found this drug combination to have a progression-free survival of 24.9% at one year compared to 0% of the placebo group in brain metastasis patients [106]. Capecitabine has demonstrated CNS efficacy in the past making it a valuable treatment for BCBM [107]. Capecitabine has also been studied in combination with the drug neratinib compared with lapatinib plus capecitabine in the randomized phase III NALA trial in previously treated HER2 + metastatic breast cancer patients [108]. Subgroup analysis from this trial on BCBM patients revealed neratinib plus capecitabine had a better progression-free survival at 24 months compared to lapatinib plus capecitabine with a mean of 7.8 vs. 5.5 months (HR 0.66, 95% CI 0.41–1.05) [109]. These findings suggest strong CNS efficacy of neratinib along with capecitabine. Another potent treatment for HER2 + BCBM with proven CNS efficacy is trastuzumab emtansine (T-DM1). The KAMILLA trial, a phase IIIb multicenter study evaluated T-DM1 in HER2 + patients with unresponsive advanced or metastatic breast cancer [110]. Subgroup analysis of BCBM patients revealed in 126 patients with measurable BCBM, 42.9% (95% CI 34.1–52.0) achieved a ≥ 30% reduction in lesion size. Ongoing trials such as the TUCATEMEB trial (NCT05673928) are further evaluating tucatinib with T-DM1 in treating HER2 + BCBM as well as other cancers [111]. T-DM1 adds to the multitude of available drugs with CNS efficacy in patients with HER2 + BCBM [110, 112].
ER + Disease
In comparison to HER2+, treatment options for ER + BCBM have been limited. Many anti hormonal drugs have been studied though they face significant challenges as not all of them can cross the BBB [113]. Novel alternative such as selective estrogen receptor degraders (SERDs) including elacestrant may have greater ability to cross the BBB [114]. Elacestrant has been approved in 2023 for advanced metastatic breast cancer in HER2-, ER+, ESR1-mutated patients with resistant disease [115]. This came after multiple phase 1 clinical trials (NCT02650817, NCT02338349) studying elacestrant for advanced breast cancer found antitumor activity in heavily pretreated ER + breast cancer [116, 117]. Despite this, two phase 1 studies in postmenopausal women found low elacestrant concentrations in CSF suggesting the need for more human studies to confirm its efficacy in BCBM patients [114].
Further expanding the use of novel SERDs imlunestrant is another drug of the same class with proven efficacy for ER+, ESR1-mutated patients with advanced breast cancer. In the EMBER-3 trial (NCT04975308), which enrolled 874 with ER-positive HER2- treatment resistant advanced breast cancer, imlunestrant demonstrated significantly greater progression-free survival compared to standard endocrine monotherapy, which consisted of oral exemestane or intramuscular fulvestrant for patients with ESR1 mutations (mean survival time, 2.6 months; 95% CI, 1.2 to 6.9; P < 0.001) [118]. The significance of this benefit did not extend to the overall cohort, representing a limitation in the broader usage of imlunestrant [118].
Imlunestrant also may help address the limitations of treating ER + BCBM due to its ability as a CNS penetrant. In the EMBER-3 trial, there was significantly lower incidence of CNS progression in patients receiving imlunestrant compared to standard therapy in the ESR1 mutated subgroup (1.5% vs. 6.7%, cause-specific hazard ratio, 0.18; 95% CI, 0.04 to 0.90). However, this benefit was not significant in the overall population, and the trial excluded patients with symptomatic or untreated BCBM indicating a greater need for clinical data to determine its efficacy in treating BCBM [118].
Investigational Therapies in BCBM
Studies have explored combining radiotherapy with targeted treatments such as poly-ADP ribose polymerase (PARP) inhibitors like veliparib. A study tested veliparib in a group of 25 breast cancer brain metastasis patients undergoing WBRT and demonstrated a partial or complete response in 41% of patients [119]. However, veliparib’s original results were disappointing, as veliparib failed to significantly improve pathological complete response when added to treatment regimens compared to control group in treatment for TNBC [120]. Nevertheless, some studies remain optimistic, exploring its effectiveness in various combination therapies and pathologies.
Beyond veliparib, other PARPis have shown more promising outcomes. PARPis such as olaparib and talazoparib have been approved for the treatment of metastatic breast cancer in BRCA1 and BRCA2 carriers and have recently demonstrated efficacy in patients with PALB2 mutations [121]. Because PARPis are used in both triple negative and hormone receptor positive breast cancers with germline BRCA1 or BRCA2 mutations, their continued development is particularly valuable. Moreover, PARPis such as olaparib have shown relevant therapeutic levels in the brain, demonstrating promise in penetrating the BBB, a challenge encountered by many therapeutic agents in treating BCBM [122]. Despite this, more clinical evidence is needed to confirm the efficacy of drugs such as olaparib in the brain.
Immunotherapies have increasingly emerged as versatile tools for managing BCBM. Evidence of this can be seen in newly developed drugs targeting programmed death-ligand 1 (PD-L1), including atezolizumab. This drug was tested in a combination therapy study with pertuzumab and trastuzumab for HER2 + breast cancer (NCT03417544) [123, 124]. The clinical benefit rate at 18 weeks was 42.1%, with only 2 out of 19 patients achieving a partial response. PD-L1 inhibitors are still being studied as numerous ongoing studies are investigating its use (NCT06418594) [125]. PD-L1 inhibitors are also used for treatment in TNBC making it potentially an effective therapy for various subtypes of brain metastasis in the future. However, due to the PD-L1 inhibitor’s large molecular size, there are concerns that this drug class may not effectively penetrate the BBB, and further research is warranted for clarification [126]. In parallel, a recent study in mice, portrayed the way in which brain astrocytes can induce overexpression of CDK5 in BCBM, thus encouraging and allowing for outgrowth [127]. CDK5 can suppress MHC-I expression on cancer cells, preventing T-cells from recognising BCBM allowing for the evasion of the immune response, however, studies are needed to evaluate their use clinically [127]. Another novel therapeutic agent, roscovitine, used independently or alongside immune checkpoint inhibitors, showed a significantly reduced BCBM burden, with increased levels of tumour infiltration by T-cells in mice [127]. This highlights the role of CDK5 in immune evasion, as well as the potential for CDK5 inhibitors to be used as a means of restoring immune recognition, as well as improved tumour control [127]. Nonetheless, more evidence is required to evaluate their clinical efficacy.
Another promising drug class is CDK12 inhibitors. CDK12 has been implicated in resistance to anti-HER2 treatments [128]. Several ongoing trials are evaluating the effectiveness of drugs like CT7439 in advanced breast cancer (NCT06600789), offering hope for improved prognoses in cases of resistant metastases [129]. A recent study found that CDK12 was the most frequently rearranged gene in brain metastases from breast cancer, with a significantly higher rearrangement rate in HER2 + cases compared to HER2- ones [130]. This suggests that CDK12 not only plays a critical role in the pathogenesis of BCBM but may also contribute to resistance against anti-HER2 therapies, but more research is needed to assess its clinical utility.
Preclinical and Functional Precision Medicine Approaches
An interesting study of 12 BCBM and their respective primary tumour samples, were used to identify potential treatment targets [131]. Six novel patient-derived xenografts (PDXs) were used as drug screening platforms. The PDXs were treated with a panel of more than 350 drugs [131]. Alterations in the PI3K pathway were reported to be the most predictive for drug efficacy in PDXs [131]. The highest sensitivity was demonstrated to histone deacetylase (HDAC) inhibitors and proteasome inhibitors [131]. It is important to note, that these drugs would not have been identified as they are not on routine NGS sequencing panels, functional drug screening is very important in this individualized approach [131]. This study highlighted the importance of using accurate preclinical models such as PDXs, and the importance of functional drug response assessments in a wide range of targets, to allow for the identification of effective therapies to optimize treatment options for BCBM patients. These xenografts provide valuable preclinical evidence for emerging drug classes and may pave the way for personalized BCBM treatment, although clinical validation is still required. Details of the aforementioned pharmacologic trials are summarized in Table 2.Table 2. Overview of pharmacologic trials evaluated for BCBMStudy Title (NCT)Drug InterventionsPhase(s)BCBM-Specific FindingsReference(s)Phase II study of irinotecan and temozolomide in breast cancer patients with progressing central nervous system disease (NCT00617539)Irinotecan hydrochloride TemozolomidePhase IITwo patients achieved confirmed partial responses in the CNS, while five maintained stable disease for at least 16 weeks.[98]Tucatinib vs Placebo, Both in Combination With Trastuzumab and Capecitabine, for Previously Treated ERBB2 (HER2)-Positive Metastatic Breast Cancer in Patients With Brain Metastases: Updated Exploratory Analysis of the HER2CLIMB Randomized Clinical Trial (NCT02614794)TucatinibCapecitabineTrastuzumabPlaceboPhase IITucatinib, when used alongside trastuzumab and capecitabine, extended median overall survival by 9.1 months in patients with brain metastases and lowered the likelihood of new brain lesions or death as the first event by 45.1% across all participants.[99]Trastuzumab deruxtecan in HER2-positive breast cancer with brain metastases: a single-arm, phase 2 trial (NCT04752059)Trastuzumab deruxtecanPhase IITrastuzumab deruxtecan achieved its primary goal, demonstrating a 73.7% intracranial response rate.[132]A Phase II Study of Atezolizumab, Pertuzumab, and High-Dose Trastuzumab for Central Nervous System Metastases in Patients with HER2-Positive Breast Cancer (NCT03417544)AtezolizumabPertuzumabTrastuzumabPhase IIOut of 19 participants, two experienced a confirmed partial response in the brain, resulting in a CNS overall response rate of 10.5% (90% CI: 1.9%–29.6%). As the trial did not meet its predefined efficacy criteria, it was discontinued early.[123]A Study of T-DXd in Participants With or Without Brain Metastasis Who Have Previously Treated Advanced or Metastatic HER2 Positive Breast Cancer (NCT04739761)Trastuzumab deruxtecanPhase IIITrastuzumab deruxtecan achieved a CNS progression-free survival of 58.9% demonstrating high intracranial activity.[102]Trastuzumab Deruxtecan plus Pertuzumab for HER2-Positive Metastatic Breast Cancer (NCT04784715)Trastuzumab deruxtecanPlaceboTaxanePertuzumabTrastuzumabPhase IIITrastuzumab deruxtecan plus pertuzumab improved first-line progression-free survival (40.7 vs 26.9 months) compared with the standard regimen of taxane, trastuzumab, and pertuzumab in HER2-positive metastatic breast cancer. This benefit was also seen in patients with BCBM.[103]A Study of Tucatinib vs. Placebo in Combination With Capecitabine & Trastuzumab in Patients With Advanced HER2+ Breast Cancer (NCT02614794)TucatinibCapecitabineTrastuzumabPlaceboPhase IIPatients with BCBM had a 24.9% progression free survival with the tucatinib combination vs 0% with the placebo combination (HR 0.48; 95% CI 0.34–0.69; P<0.001).[106]Imlunestrant with or without Abemaciclib in Advanced Breast Cancer (NCT04975308)ImlunestrantExemestaneFulvestrantAbemaciclibPhase IIICumulative incidence of CNS progression was significantly lower in the imlunestrant group compared to standard treatment (1.5% vs 6.7%; hazard ratio 0.18, 95% CI 0.04–0.90 in ESR1-mutated).However, this benefit was only significant in the ESR1-mutated subgroup. (1.6% vs 3%; hazard ratio, 0.47; 95% CI, 0.16 to 1.38 in overall population)[118]A Study of Neratinib Plus Capecitabine Versus Lapatinib Plus Capecitabine in Patients With HER2+ Metastatic Breast Cancer Who Have Received Two or More Prior HER2 Directed Regimens in the Metastatic Setting (NCT01808573)NeratinibCapecitabineLapatinibPhase IIIIn 101 patients with CNS metastases, median PFS was 7.8 months with neratinib with capecitabine vs 5.5 months with lapatinib with capecitabine; intracranial objective response rate was 26.3% vs 15.4%, respectively.[108, 109]A Study of Trastuzumab Emtansine in Participants With Human Epidermal Growth Factor Receptor 2 (HER2)-Positive Breast Cancer Who Have Received Prior Anti-HER2 And Chemotherapy-based Treatment (NCT01702571)TrastuzumabEmtansinePhase IIIAmong all patients with BCBM (n = 398), median PFS was 5.5 months (95% CI 5.3–5.6) and median OS was 18.9 months (95% CI 17.1–21.3). In those with measurable BCBM (n=126), 42.9% (95% CI 34.1–52.0) achieved a ≥30% reduction in lesion size. [110, 112]A Phase II Study of Tucatinib and Ado-trastuzumab Emtansine (T-DM1) in Patients With HER2-positive Metastatic Solid Tumours and Metastases to Brain (NCT05673928)Trastuzumab emtansineTucatinibPhase IIRecruiting [111]Adebrelimab Plus Apatinib and Etoposide for the Treatment of HER2-Negative Breast Cancer Brain Metastasis (NCT06418594)AdebrelimabApatinibEtoposidePhase IIRecruiting[125]A Modular Phase 1/2 Study with CT7439 in Participants with Solid Malignancies (including advanced breast cancer) (NCT06600789)CT7439Phase I/IIRecruiting[129]
Future Directions
Future directions in BCBM research increasingly incorporate developments in computational science and cancer neuroscience. These approaches are being explored to deepen understanding of disease mechanisms and improve clinical decision making.
Machine Learning
Machine learning (ML) is garnering increasing attention for its potential to improve prognostication, treatment planning, and diagnosis in patients with BCBMs.
Initial ML applications as prognostic measures in BCBM involved the generation of models to predict survival. Li et al. utilized the clinical features of BCBM patients, from the Surveillance, Epidemiology, and End Results (SEER) database (2010–2019), to generate an XGBoost model capable of predicting survival. Impressive results were observed, particularly in forecasting 3-year survival on external datasets with an AUC of 0.936 [133]. This model allowed for further identification of underlying trends such as the added survival benefit of surgical intervention in HER2 + and HR-/HER2- subtypes of patients with BCBM and lack of benefit in the HR+/HER2- subtype [133].
More advanced applications in prognostication have included the utilization of AI to predict breast cancers with metastatic potential. The value of AI in this context has recently been demonstrated by Tan et al., in the development of an AI model utilizing clinical blood markers and ultrasound data to predict distant metastasis in patients with breast cancer [134]. Although this LightGBM model did not include analysis on brain metastases, the results of the combined model on external datasets were encouraging with an AUC of 0.918 [134]. In addition, the analysis of features utilized by the model allows further insight into biochemistry markers previously queried for their role in metastatic cancer. Such is seen in the exploration of CK-MB and CA153, which were highlighted as key features of their model, substantiating previous studies into their prognostic value [134]. A similar model was developed by Shiner et al., which encompassed brain metastases and displayed prominent levels of accuracy [135].
ML has been employed to detect BCBMs on imaging to automate and enhance diagnostics. Grovik et al. utilized a deep learning algorithm based on a convolutional neural network to analyze multisequence MRIs and effectively detect the presence of metastases as well as segment individual growths [136]. Similarly, Ziyaee produced a deep-learning model with high positive predictive value in delineating metastatic margins on MRI, a key aspect of treatment planning [137]. Interestingly, 9% of false-positives in this population were in fact true-positives missed on initial review and labelling, which highlights the power of this model to enhance early detection [137].
The field of radiomics is an emerging application of advanced ML capabilities in radiology. Although perfusion and permeability imaging have taken strides towards quantitative imagining, radiomics accesses pixel-level relationships and image features such as texture and morphology to draw conclusions [138]. Nowakowski et al. have summarized the diverse array of radiomic applications specific to brain metastases, including the prediction of response to stereotactic radiosurgery, differentiating radiation necrosis from local recurrence/progression, predicting mutation status, differentiating between primary and metastatic tumors, and lastly predicting the primary cancer site in the case of metastasis [139]. The breadth of information delivered by radiomic models may function as a form of virtual biopsy in research settings, with the potential to provide non-invasive support for patient stratification, treatment planning and detection of coexisting pathology in the future.
The application of ML in neuro-oncology holds immense promise, yet this enthusiasm must be tempered by a recognition of its current limitations. The NEVER study, which assessed publication bias in radiomics research, identified several key weaknesses that contribute to the growing disconnect between ML studies and their clinical translation [140]. Among these are the predominance of retrospective study designs (95%), reliance on private datasets (91%), single-institution settings (75%), and a lack of external validation (81%) [140]. With regards to BCBMs specifically, there is a particular scarcity of prospective literature, although integration of ML into brain metastasis clinical workflows has been initiated. Such an example can be seen in VBrain, an FDA-cleared deep learning model constructed for the diagnosis and segmentation of metastatic brain tumours [141]. Furthermore, many ML studies fail to compare their models to established diagnostic standards, making it difficult to assess their real-world utility [140]. Variability in ML methodologies further undermines reproducibility and raises concerns about the generalizability of these models across diverse populations [140]. A practical roadmap to overcome these challenges could include the utilization of common data elements (CDEs), as well as the establishment of multi-centre validation consortia. Past reviews have demonstrated how variations in segmentation as well as the application of external validation can augment the diagnostic accuracy of radiomic models [142]. CDEs may be applied in this context to not only standardize feature definitions and formats, but to harmonize segmentation protocols to ensure reproducibility. Shared validation data across institutions should afford models a wealth of heterogenous data to mimic a real-world landscape and improve generalizability. Establishing external validation as a consistent requirement is essential to narrowing the gap between academic literature and clinical practice. Such efforts could lay the groundwork for the prospective use of ML models and accelerate their integration into precision medicine.
Cancer Neuroscience in BCBM
Breast cancer cells that enter the cerebral circulation must first engage and remodel the blood brain barrier. They influence endothelial cells, pericytes, and astrocytic end feet to loosen tight junctions and allow their arrest and passage into the parenchyma. Enzymes and transporters such as ENPP1 and molecular pathways that regulate endothelial permeability have been identified as key mediators of this early step [143, 144]. Once within the brain tissue, metastatic cells must survive a highly specialized environment. They adapt by exploiting local trophic signals and by adopting features of neuronal physiology, a process often described as neuronal mimicry. Evidence from patient samples and preclinical models demonstrates that these cells can utilize gamma aminobutyric acid as a metabolic substrate, expressing the associated transporters and enzymes, and in some cases forming pseudo synaptic contacts with neurons that allow access to neurotransmitter related nutrients [145]. Similar interactions have been observed with glutamatergic neurons, where tumour cells display sensitivity to N methyl D aspartate (NMDA) receptor signalling and may exploit neuronal firing to enhance their own proliferation [146].
Astrocytes emerge as critical partners in this process. Direct physical connections such as gap junctions allow the exchange of small molecules and microRNAs that reprogram astrocytes toward a tumour supportive phenotype, increasing the resistance of cancer cells to stress and therapy. Astrocyte derived signals can also activate cyclin dependent kinase 5 in tumour cells, promoting invasion [147]. This supportive microenvironment is further shaped by microglia, which respond to disseminated tumour cells with a range of programs. Although they can mount antitumor responses characterized by antigen presentation and pro inflammatory activity, microglia also release cytokines such as interleukin six and C-C motif chemokine ligand two that enhance tumour cell survival and motility [148]. Reprogramming microglia toward a sustained antitumor phenotype in experimental systems suppresses metastatic growth, highlighting their therapeutic potential.
Communication between tumour and brain cells is not limited to direct contact. Breast cancer cells with a propensity for brain colonization release extracellular vesicles carrying microRNAs that alter neuronal and astrocytic metabolism. For example, miR 199b 5p targets solute carrier transporters, leading to glutamate accumulation in the extracellular space, which in turn fuels tumour growth [149]. Other microRNAs have been linked to disruption of barrier integrity and modulation of the immune and glial landscape, suggesting their role as both biomarkers and therapeutic targets.
The interplay between tumour biology and the neural microenvironment varies by breast cancer subtype. HER2 + and triple negative disease have the highest rates of brain involvement, and their respective tumour cells exhibit distinct strategies for barrier interaction, neuronal mimicry, and reliance on glial support [144]. These biological differences influence drug penetration and treatment response, reinforcing the need for approaches that target neuron like signalling and glial contributions in addition to conventional local and systemic therapies.
Emerging work now connects barrier remodelling, neural circuit activity, astrocyte and microglia state changes, and vesicle mediated communication into a unified model of metastatic growth in the brain [143–149]. Future research priorities include mapping the specific neural circuits that promote tumour expansion in each subtype, charting the dynamic states of astrocytes and microglia in patients, and developing interventions that interrupt synaptic like signalling or restore the protective functions of the barrier and resident immune cells. Such advances may provide the mechanistic basis for therapies that complement current surgery, radiotherapy, and systemic treatment to more effectively control brain metastases in breast cancer.
Limitations
This paper is a literature review, which brings several important limitations. A review depends on the quality and consistency of the published work it draws from. Many of the available studies on BCBM are small, retrospective, or based on experimental laboratory models. This means the findings may not fully reflect outcomes in broader patient groups. Some of the biological pathways and diagnostic methods discussed have only been tested in early research settings and are not yet supported by large clinical studies. In addition, new tools such as liquid biopsy, spatial transcriptomics, radiomics and machine learning vary widely in their methods and have limited evaluation in real world clinical care. Research on receptor changes in brain metastases is also limited because brain tissue samples are difficult to obtain. These factors mean that the conclusions of this review should be interpreted with caution. More large and carefully designed clinical studies are needed to confirm how these emerging approaches can be used in the management of BCBM.
Conclusion
Future progress in BCBM will likely involve a coordinated approach that unites advances in computational science with deeper exploration of cancer neuroscience. Priorities include the standardization of spatial transcriptomics protocols specific to this disease to allow reproducible mapping of tumour-microenvironment interactions, the creation of multi-institutional consortia to externally validate radiomic and other ML models for clinical applicability, and the launch of prospective trials to determine the survival impact of receptor reassessment. Equally important is the continued investigation of neural circuit involvement, glial cell dynamics, and vesicle-mediated signalling as therapeutic targets, supported by functional drug screening in patient-derived models. Achieving these aims may help translate molecular, imaging, and neurobiological insights into precision strategies that can improve outcomes in this challenging patient population.
Key References
- Jagust P, Powell AM, Ola M, Watson L, de Pablos-Aragoneses A, García-Gómez P, et al. RET overexpression leads to increased brain metastatic competency in luminal breast cancer. J Natl Cancer Inst. 2024;116(10):1632-44.
- ○ Identified RET overexpression as a driver of oestrogen receptor positive breast cancer growth in the brain, supporting RET inhibition as a potential treatment.
- Hulsbergen AFC, Claes A, Kavouridis VK, Ansaripour A, Nogarede C, Hughes ME, et al. Subtype switching in breast cancer brain metastases: a multicenter analysis. Neuro Oncol. 2020;22(8):1173-81.
- ○ It provides essential insight by demonstrating subtype switching and receptor discordance in breast cancer brain metastases, directly informing prognosis and highlighting the need for receptor reassessment to optimize treatment decisions.
- Vogelbaum MA, Brown PD, Messersmith H, Brastianos PK, Burri S, Cahill D, et al. Treatment for brain metastases: ASCO-SNO-ASTRO guideline. Oxford University Press US; 2022.
- ○ This guideline provides evidence-based recommendations for the treatment of brain metastases, offering clear guidance on surgery, radiosurgery, and radiation therapy in different clinical scenarios.
- Lin NU, Murthy RK, Abramson V, Anders C, Bachelot T, Bedard PL, et al. Tucatinib vs placebo, both in combination with trastuzumab and capecitabine, for previously treated ERBB2 (HER2)-positive metastatic breast cancer in patients with brain metastases: updated exploratory analysis of the HER2CLIMB randomized clinical trial. JAMA oncology. 2023;9(2):197-205.
- ○ This study provides strong clinical evidence that tucatinib can extend survival in patients with HER2 positive metastatic breast cancer and brain metastases, addressing a group with limited effective treatment options.
- Bartsch R, Berghoff AS, Furtner J, Marhold M, Bergen ES, Roider-Schur S, et al. Final outcome analysis from the phase II TUXEDO-1 trial of trastuzumab-deruxtecan in HER2-positive breast cancer patients with active brain metastases. Neuro-oncology. 2024;26(12):2305-15.
- ○ This study demonstrates that trastuzumab deruxtecan provides durable disease control in patients with active HER2 positive breast cancer brain metastases, supporting its role as an effective treatment option.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A Phase 1 Study of MOMA-313 Given as Monotherapy or in Combination With a PARP Inhibitor in Participants With Advanced or Metastatic Solid Tumors [Internet]. 2024. Available from: https://clinicaltrials.gov/study/NCT 06545942
- 2Phase A. 1/2a, Multi-Center, Open-Label Study to Evaluate the Safety, Tolerability, Pharmacokinetics, and Preliminary Evidence of Antitumor Activity of JAB-2485 in Adult Patients With Advanced Solid Tumors [Internet]. 2022. Available from: https://clinicaltrials.gov/study/NCT 05490472
- 3Phase A. II Clinical Trial to Investigate ARID 1A Mutation and CXCL 13 Expression in the Pre-Treatment Tumor Samples as a Combinatorial Predictive Biomarker for Immune Checkpoint Therapy in Metastatic Solid Tumors [Internet]. 2021. Available from: https://clinicaltrials.gov/study/NCT 04957615
- 4Open-label. Multicentre, Phase Ib Dose-escalation Study of MEN 1611, a PI 3K Inhibitor Combined With Trastuzumab With or Without Fulvestrant, in Subjects With PIK 3CA Mutated HER 2 Positive Locally Recurrent Unresectable (Advanced) or Metastatic (a/m) Breast Cancer Progressed to Anti-HER 2 Based Therapy [Internet]. 2018. Available from: https://clinicaltrials.gov/study/NCT 03767335
- 5Phase II Study for Patients With Advanced Triple Negative or Metaplastic HR-positive/HER 2-negative, PIK 3CA/PTEN-altered Breast Cancer Treated With Eribulin in Combination With MEN 1611 [Internet]. 2023. Available from: https://clinicaltrials.gov/study/NCT 05810870
- 6Phase 1b/2, Multicenter, Open-label, Dose-Expansion Modular Study To Explore the Safety, Tolerability, and Anti-tumor Activity of HER 3- D Xd Monotherapy and Combinations in Patients With Inoperable Advanced Breast Cancer (ABC) After Progression on T-D Xd [Internet]. 2024. Available from: https://clinicaltrials.gov/study/NCT 06298084
- 7HERTHENA-Pan Tumor 01 (U 31402-277): A Phase 2, Multicenter, Multicohort, Open-Label, Proof of Concept Study of Patritumab Deruxtecan (HER 3-D Xd; U 3-1402) in Subjects With Locally Advanced or Metastatic Solid Tumors [Internet]. 2023. Available from: https://clinicaltrials.gov/study/NCT 06172478
- 8A Phase I Ia Study of Dendritic Cell Vaccines Against Her 2/Her 3 and Pembrolizumab in Patients With Asymptomatic Brain Metastasis From Triple Negative Breast Cancer (TNBC) or HER 2 + Breast Cancer (HER 2 + BC) or Hormone Receptor Positive (HR+) Breast Cancer [Internet]. 2020. Available from: https://clinicaltrials.gov/study/NCT 04348747