Heat therapy for primary dysmenorrhea: a systematic review and meta-analysis
Dongni Yuan, Yunyu Liu, Ziyi Chen, Zhuoya Hu, Xingxian Li, Wanyi Zhang, Kexin Mao, Wenbin Ma, Lei Lan

TL;DR
Heat therapy may be as effective as NSAIDs for treating menstrual pain and has fewer side effects.
Contribution
A systematic review and meta-analysis evaluating heat therapy's efficacy and safety for primary dysmenorrhea.
Findings
Heat therapy reduces pain intensity more than no treatment during both prevention and acute treatment.
Heat therapy may provide comparable or slightly better pain relief than NSAIDs with fewer adverse effects.
Abstract
Primary dysmenorrhea is highly prevalent and often suboptimally managed, as non-steroidal anti-inflammatory drugs (NSAIDs) fail to provide analgesia in 18% of women. This review therefore aims to evaluate the efficacy and safety of heat therapy—a widely used self-care method—for both preventing and acutely treating primary dysmenorrhea. We searched seven databases (CENTRAL, PubMed, Web of Science, EMBASE, CNKI, VIP, Wanfang) from inception to October 28, 2024 and updated to August 03, 2025. Pairs of reviewers independently screened records, extracted data, and assessed risk of bias using a modified Cochrane RoB 1.0 tool. Random-effects meta-analyses were performed for pain intensity (converted to 10-cm VAS) and adverse events. Evidence certainty was graded via GRADE (Grading of Recommendations, Assessment, Development, and Evaluations). We screened 2,733 citations and included 57 RCTs…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
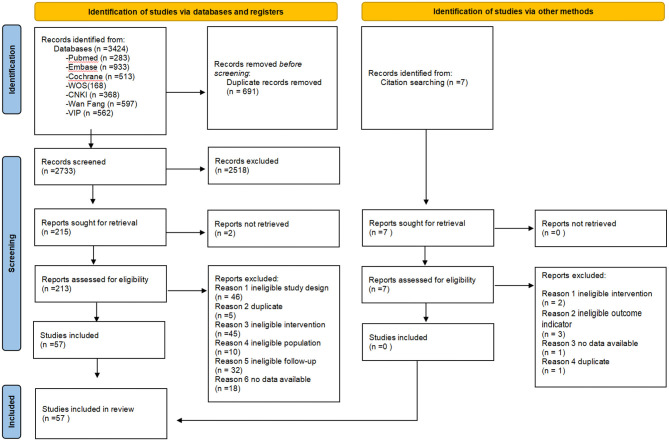 Figure 1
Figure 1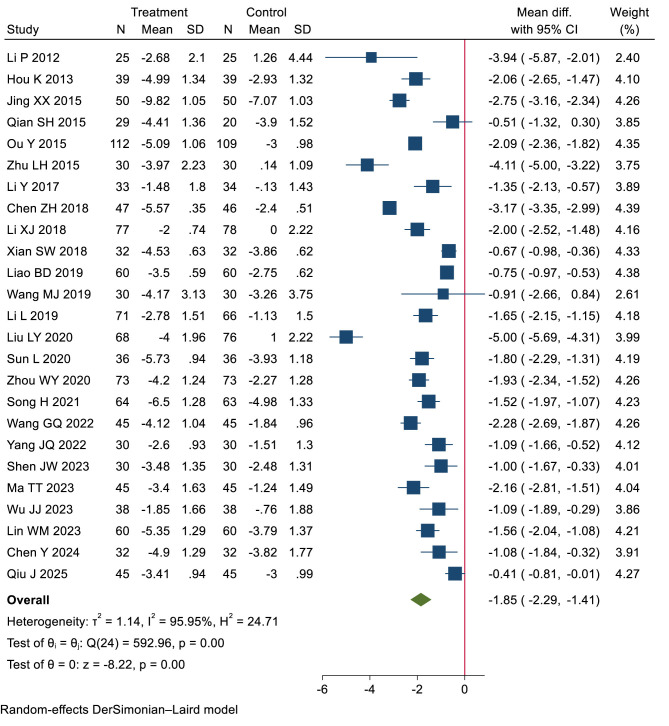 Figure 2
Figure 2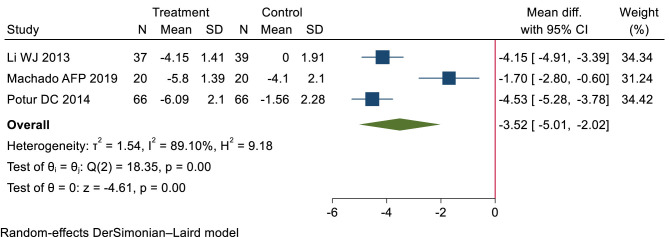 Figure 3
Figure 3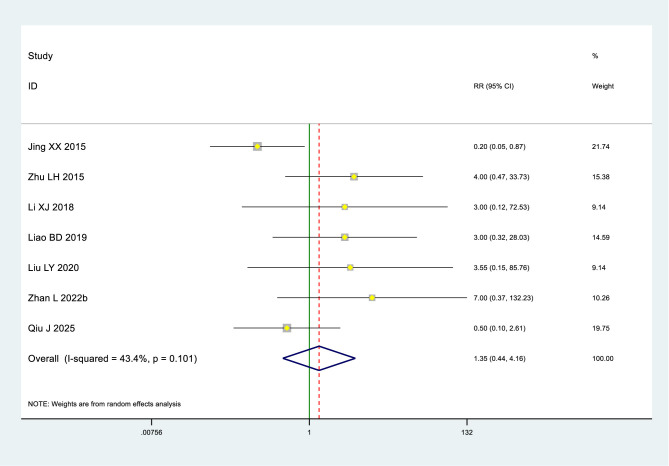 Figure 4
Figure 4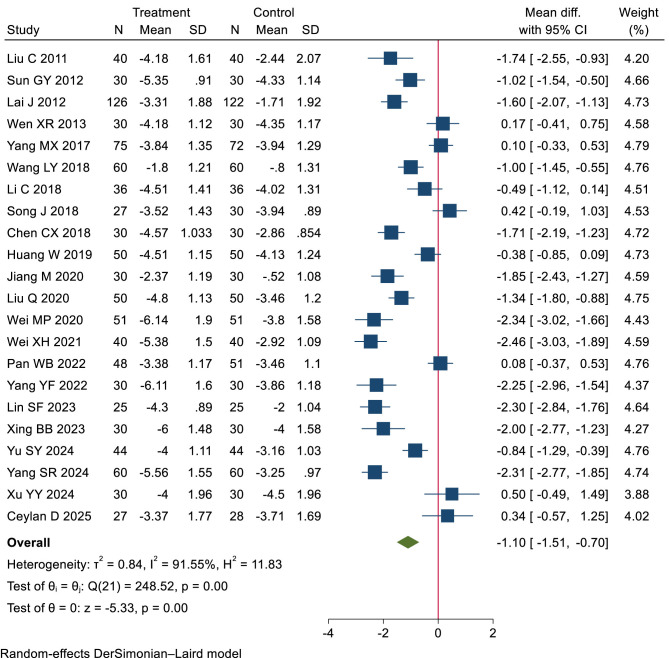 Figure 5
Figure 5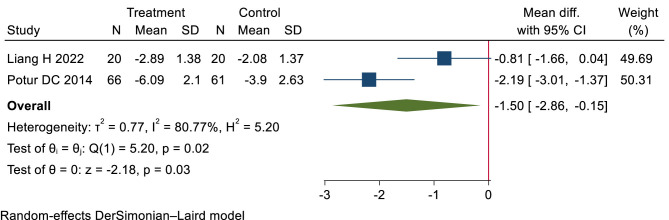 Figure 6
Figure 6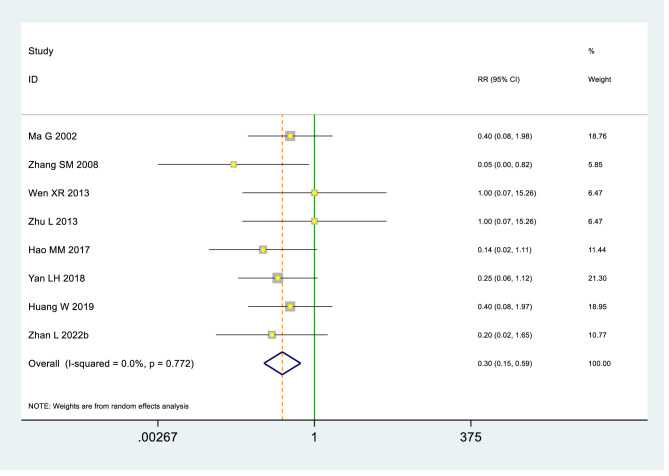 Figure 7
Figure 7|
|
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|---|---|
| Ma G 2002 ( | Microwave therapy | Ibuprofen | NR | China | 120 | 90 | 24 (4.23) | 19 (2.73) |
| Zhang SM 2008 ( | TDP & Moxi | Indometacin | NR | China | 98 | 90 | 46.76(NR) | 19.2 (NR) |
| Liu C 2011 ( | Moxi | Ibuprofen | NR | China | 80 | 90 | 68.2 (35.69) | 21.22 (5.86) |
| Sun GY 2012 ( | Moxi & Usual care | Ibuprofen & Usual care | NR | China | 60 | 90 | 60 (NR) | 23 (NR) |
| Lai J 2012 ( | Super Lizer | Indometacin | NR | China | 248 | 90 | 41.3 (17.02) | 17.7 (2.25) |
| Li P 2012 ( | Moxi | Blank | NR | China | 50 | 90 | 74.6 (32.09) | 21.9 (1.92) |
| Hou K 2013 ( | Moxi & NSAID | NSAID | NR | China | 78 | 90 | NR | 25.6(NR) |
| Li WJ 2013 ( | Moxi | Blank | NR | China | 76 | 20 min | NR | NR |
| Wen XR 2013 ( | Moxi | Ibuprofen | NR | China | 60 | 90 | 73.2 (36.6) | 22.3 (2.53) |
| Zhu L 2013 ( | Moxi & Acupuncture | Acupuncture | NR | China | 60 | 90 | 72.7 (35.93) | 22.3 (2.53) |
| Potur DC 2014 ( | Hot post | NSAID or Blank | Government | Turkey | 252 | 8h | NR | 59.62 (1.18) |
| Jing XX 2015 ( | Moxi & Ibuprofen | Ibuprofen | NR | China | 100 | 90 | 27 (3.1) | 22.2 (2.14) |
| Qian SH 2015 ( | RDP & Point application theropy | Point application therapy | NR | China | 52 | 90 | 41.3 (28.74) | 21 (3.96) |
| Ou Y 2015 ( | Moxi & TCM | TCM | NR | China | 221 | 120 | 36 (NR) | 21.2 (NR) |
| Zhu LH 2015 ( | Moxi | Blank | Government | China | 64 | 90 | 59.6 (20.25) | 20.3 (1.6) |
| Li Y 2017 ( | Moxi & Usual care | Usual care | Government | China | 70 | 90 | 25.5 (12.58) | 20.3 (1.05) |
| Yang MX 2017 ( | Moxi | Ibuprofen | Government | China | 152 | 90 | NR | 23 (2.92) |
| Hao MM 2017 ( | Moxi | Painkiller | NR | China | 80 | 90 | NR | 19.7 (NR) |
| Wang LY 2018 ( | Moxi | Ibuprofen | NR | China | 120 | 90 | 78.5 (39.76) | 22.3 (2.63) |
| Chen ZH 2018 ( | Moxi & Acupuncture | Acupuncture | NR | China | 93 | 120 | 27.2 (14.23) | 22.8 (3.1) |
| Li C 2018 ( | Moxi | Ibuprofen | NR | China | 72 | 90 | 54.7 (41.75) | 23 (1.42) |
| Li XJ 2018 ( | Moxi | Blank | Government | China | 155 | 90 | 57 (5.39) | 20 (0.5) |
| Song J 2018 ( | Moxi | Ibuprofen | NR | China | 60 | 90 | 60.1 (27.77) | 23.6 (3.44) |
| Xian SW 2018 ( | Moxi & Acupuncture | Acupuncture | Government | China | 64 | 180 | 37.9 (32.13) | 20.6 (1.42) |
| Yan LH 2018 ( | Moxi & Ibuprofen | Ibuprofen | NR | China | 106 | 90 | 5.4 (0.6) | 24.7 (4.64) |
| Chen CX 2018 ( | Moxi & Ibuprofen | Ibuprofen | Government | China | 60 | 120 | 17.5 (7.05) | 20.3 (1.62) |
| Machado AFP 2019 ( | Thermal therapy & TENS | TENS | NR | Brazil | 44 | 24 h | NR | 22.6 (4.08) |
| Wang MJ 2019 ( | Moxi & TCM | TCM | NR | China | 60 | 90 | NR | 24.4 (NR) |
| Huang W 2019 ( | Moxi | Ibuprofen | Government | China | 100 | 90 | 36.8 (22.82) | 20.4 (1.6) |
| Li L 2019 ( | Moxi & Usual care | Usual care | NR | China | 150 | 90 | NR | NR |
| Liao BD 2019 ( | Moxi & Needle warming Moxi | Needle warming Moxi | NR | China | 120 | 120 | NR | 24 (3) |
| Jiang M 2020 ( | Moxi | Ibuprofen | Government | China | 60 | 90 | 30.4 (4.42) | 22.2 (4.03) |
| Liu Q 2020 ( | Moxi | Ibuprofen | Government | China | 100 | 90 | 48.2 (14.42) | 26.3 (4.98) |
| Liu LY 2020 ( | Moxi | Blank | Government | China | 144 | 90 | 54 (6.8) | 20 (0.5) |
| Sun L 2020 ( | Moxi & TCM | TCM | NR | China | 72 | 90 | 68 (27.45) | 26 (3.75) |
| Wei MP 2020 ( | Moxi | Ibuprofen | NR | China | 102 | 90 | 23.4 (7.04) | 20.1 (2.34) |
| Zhou WY 2020 ( | Moxi & TCM | TCM | NR | China | 146 | 90 | 38.6 (13.01) | 26.7 (1.87) |
| Song H 2021 ( | Moxi & Acupuncture and cupping | Acupuncture and cupping | NR | China | 127 | 90 | NR | 22.2 (2.88) |
| Wei XH 2021 ( | Moxi | Ibuprofen | NR | China | 80 | 90 | 32.9 (13.53) | 20.4 (1.83) |
| Pan WB 2022 ( | Moxi | Ibuprofen | Government | China | 99 | 90 | 39.5 (18.83) | NR |
| Wang GQ 2022 ( | Moxi & TCM | TCM | NR | China | 90 | 90 | 23.4 (7.33) | 21 (2.62) |
| Liang H 2022 ( | Electromagnetic wave | Ibuprofen | NR | China | 40 | 30 min | 34 (4.73) | 19.2 (1.02) |
| Yang JQ 2022 ( | Moxi & TCM | TCM | NR | China | 62 | 90 | 86.7 (35.72) | 27 (3.04) |
| Yang YF 2022 ( | Moxi | Ibuprofen | NR | China | 60 | 90 | 47.6 (5.23) | 35 (5.19) |
| Zhan L 2022 ( | Moxi | Ibuprofen | NR | China | 104 | 90 | 19.1 (14.58) | 23.4 (2.77) |
| Shen JW 2023 ( | Moxi patch & TCM | TCM | Government | China | 60 | 90 | 49.2 (22.86) | 29.4 (4.14) |
| Lin SF 2023 ( | TDP & Moxi | Indometacin | NR | China | 50 | 90 | NR | 18.1 (3.5) |
| Ma TT 2023 ( | Moxi patch & TCM | TCM | NR | China | 90 | 180 | 58.8 (39.49) | 27.6 (5.32) |
| Wu JJ 2023 ( | Moxi & Usual care | Usual care | Government | China | 76 | 90 | NR | 22 (2.48) |
| Lin WM 2023 ( | Moxi | Ibuprofen | Government | China | 120 | 90 | 80.8 (38.49) | 24.9 (6.05) |
| Xing BB 2023 ( | Moxi | Ibuprofen | NR | China | 66 | 90 | 81 (32.28) | 25.2 (2.56) |
| Yu SY 2024 ( | Moxi patch & TCM | TCM | NR | China | 88 | 90 | 12.5 (3.4) | 26.4 (3.26) |
| Yang SR 2024 ( | Moxi | Ibuprofen | Government | China | 120 | 90 | 84 (NR) | 26.3 (NR) |
| Xu YY 2024 ( | Moxi | Ibuprofen | NR | China | 68 | 90 | 142 (77.94) | 29.4 (6.49) |
| Chen Y 2024 ( | Moxi & Acupuncture | Acupuncture | NR | China | 64 | 90 | 10.1 (8.33) | 25.1 (4.02) |
| Qiu J 2025 ( | Moxi & catgut embedding | Catgut embedding | Government | China | 90 | 90 | 8.4 (1.74) | 23.4 (2.6) |
| Ceylan D 2025 ( | Thermal therapy | Dexketoprofen trometamol | Government | Turkey | 56 | 90 | NR | NR |
|
|
|
|
|
|
|---|---|---|---|---|
| Heat vs. blank control | Pain relief (VAS, cm) | ≥3 months | Low | Superior to control (WMD −1.85 cm, 95% CI: −2.29 to −1.41) |
| Pain relief (VAS, cm) | ≤24 h | Low | Superior to control (WMD −3.52 cm, 95% CI: −5.01 to −2.02) | |
| Adverse effects | Various | Low | Little to no difference (RR 1.34, 95% CI: 0.44 to 4.16) | |
| Heat vs. NSAIDs | Pain relief (VAS, cm) | ≥3 months 24 h | Low | Similar efficacy (WMD −1.10 cm, 95% CI: −1.51 to −0.70) |
| Pain relief (VAS, cm) | ≤24 h | Low | Similar efficacy (WMD −1.5 cm, 95% CI: −2.86 to −0.15) | |
| Adverse effects | Various | Moderate | Safer than NSAIDs (RR 0.3, 95% CI: 0.15 to 0.59) |
|
|
|
|
|
|
|
|
|
| |
|---|---|---|---|---|---|---|---|---|---|
| 25 (2,393) | Seriousa | Not seriousb, I2=95.95% | Not serious | Not serious | Seriousc | Achieved at or above MID | |||
| Heat 98% | Control 77% | Low | |||||||
| Modeled RD 21% (19%, 22%) | |||||||||
| WMD −1.85 (−2.29, −1.41) | |||||||||
| 3 (248) | Seriousa | Not seriousb, | Not serious | Seriousd | NA | Achieved at or above MID | Low | ||
| Heat 96% | Control 51% | ||||||||
| Modeled RD 45% (33%, 48%) | |||||||||
| WMD −3.52 (−5.01, −2.02) | |||||||||
|
| |||||||||
| 7 (784) | Seriousa | Not serious, | Not serious | Seriouse | NA | RR 1.35 (0.44, 4.16) | Low | ||
|
|
|
|
|
|
|
|
|
| |
|---|---|---|---|---|---|---|---|---|---|
| 22 (1,938) | Seriousa | Not seriousb, | Not serious | Not serious | Seriousc | Achieved at or above MID | |||
| Heat 100% | Control 96% | Low | |||||||
| Modeled RD 4% (3%, 4%) | |||||||||
| WMD −1.10 (−1.51, −0.70) | |||||||||
| 2 (167) | Seriousd | Not seriouse, | Not serious | Seriousf | NA | Achieved at or above MI | Low | ||
| Heat 93% | Control 77% | ||||||||
| Modeled RD 16% (2%, 21%) | |||||||||
| WMD −1.50 (−2.86, −0.15) | |||||||||
|
| |||||||||
| 8 (728) | Seriousa | Not serious, | Not serious | Not serious | NA | RR 0.30 (0.15, 0.59) | Moderate | ||
- —Sichuan Provincial Science and Technology Support Program10.13039/100012542
- —Chengdu University of Traditional Chinese Medicine University-Institute Joint Innovation Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMenstrual Health and Disorders · Menopause: Health Impacts and Treatments · Thermoregulation and physiological responses
Introduction
1
Primary dysmenorrhea is a pervasive yet frequently overlooked public health issue, affecting up to 90% of reproductive-aged women worldwide (1). It is defined as painful menstrual cramps in the absence of pelvic pathology (2). The repercussions are substantial, with severe symptoms leading to activity restriction and absenteeism from work or school in up to 15% of affected women, underscoring its considerable socioeconomic burden (3, 4).
Research indicates that women with dysmenorrhea have elevated levels of prostaglandins, a hormone known to cause crampy abdominal pain. NSAIDs are medications that work by blocking the production of prostaglandins (5). NSAIDs are effective for treating dysmenorrhea, as demonstrated by a meta-analysis of 35 randomized controlled trials (5). However, a review of 51 different clinical trials found that 18% of women reported little to no relief from menstrual pain with NSAIDs (6). And NSAIDs carry a range of adverse effects, primarily affecting the gastrointestinal, renal, and cardiovascular systems (7). Given these limitations, non-pharmacological alternatives are increasingly sought.
A diverse range of non-pharmacological interventions exists, including dietary supplements, transcutaneous electrical nerve stimulation (TENS), acupuncture, and exercise (8–11). Among these options, thermal therapy stands out by enabling self-care for patients, offering a superior safety profile, and demonstrating high accessibility and public acceptance. The rationale for focusing on heat is 2-fold. First, it aligns with the prostaglandin-based pathophysiology of dysmenorrhea; applied heat increases pelvic blood flow, which may help to dissipate and reduce the concentration of prostaglandins, thereby relieving ischemia and muscle cramps (12). Second, it offers a unique combination of immediate, non-invasive analgesia and an exceptional safety profile, presenting a practical and accessible option for women seeking to avoid medication-related side effects (13). Therefore, we posit that thermal therapy represents a promising and strategic non-pharmacological approach worthy of in-depth study.
Methods
2
Literature search
2.1
An academic librarian systematically designed and executed comprehensive, database-specific search strategies for seven major biomedical databases: Cochrane Central Register of Controlled Trials (CENTRAL), PubMed, Web of Science, EMBASE, Chinese National Knowledge Infrastructure (CNKI), VIP Database for Chinese Technical Periodicals, and Wanfang Data. Our systematic search encompassed all available records from each database's inception through October 28, 2024 and updated to August 03, 2025, without imposing language or publication status limitations. We also searched the previous systematic reviews and screened the reference lists and the studies included (Supplementary Table 1).
Study selection
2.2
Pairs of reviewers (HZY, LXX, CZY, ZWY) independently screened titles, abstracts, and subsequently, the full texts of potentially eligible articles using standardized, pre-tested forms. The data extraction form was structured around the PICOS framework, covering participant characteristics (Population), detailed descriptions of the interventions and comparators (Intervention/Comparison), study design (Study), outcome measures (Outcome), along with risk of bias assessments and records of adverse effects (see Supplementary File 1).
Disagreements primarily concerned the applicability of the interventions or the certainty of outcome reporting in the full-text articles assessed. All disagreements were referred to the arbitrator (YDN). The arbitrator made the final decision by referring to the predetermined inclusion criteria outlined in the PICOS framework and based on the original article text.
We included trials that met the following criteria: (1) enrolled patients diagnosed with primary dysmenorrhea; (2) randomized participants to receive localized superficial heat therapy, defined as the application of any device or substance (e.g., electric heating pads, adhesive abdominal warmers, far-infrared belts, or moxibustion) aimed at transferring thermal energy continuously to the body, vs. a control (no treatment, placebo, or NSAIDs); (3) evaluated outcomes either in the immediate term (≤24 h) or analgesic effect or over the longer term (≥3 months) for repeated-use efficacy; and (4) reported measures of pain intensity or safety endpoints.
Data abstraction and risk of bias assessment
2.3
Four reviewers (YDN, LYY, HZY, CZY) extracted data from each eligible trial sequentially, ensuring they faced away from each other during the process. We gathered information on study characteristics, including author name, year of publication, study location, funding source, sample size, and length of follow-up, as well as intervention characteristics and all patient-important outcomes.
In cases where a study reported outcomes at multiple time points, we selected the most commonly reported follow-up period among the eligible trials. To account for within-person variability, we abstracted change scores from baseline; end scores were used only when change scores were not available. Additionally, when multiple instruments or questionnaires were employed to measure a common outcome (such as pain), we abstracted data solely for the most frequently used instrument across the eligible studies.
Three reviewers (HZY, LYY, CZY) independently assessed the risk of bias using a modified Cochrane Risk of Bias Tool 1.0 (14, 15). The tool assessed the following domains: random sequence generation; allocation concealment; blinding of study participants, healthcare providers, and outcome assessors; incomplete outcome data (≥20% missing data was considered high risk of bias); and other potential sources of bias. For each item, responses were scored as “definitely or probably yes” (low risk of bias) or “definitely or probably no” (high risk of bias). Disagreements between reviewers were resolved through discussion and, if necessary, by third-party adjudication (see Supplementary Table 2).
Data synthesis
2.4
For dichotomous outcomes, we calculated the relative risk (RR) and its corresponding 95% confidence interval (CI). For continuous outcomes, we calculated the weighted mean difference (WMD) and its corresponding 95%CI after we converted all the pain intensity data to the 10 cm visual analog scale (VAS) for pain (16). 1.5 cm was considered the minimal clinical important difference (MID) of pain intensity (17). We calculated the modeled risk difference (RD) value for comparisons to make the results easier to be understood.
We used a DerSimonian-Laird random effects model for all meta-analyses. Data were analyzed with STATA software version 17 (Stata Corp, College Station, TX, USA).
Certainty of evidence
2.5
We evaluated the certainty of evidence for all outcomes using the GRADE framework (Grading of Recommendations, Assessment, Development, and Evaluations) (18). Evidence from randomized controlled trials (RCTs) is initially rated as high certainty but was subject to downgrading by one or more levels (to moderate, low, or very low) following assessment across five domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias—the latter evaluated through visual inspection of funnel plot asymmetry where ≥10 studies contributed to a meta-analysis. We defined it imprecise when 95% CIs of pain intensity contained either half MID (0.75 cm) or 0 cm, and 95% CIs of adverse events included no difference (RR = 1).
Results
3
Search results and study characteristics
3.1
We screened 2,733 citations, identifying 57 eligible trials (19–75) involving 5,359 participants (search flow shown in Figure 1). The median of the mean ages reported across the 53 trials (19–25, 27–47, 49–57, 59–74) that provided age data was 22.3 years. Among the 44 trials (19–24, 27, 28, 30–34, 37–44, 47, 50–55, 57–64, 66, 68–74) reporting the duration of primary dysmenorrhea, the median of the mean durations was 44 months. Of the studies reporting location, 54 were conducted in Asia (19–28, 30–44, 46–74), two in Europe (29, 75), and one in South America (45). Twenty-eight trials (24–26, 29–34, 38, 40, 42, 45, 46, 48, 49, 52, 53, 55, 56, 59, 61, 64, 66–68, 73, 74) compared heat therapy with a control group [three (26, 29, 45) assessing short-term effects], and 24 trials (21–23, 27, 29, 35, 37, 39, 41, 44, 47, 50, 51, 54, 57, 58, 60, 62, 65, 69–72, 75) compared heat therapy with NSAIDs [two (29, 60) assessing short-term effects] (see Table 1).
Search flowchart.
Risk of bias
3.2
The risk of bias assessment for the 57 included trials is summarized in Supplementary Table 2. Random sequence generation was adequately reported in 36 trials (63%) (21, 27–29, 31–35, 39–42, 44, 45, 47, 49–53, 55–58, 60, 62, 64–69, 71, 72, 74), suggesting a low risk of selection bias for this domain in these studies. However, allocation concealment was implemented in only 17 trials (30%) (21, 27–29, 31–35, 39–42, 45, 52, 55, 74), potentially compromising 1.5 cm was considered the minimal clinica integrity. Only 3 trials (5%) (45, 52, 74) blinded participants, and 3 (5%) (28, 40, 45) blinded healthcare providers. This high risk of performance bias means that the expectation of receiving a therapeutic intervention (heat) could have influenced participants' reporting of pain relief. Similarly, blinding of outcome assessors and data analysts was reported in only 6 trials (11%) (28, 33, 35, 40, 41, 52), constituting a significant source of detection bias for the subjective outcome of self-reported pain. Importantly, no trials had ≥20% missing data, which minimizes bias from incomplete outcomes and strengthens the robustness of the pooled analysis.
Heat therapy vs. blank control
3.3
Pain analgesia over 3 months
3.3.1
Low-certainty evidence (25 RCTs, 2,393 patients) (24, 25, 30–34, 38, 40, 42, 46, 48, 49, 52, 53, 55, 56, 59, 61, 64, 66–68, 73, 74) showed that compared with blank intervention, patients with dysmenorrhea who received heat treatment may have experienced more pain relief (WMD −1.85 cm, 95% CI −2.29 to −1.41 cm; the modeled RD 21%, 95% CI 19% to 22%) (see Tables 2, 3; Figure 2).
Long-term pain relief: heat therapy group vs. blank group.
Pain analgesia within 24 h
3.3.2
Low-certainty evidence (3 RCTs, 248 patients) (26, 29, 45) suggested that compared with blank intervention, patients with dysmenorrhea who received heat treatment experienced more pain relief (WMD −3.52 cm, 95% CI −5.01 to −2.02 cm; the modeled RD 45%, 95% Cl 33% to 48%) (see Tables 2, 3; Figure 3).
Short-term pain relief: heat therapy group vs. blank group.
Adverse effects
3.3.3
Low-certainty evidence (7 RCTs, 784 patients) (30, 33, 40, 49, 52, 63, 74) indicated little to no difference in adverse effects between heat therapy and blank intervention for primary dysmenorrhea (RR 1.34, 95% Cl 0.44–4.16) (see Tables 2, 3; Figure 4).
Adverse effects in the heat therapy and bank groups.
Heat therapy vs. NSAIDs
3.4
Pain analgesia over 3 months
3.4.1
Low-certainty evidence (22 RCTs, 1,938 patients) (21–23, 27, 35, 37, 39, 41, 44, 47, 50, 51, 54, 57, 58, 62, 65, 69–72, 75) suggested that heat therapy and NSAIDs may be comparable in relieving pain, with WMD −1.10 cm (95% CI −1.51 to −0.70 cm), modeled RD 4% (95% CI 3% to 4%) (see Tables 2, 4; Figure 5).
Long-term pain relief: heat therapy group vs. NSAIDs group.
Pain analgesia within 24 h
3.4.2
Low-certainty evidence (2 RCTs, 167 patients) (29, 60) suggested that heat therapy and NSAIDs may show similar efficacy in pain relief, with WMD −1.5 cm (95% CI −2.86 to −0.15 cm), modeled RD 16% (95% CI 2% to 21%) (see Tables 2, 4; Figure 6).
Short-term pain relief: heat therapy group vs. NSAIDs group.
Adverse effects
3.4.3
Moderate-certainty evidence (8 RCTs, 728 patients) (19, 20, 27, 28, 36, 43, 47, 63) indicated that heat therapy probably reduced the risk of adverse effects compared with NSAIDs in primary dysmenorrhea (RR 0.3, 95% Cl 0.15 to 0.59) (see Tables 2, 4; Figure 7).
Adverse effects in the Heat therapy and NSAIDs groups.
Discussion
4
Overall findings
4.1
Compared to no treatment, heat therapy reduces pain in primary dysmenorrhea with comparable safety. When compared to NSAIDs, heat therapy demonstrates minimal difference in pain intensity but is probably associated with fewer adverse events. These treatment outcomes remain consistent across both short-term (24-h) and long-term (3-month) assessments.
Relation to other studies
4.2
We have identified two systematic reviews in the literature addressing heat therapy for primary dysmenorrhea (76, 77); however, we excluded 6 RCTs for specific reasons. The first meta-analysis (76) included three RCTs on thermotherapy. One trial was excluded due to a lack of baseline data (78). The other two (79, 80), with treatment durations of 1 and 2 months, were also excluded. The second meta-analysis (77) included six RCTs (29, 78, 80–83), only one of which was included in our analysis (29). The other five trials were excluded due to the absence of extractable outcome measures (78, 80, 81), unavailable resources (82), or non-compliant interventions (83). A detailed breakdown is provided in Supplementary Table 3.
Earlier systematic reviews offered valuable preliminary insights by suggesting heat therapy might be effective and potentially comparable to analgesic medication. However, their conclusions were notably constrained: Jo and Lee's analysis, while indicating superiority over placebo, was limited to only 6 RCTs (77); Igwea et al. identified merely 3 heat therapy trials, were unable to perform a direct comparative meta-analysis, and ultimately highlighted the need for more robust evidence (76).
Our study comprehensively addresses these limitations through key advancements: a markedly expanded evidence base (57 RCTs) enabling more precise and generalizable treatment estimates; broader intervention diversity encompassing microwave therapy, electromagnetic wave therapy, moxibustion, and hot packs beyond previous narrow focus; and demonstration of consistent therapeutic benefits across both immediate (24-h) and sustained (3-month) timeframes—a previously unexamined dimension. Methodologically, the systematic application of the GRADE framework provides rigorous evidence certainty assessment, thereby substantiating prior hypotheses and establishing a more reliable foundation for positioning heat therapy as a viable non-pharmacological treatment for primary dysmenorrhea.
Strengths and limitations
4.3
This review has several strengths. We predefined the MIDs to visually demonstrate between-group differences and evaluate the clinical significance of the findings. The calculation of MID-derived risk differences (RDs) further enhanced the interpretation of the clinical feasibility of treatment effects. Moreover, our study overcomes the limitations of previous analyses by comprehensively incorporating diverse thermotherapy modalities and leveraging a robust sample size, thereby yielding more precise and generalizable estimates.
Nevertheless, several limitations warrant consideration. The methodological quality of many included trials was compromised by inadequate randomization and concealment of allocation. Furthermore, significant heterogeneity was observed in some analyses, likely stemming from clinical diversity in patient populations and variations in heat therapy protocols. Finally, the predominance of studies conducted in Asian populations may limit the generalizability of our findings to other regions.
Implications
4.4
Our findings provide evidence for informing a stepped-care approach to managing primary dysmenorrhea. During acute episodes, local heat therapy using modalities such as hot water bottles or self-heating patches can provide immediate pain relief comparable to NSAIDs, with a superior safety profile. This offers an ideal first-line option for patients who cannot or prefer not to use medication. During the intermenstrual period, regular application of heat therapies like moxibustion or infrared therapy can serve as an effective preventive measure. Long-term adherence may reduce the frequency and intensity of pain episodes and decrease reliance on analgesic medications. For patients with severe pain, a “heat therapy-first, medication-as-supplement” combination strategy could be considered—employing heat therapy both preventively and during acute phases, reserving short-term NSAID use only for peak pain levels to optimize both efficacy and safety.
From a research perspective, the application of MIDs in our meta-analysis offers a concrete method for evaluating the clinical significance of future findings. However, the promising results are constrained by the low certainty of evidence and prevalent risk of bias in existing studies.
Future research should therefore prioritize high-quality, adequately powered RCTs that are specifically designed to overcome these limitations. We recommend that future trials: (1) calculate sample sizes based on the established MIDs for pain scales to ensure sufficient statistical power; (2) predefine and consistently apply a standardized heat intervention protocol (specifying temperature, application site, duration, and treatment frequency) to reduce heterogeneity; (3) adhere to the CONSORT reporting guidelines, providing clear descriptions of randomization, allocation concealment, and blinding methods; and (4) systematically record and report all adverse events to better establish the long-term safety profile of repeated heat application. Such rigorously generated evidence is crucial to confirm these findings and establish clear, evidence-based clinical guidelines.
Conclusion
5
Compared to no treatment, heat therapy is likely to reduce pain intensity both during prophylaxis and acute episodes. When compared to NSAIDs, heat therapy may achieve comparable analgesic efficacy with a superior safety profile.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Iacovides S Avidon I Baker FC. What we know about primary dysmenorrhea today: a critical review. Hum Reprod Update. (2015) 21:762–78. doi: 10.1093/humupd/dmv 03926346058 · doi ↗ · pubmed ↗
- 2Ferries-Rowe E Corey E Archer JS. Primary dysmenorrhea: diagnosis and therapy. Obstet Gynecol. (2020) 136:1047–58. doi: 10.1097/AOG.000000000000409633030880 · doi ↗ · pubmed ↗
- 3Dawood MY. Primary dysmenorrhea: advances in pathogenesis and management. Obstet Gynecol. (2006) 108:428–41. doi: 10.1097/01.AOG.0000230214.26638.0c 16880317 · doi ↗ · pubmed ↗
- 4Ju H Jones M Mishra G. The prevalence and risk factors of dysmenorrhea. Epidemiol Rev. (2014) 36:104–13. doi: 10.1093/epirev/mxt 00924284871 · doi ↗ · pubmed ↗
- 5Marjoribanks J Ayeleke RO Farquhar C Proctor M. Nonsteroidal anti-inflammatory drugs for dysmenorrhoea. Cochrane Database Syst Rev. (2015) 2015:Cd 001751. doi: 10.1002/14651858.CD 001751.pub 326224322 PMC 6953236 · doi ↗ · pubmed ↗
- 6Owen PR. Prostaglandin synthetase inhibitors in the treatment of primary dysmenorrhea. Outcome trials reviewed. Am J Obstet Gynecol. (1984) 148:96–103. doi: 10.1016/S 0002-9378(84)80039-36419611 · doi ↗ · pubmed ↗
- 7Essex MN Zhang RY Berger MF Upadhyay S Park PW. Safety of celecoxib compared with placebo and non-selective NSAI Ds: cumulative meta-analysis of 89 randomized controlled trials. Expert Opin Drug Saf. (2013) 12:465–77. doi: 10.1517/14740338.2013.78059523506230 · doi ↗ · pubmed ↗
- 8Xu T Hui L Juan YL Min SG Hua WT. Effects of moxibustion or acupoint therapy for the treatment of primary dysmenorrhea: a meta-analysis. Altern Ther Health Med. (2014) 20:33–42. 25141361 · pubmed ↗