Exploring the level of knowledge related to ectopic pregnancy among married Saudi women
Wjdan Almutairi, Amel Dawod Kamel Gouda, Shujun Almutiri, Rana Alhashemi, Razan Almubaraki, Hanadi Alshehri, Fawziah Almadhabri

TL;DR
This study found that most married Saudi women in Riyadh have poor knowledge about ectopic pregnancy, highlighting a need for educational programs.
Contribution
The study provides new insights into the knowledge gaps of ectopic pregnancy among Saudi women and suggests the need for targeted education.
Findings
60.4% of the women had a poor level of knowledge about ectopic pregnancy.
Only 8.6% of the participants demonstrated good knowledge of ectopic pregnancy signs, symptoms, and management.
Educational programs are recommended to improve awareness and understanding of ectopic pregnancy.
Abstract
Ectopic pregnancy (EP) is an abnormal condition in which blastocyst implantation occurs outside the lining of the uterus and is the leading cause of pregnancy-related death. Women who have had one ectopic pregnancy are at increased risk. Early diagnosis may reduce the risk of fallopian tube rupture. This study assessed the level of knowledge related to ectopic pregnancy among married Saudi women in Riyadh, Saudi Arabia. A descriptive cross-sectional design was used. This study was conducted at outpatient obstetrics clinics at the Women's Health Specialist Hospital at King Fahad National Guard Hospital in Riyadh. The convenience sample consisted of 255 pregnant women. The data were collected through a structured interviewing questionnaire, which consisted of demographic data and an ectopic pregnancy knowledge assessment tool. The study's findings revealed that the mean age of the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
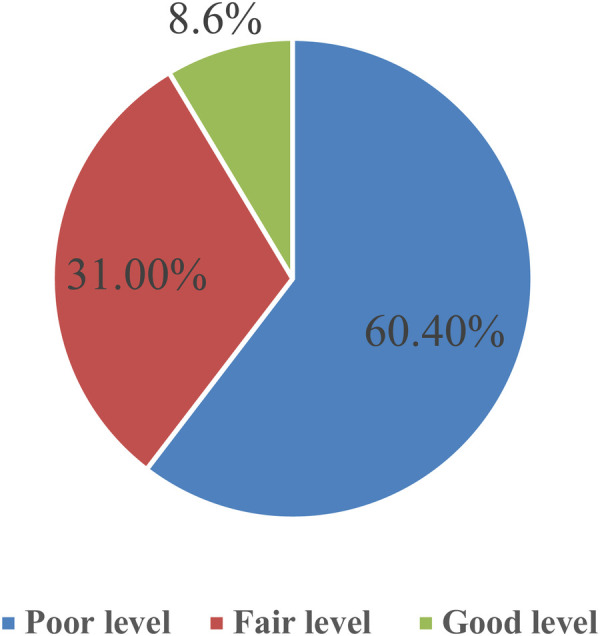 Figure 1
Figure 1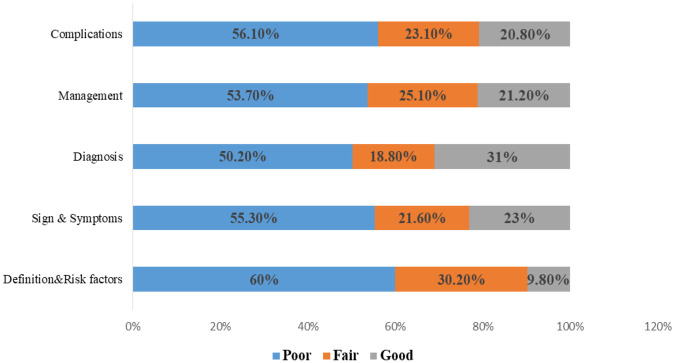 Figure 2
Figure 2| Items |
| % |
|---|---|---|
| Age | ||
| <18 | 0 | 0.0 |
| 18–25 years | 26 | 10.2 |
| 26–35 years | 81 | 31.8 |
| 36–45 years | 148 | 48 |
| Mean ± SD yrs | 35.50 ± 6.45 | |
| Educational level | ||
| Can't read or write | 2 | 0.8 |
| Primary Education | 10 | 3.9 |
| Preparatory Education | 20 | 7.8 |
| Secondary School | 53 | 20.8 |
| University Education | 170 | 66.7 |
| Marital status | ||
| Married | 237 | 92.9 |
| Divorced | 18 | 7.1 |
| Items | Freq. | % |
|---|---|---|
| Menstrual cycle regularity | ||
| Regular | 203 | 79.6 |
| Irregular | 52 | 20.4 |
| Number of pregnancies | ||
| Nulliparous | 12 | 4.7 |
| 1–2 | 71 | 27.8 |
| 3 | 27 | 10.6 |
| More than 3 | 145 | 56.9 |
| Number of deliveries | ||
| Nulliparous | 21 | 8.2 |
| 1–2 | 71 | 27.8 |
| 3 | 30 | 11.8 |
| More than 3 | 133 | 52.2 |
| Number of abortions | ||
| Yes | 113 | 44.31 |
| No | 142 | 55.7 |
| 1–2 | 92 | 36.1 |
| 3 | 12 | 4.7 |
| More than 3 | 9 | 3.5 |
| Mode of previous delivery | ||
| Yes | 234 | 91.76 |
| No | 21 | 8.2 |
| Normal Vaginal delivery | 163 | 63.9 |
| Cesarean Section | 71` | 27.8 |
| Family Planning Methods | ||
| Yes | 124 | 48.6 |
| No | 131 | 51.4 |
| If yes | ||
| Types of family planning methods: Oral contraceptives | 83 | 32.5 |
| IUD | 29 | 11.4 |
| Condom | 12 | 4.7 |
| Variables | I don't know (1) | Incomplete Answer (2) | Complete Answer (3) | |||
|---|---|---|---|---|---|---|
| Freq. | % | Freq. | % | Freq. | % | |
| Part I | ||||||
| Definition of ectopic pregnancy | 70 | 27.5 | 68 | 26.7 | 117 | 45.9 |
| Types of ectopic pregnancy | 171 | 67.1 | 50 | 19.6 | 34 | 13.3 |
| Fallopian tube | 150 | 58.8 | 44 | 17.3 | 61 | 23.9 |
| ovaries | 157 | 61.6 | 57 | 22.4 | 41 | 16.1 |
| On isthmus | 166 | 65.1 | 53 | 20.8 | 36 | 14.1 |
| Others | 203 | 79.6 | 32 | 12.5 | 20 | 7.8 |
| Causes of ectopic pregnancy | 190 | 74.5 | 46 | 18 | 19 | 7.5 |
| Inflammation | 197 | 77.3 | 43 | 16.9 | 15 | 5.9 |
| Hormonal disturbance | 161 | 63.1 | 72 | 28.2 | 22 | 8.6 |
| Pelvic operation | 190 | 74.5 | 44 | 17.3 | 21 | 8.2 |
| Uterus anomalies | 160 | 62.7 | 65 | 25.5 | 30 | 11.8 |
| Risk factors for ectopic pregnancy | 140 | 54.9 | 55 | 21.6 | 60 | 23.5 |
| Previous ectopic | 177 | 69.4 | 43 | 16.9 | 35 | 13.7 |
| Infertility | 188 | 73.7 | 44 | 17.3 | 23 | 9 |
| Family history | 184 | 72.2 | 43 | 16.9 | 28 | 11 |
| Age less than 18 years | 198 | 77.6 | 33 | 12.9 | 24 | 9.4 |
| Exhaustion | 187 | 73.3 | 47 | 18.4 | 21 | 8.2 |
| Tubal ligation | 162 | 63.5 | 58 | 22.7 | 35 | 13.7 |
| Mean total score part I | 26.55 ± 7.64 | |||||
| Categorize | ||||||
| Poor | 153 (60%) | |||||
| Fair | 77 (30.2%) | |||||
| Good | 25 (9.8%) | |||||
| Part II | ||||||
| Signs and symptoms of ectopic pregnancy | 165 | 64.7 | 58 | 22.7 | 32 | 12.5 |
| vaginal bleeding | 143 | 56.1 | 58 | 22.7 | 54 | 21.2 |
| Abdominal pain | 132 | 51.8 | 66 | 25.9 | 57 | 22.4 |
| Lower abdominal &back pain | 131 | 51.4 | 61 | 23.9 | 63 | 24.7 |
| Pain during urination | 155 | 60.8 | 61 | 23.9 | 39 | 15.3 |
| Upper shoulder pain | 201 | 78.8 | 36 | 14.1 | 18 | 7.1 |
| Mean Total Score Part II | 9.39 ± 3.62 | |||||
| Categorize | ||||||
| Poor | 141 (55.3%) | |||||
| Fair | 55 (21.6%) | |||||
| Good | 59 (23.1%) | |||||
| Part III | ||||||
| Diagnosis of ectopic pregnancy | 141 | 55.3 | 47 | 18.4 | 67 | 26.3 |
| Ultrasound | 117 | 45.9 | 49 | 19.2 | 89 | 34.9 |
| Blood test to measure B-HCG level | 150 | 58.8 | 62 | 24.3 | 43 | 16.9 |
| Laparoscopy | 145 | 56.9 | 57 | 22.4 | 53 | 20.8 |
| Mean total score part III | 6.81 ± 2.68 | |||||
| Categorize | ||||||
| Poor | 128 (50.2%) | |||||
| Fair | 48 (18.8%) | |||||
| Good | 79 (31%) | |||||
| Part IV | ||||||
| Management of ectopic pregnancy | 172 | 67.5 | 41 | 16.1 | 42 | 16.5 |
| Regular follow-up | 143 | 56.1 | 55 | 21.6 | 57 | 22.5 |
| Laparoscopy surgery | 144 | 56.5 | 62 | 24.3 | 49 | 19.2 |
| Treating according to the cases | 140 | 54.9 | 56 | 22 | 59 | 23.1 |
| Mean Total Score Part IV | 6.46 ± 2.56 | |||||
| Categorize | ||||||
| Poor | 137 (53.7%) | |||||
| Fair | 64 (25.1%) | |||||
| Good | 54 (21.2%) | |||||
| Part V | ||||||
| Complications of ectopic pregnancy | 151 | 59.2 | 62 | 24.3 | 42 | 16.5 |
| severe bleeding | 134 | 52.5 | 62 | 24.3 | 59 | 23.1 |
| Vaginal infection | 168 | 65.9 | 70 | 27.5 | 17 | 6.7 |
| Abdominal pain& distention | 142 | 55.7 | 72 | 28.2 | 41 | 16.1 |
| Nausea and vomiting | 148 | 58 | 72 | 28.2 | 35 | 13.7 |
| Problems with the bladder & intestine | 170 | 66.7 | 61 | 23.9 | 24 | 9.4 |
| Mean total score part V | 9.27 ± 3.46 | |||||
| Categorize | ||||||
| Poor | 143 (56.1%) | |||||
| Fair | 59 (23.1%) | |||||
| Good | 53 (20.8%) | |||||
| Mean total knowledge score | ||||||
| Total knowledge categories | ||||||
| Poor level | 154 (60.4%) | |||||
| Fair level | 79 (31%) | |||||
| Good level | 22 (8.6%) | |||||
| Variables | Minimum | Maximum | M | ±SD |
|---|---|---|---|---|
| Part I | 18 | 54 | 26.55 | 7.64 |
| Part II | 6 | 18 | 9.39 | 3.62 |
| Part III | 4 | 12 | 6.81 | 2.68 |
| Part IV | 4 | 12 | 6.46 | 2.56 |
| Part V | 6 | 18 | 9.27 | 3.46 |
| Total knowledge | 38 | 114 | 56.96 | 17.09 |
| Items | Poor ( | Fair ( | Good ( | |
|---|---|---|---|---|
| Age | ||||
| 18–25 years | 14 (9.1) | 7 (8.9) | 5 (22.7) | X = 6.49, |
| 26–35 years | 47 (30.5) | 30 (38) | 4 (18.2) | |
| 36–45 years | 93 (60.4) | 42 (53.2) | 13 (59.1) | |
| Educational level | ||||
| Can't read or write | 2 (1.3) | 0 (0.0) | 0 (0.0) | X = 8.05, |
| Primary Education | 7 (4.5) | 1 (1.3) | 2 (9.1) | |
| Preparatory Education | 11 (7.1) | 8 (10.1) | 1 (4.5) | |
| Secondary School | 32 (20.8) | 16 (20.3) | 5 (22.7) | |
| University Education | 102 (66.2) | 54 (68. | 14 (63.6) | |
| Marital status | ||||
| Married | 147 (95.5) | 70 (88.6) | 20 (90.9) | X = 3.88, |
| Divorced | 7(4.5) | 9(11.4) | 2(9.1) | |
| Items | Poor ( | Fair ( | Good ( | |
|---|---|---|---|---|
| Menstrual cycle regularity | ||||
| Regular | 123 (79.9) | 63 (79.7) | 17 (77.3) | X = 0.08, |
| Irregular | 31 (20.1) | 16 (20.3) | 5 (22.7) | |
| Number of pregnancies | ||||
| Nulliparity | 6 (3.9) | 4 (5.1) | 2 (9.1) | X = 6.42, |
| 1–2 | 38 (24.7) | 45 (57) | 7 (31.8) | |
| 3 | 20 (13) | 4 (5.1) | 3 (13.6) | |
| More than 3 | 90 (58.4) | 26 (32.9) | 10 (45.5) | |
| Number of deliveries | ||||
| Nulliparous | 13 (8.4) | 9 (9) | 2 (8.7) | X = 2.58, |
| 1–2 | 39 (25.3) | 30 (30) | 9 (39.1) | |
| 3 | 20 (13) | 10 (10) | 3 (13) | |
| More than 3 | 82 (53.2) | 51 (51) | 9 (39.1) | |
| Number of abortions | ||||
| No | 6 (3.9) | 5 (6.3) | 1 (4.5) | X = 2.71, |
| 1–2 | 5 (3.2) | 4 (5.1) | 0 (0.0) | |
| 3 | 85 (55.2) | 45 (57) | 12 (54.5) | |
| More than 3 | 58 (37.7) | 25 (31.6) | 9 (40.9) | |
| Mode of previous delivery | ||||
| No | 14 (9.1) | 4 (5.1) | 3 (13.6) | X = 4.72, |
| Normal Vaginal delivery | 93 (60.4) | 54 (68.4) | 16 (72.7) | |
| Cesarean Section | 47 (30.5) | 21 (26.6) | 3 (13.6) | |
| Family Planning Methods | ||||
| Yes | 72 (46.8) | 39 (49.4) | 13 (59.1) | X = 1.19, |
| No | 82(53.2) | 40(50.6) | 9(40.9) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEctopic Pregnancy Diagnosis and Management · Reproductive Health and Contraception · Gynecological conditions and treatments
Introduction
1
Ectopic pregnancy is a medical emergency that increases the risk of maternal morbidity and death. It is also the primary cause of maternal mortality in the first trimester of pregnancy, accounting for approximately 10% of all pregnancy-related deaths (1). Pregnant women are prone to high morbidity and mortality due to the undiagnosed and delayed complications of ectopic pregnancy (2). Ectopic pregnancy is an abnormal condition in which the implantation of a blastocyst occurs outside the lining of the uterus. It is particularly important in gynecology in developing countries, as it contributes substantially to first-trimester morbidity and maternal mortality (3). Due to the nonspecific nature of its presentation, ectopic pregnancy should be ruled out first in all pregnant women presenting with abdominal pain, vaginal bleeding, or non-specific symptoms such as nausea and vomiting. Notably, approximately one-third of women with ectopic pregnancy may be asymptomatic, and up to 10% may exhibit no clinical signs at all (4). The clinical indicators that may suggest ectopic pregnancy include increased human chorionic gonadotropin, vaginal bleeding of varying amounts, abrupt lower abdomen pain, pelvic pain, a painful cervix, an adnexal mass, or adnexal tenderness (1). However, adnexal tenderness may only be present when the ectopic pregnancy is located in the adnexa. Clinicians should also consider non-tubal ectopic pregnancies, such as intrauterine ectopic gestations (5).
A successful intrauterine pregnancy depends on a complex interplay of chemical, hormonal, and anatomical factors during fertilization, tubal transport, and embryo implantation (6). Disruption of these processes may predispose to ectopic implantation, and local factors such as prior infection, immunologic alterations, viral exposure, toxic substances, fibrotic, or mechanical mechanisms, thereby delaying embryo transport and increasing the risk of implantation outside the endometrial cavity (7). Ectopic pregnancy presents in several forms, including tubal, corneal, cesarean scar, cervical, heterotypic, abdominal, and ovarian pregnancies. Among these, tubal ectopic pregnancies are the most common and have high maternal morbidity and fatality rates when ruptured. Without timely assessment using the human chorionic gonadotrophin (hCG) or the ultrasound, severe vaginal bleeding from a ruptured ectopic pregnancy may be mistaken for a miscarriage, potentially delaying critical treatment. While symptoms such as nausea, vomiting, and diarrhea are less common in ectopic pregnancy, rupture often precipitates acute clinical manifestations, including hypovolemic shock, peritonitis, abdominal distension, and severe abdominal pain (1).
To treat ectopic pregnancy, confirmation of ectopic pregnancy is necessary. In cases where the early diagnosis of an ectopic pregnancy is unsuitable for active monitoring, medical treatment with methotrexate may be suggested. It is administered intramuscularly and may be given as a single dose or as a multi-dose regimen, depending on clinical criteria, ultrasound findings, initial human chorionic gonadotropin (hCG) levels, and the patient's response to treatment (8). Additionally, laparoscopy, or keyhole surgery, is performed to remove the pregnancy before it becomes too large (8). Early detection of an ectopic pregnancy is essential for preventing additional damage to the tube, lowering the risk of morbidity, and maintaining fertility. An ectopic pregnancy needs to be ruled out if the pregnancy test is positive and the ultrasound reveals an empty uterus (9).
Ectopic pregnancy is reported to be a common condition among women of childbearing age. The reported estimated incidence of ectopic pregnancies in the United States is 1%–2%, and ruptured ectopic pregnancies are responsible for 2.7% of pregnancy-related deaths (10). From 2010 to 2019, there were 15,537 ectopic pregnancies out of 979,027 pregnancies among women in California aged 15–44 years (11). In Saudi Arabia, the reported prevalence of ectopic pregnancy ranges from 1% to 2% of the overall number of pregnancies in Majmaah city of Saudi Arabia (12). Regarding the level of knowledge of ectopic pregnancy, women reported poor knowledge of EP (12). In India, although 25% of graduate-aged women and 43% of postgraduate-aged women reported being aware of EP, they demonstrated poor knowledge. Up to 98% had poor knowledge related to risk factors for EP (13). On the other hand, a study in southeastern Nigeria reported that up to 60% of participants were aware of EP, and the majority had a moderate to good level of knowledge about EP (14, 15).
Awareness of ectopic pregnancy is important, as unfavorable clinical outcomes are more likely to occur with poorer levels of EP knowledge (16). Furthermore, inadequate knowledge is associated with older age groups, lower-income groups, non-professional occupations, and lower educational attainment (16). Nurses, midwives, and other healthcare providers play a crucial role in educating women and their partners about the warning signs and symptoms of ectopic pregnancy, as well as providing preconception care. When an ectopic pregnancy is suspected, both the woman and her partner must be informed about the potential implications for her health and future fertility (17). Currently, there is limited research on women's knowledge of ectopic pregnancy in Saudi Arabia, especially in the central regions of Saudi Arabia. Also, there is limited evidence from Saudi Arabia assessing women's knowledge of ectopic pregnancy. This study was designed to help bridge the gap between theory and clinical practice. Enhancing awareness of potential risk factors for ectopic pregnancy can facilitate early detection, reduce morbidity, and prevent complications. Therefore, prioritizing early recognition and timely treatment is critical to minimizing the adverse outcomes and mortality associated with ectopic pregnancy.
Materials and methods
2
Study design
2.1
A descriptive cross-sectional study design was utilized to assess the level of knowledge about ectopic pregnancy among married Saudi women.
Aim of the study
2.2
This study aimed to assess the level of knowledge related to ectopic pregnancy among married Saudi women.
Research questions
2.3
What is the level of knowledge about ectopic pregnancy among married Saudi women?How does the level of knowledge about ectopic pregnancy among married Saudi women vary based on demographic status and obstetrical variables?
Sample
2.4
A convenience sample of approximately 255 women visited the outpatient gynecologic and obstetric clinic at the Women's Health Specialist Hospital at King Abdulaziz Medical City, which was selected using a convenience sampling approach due to its accessibility and high patient volume. Data Collection was conducted over a 3-month period from early January 2024 to the end of March 2024. The study sample was recruited according to the following inclusion criteria: Married Saudi women aged 18–45 years. Women who attended any educational sessions regarding ectopic pregnancy in the last 12 months or had experienced an ectopic pregnancy were excluded from the current study.
Sample size
2.5
The sample size was calculated using Raosoft, a software tool that determines the necessary sample size for the current study based on the average number of patients (approximately 15,000 patients per year), with a 95% confidence level and a 0.5% confidence interval. The calculated sample size was 248, and a sample of 255 was included in the study to ensure the representativeness of the total population.
Setting
2.6
The study was conducted at the outpatient clinic for prenatal care at the National Guard Women's Health Hospital, Riyadh, Saudi Arabia. It is an affiliated hospital that offers a comprehensive range of services, including labor and delivery, C-section surgery, and gynecological procedures, as well as intensive and intermediate care for neonates. It includes an in vitro fertilization clinic, a maternal-fetal medicine clinic, a breast health clinic, a general obstetrics and gynecology clinic, and a comprehensive imaging department with a capacity of 300 beds.
Tools of data collection
2.7
The questionnaire was constructed by the researchers after an extensive review of the literature (18), and it was reviewed by a panel of maternity nursing professors at the King Saud bin Abdulaziz University for Health Science. This tool was written in simple and straightforward Arabic. This study aimed to assess maternity women's knowledge regarding ectopic pregnancy and included three parts. The first part included sociodemographic data, such as women's age, educational level, and marital status. The second part included gynecological and obstetrical data, such as menstrual regularity, number of pregnancies, number of deliveries, number of abortions, date of the last labor, complications in previous pregnancies, and current pregnancy history. The third part was divided into five sections, including a knowledge assessment sheet concerning women's knowledge and attitudes regarding ectopic pregnancy. It covered information about the definition, types, causes, and risk factors for ectopic pregnancy (from questions 1 to 7). Part two included knowledge of women regarding the signs and symptoms of ectopic pregnancy (from questions 8 to 9). Part three examined the knowledge of women regarding the diagnosis, management, and treatment of ectopic pregnancy (from questions 10 to 11). Part four included women's knowledge regarding the management of ectopic pregnancy (from questions 12 to 13). Part five assessed the knowledge of women regarding complications (from questions 14 to 15), with a total of 15 questions. In the scoring system, each question was assigned a score of 1 for the incorrect answer or “I don’t know,” a score of 2 for the correct but incomplete answer, and a score of 3 for the correct and complete answer. The total knowledge score was classified as follows: correct knowledge (good) ≥75%, incomplete knowledge (fair) from 74% to 50%, and incorrect (poor) knowledge less than 50%.
Tool validity and reliability
2.8
The face validity and content validity of the questionnaire were developed by the researcher, and five experts in the field of maternity nursing and obstetric medicine tested its content validity. Modifications were made according to the experts' judgment on the clarity of the sentences and the appropriateness of the content. After the questionnaire was collected, the researcher applied test reliability to assess the internal consistency of the tool. Cronbach's alpha = α in part I was 0.72, that in part II was 0.77, that in part III was 0.85, that in part IV was 0.88, that in part V was 0.82, and the total tool reliability was estimated at 0.95, indicating a strong positive correlation between the tools.
Procedures
2.9
Over three months, beginning in early January 2024 and ending of March 2024, data were collected. Three days a week (Monday, Wednesday, and Thursday) from 9 AM to 12 PM, the researcher attended an outpatient obstetrics and gynecology clinic. After receiving official permission from the Women's Health Specialist Hospital at King Abdulaziz Medical City, the researcher contacted the medical and nursing directors of the outpatient gynecologic and obstetrics clinics to explain the study's purpose and benefits to the participants, all participants received a written description of the study before enrolling and written formal consent was obtained from all participants. The researcher then recruited the women from the outpatient obstetrics and gynecology clinic, explained the nature and goal of the study, and obtained informed consent from those who met the criteria for inclusion and agreed to participate. Every woman included in the study sample was interviewed in the waiting area to obtain information on her demographics, her obstetrical and gynecological health, and her level of knowledge about ectopic pregnancy. To collect data, the researcher spoke with each woman one-on-one privately, asked the questions in simple Arabic, and recorded each woman's response in a questionnaire. Each woman's interview lasted between ten and fifteen minutes.
Statistical design
2.10
To prevent any inconsistencies, the researcher reviewed all the data. The data were checked for coding and entry errors, and then the data were tabulated and presented via both inferential and descriptive statistics. The level of significance was set at <0.05, and p > 0.05 denotes a significant result. The p-value represents the likelihood of error in the conclusion.
Results
3
The study utilized descriptive methods to characterize the study sample. Chi-square analysis was employed to assess relationships within the data, with significance determined by a threshold of p < 0.05. The findings revealed no statistical relationships between demographics, obstetrical factors, or the level of knowledge regarding ectopic pregnancy.
The results of the current study are presented below.
Part (I): demographic characteristics of the study sample
3.1
Table 1 shows the frequency distributions of the demographic characteristics. Nearly half of the study sample (48%) were aged between 36 and 45 years. A total of 10.2% of them were aged between 18 and 25 years, with a mean age of 35.50 ± 6.45 years. Regarding the level of education, more than half of the study sample (66.7%) had a university education. However, 0.8% were unable to read and write. Most of the participants (92.9%) were married.
Table 2 shows the frequency distribution of the obstetric history of the study sample. Two-thirds of the study participants (79.6%) had regular menstrual cycles. More than half of them (56.9% and 52.2%, respectively) had experienced more than three pregnancies and deliveries. Approximately 36.1% of the samples had undergone 1–2 abortions. Among the study participants, 63.9% delivered via normal vaginal delivery, whereas 27.8% delivered via cesarean section. Additionally, 48.6% of the sample reported using family planning methods, with 32.5% using oral contraceptives.
Part (II): description of the study sample toward the level of knowledge related to ectopic pregnancy among married Saudi women
3.2
Table 3 presents the study sample's understanding of ectopic pregnancy, including its definition, causes, risk factors, signs and symptoms, complications, and management, with a mean knowledge score of 56.96 ± 17.09. Among the total knowledge categories, more than half of them had a poor level of knowledge, 31% had a fair level, and the remaining score of 8.6% had a good level of knowledge regarding ectopic pregnancy (Figure 1).
Distribution of the study sample according to the level of knowledge of ectopic pregnancy.
Specifically, among the participants in part I, 60% exhibited a poor level of knowledge concerning the definitions, types, causes, and risk factors associated with ectopic pregnancy. Conversely, 9.8% demonstrated a good level of understanding, whereas the remaining 30.2% possessed fair knowledge (Figure 2). The mean score obtained was 26.55, with a standard deviation of ±7.64. According to Part II of the study, the mean score recorded was 9.39, with a standard deviation of ±3.62. Concerning the understanding of signs and symptoms associated with ectopic pregnancy, 23.1% of the participants demonstrated a good level of knowledge, 21.6% exhibited fair understanding, and the majority, accounting for 55.3%, presented a poor level of knowledge. Part III revealed that the mean score for knowledge of diagnostic tests for ectopic pregnancy was 6.81, with a standard deviation of ±2.68. Among the participants, 50.2% exhibited poor knowledge, 18.8% demonstrated fair understanding, and 31% showed good comprehension of the diagnostic criteria of ectopic. Among the participants in part IV, 53.7% lacked knowledge regarding the management of ectopic pregnancy, 21.2% demonstrated a good understanding, and 25.1% exhibited fair knowledge. The mean score for this section was recorded as 6.46, with a standard deviation of ±2.56. Finally, in part V of the study, 56.1% of the participants had a poor understanding of the complications associated with ectopic pregnancy, 23.1% had fair knowledge, and 20.8% had a good level of understanding. The mean score for this section was calculated as 9.27, with a standard deviation of ±3.46.
Distribution of the study sample regarding the categories of knowledge of ectopic pregnancy.
As shown in the figure, in terms of overall knowledge categories, over half (60.40%) reported a low level of understanding, 31% reported a moderate level, and the remaining 8.6% reported a high level of knowledge concerning ectopic pregnancy.
Table 4 shows a summary of the minimum, maximum, mean, and standard deviation of all the knowledge regarding ectopic pregnancy among the study sample.
Part (III): the relationship between selected demographic & obstetrical variables and level of knowledge toward ectopic pregnancy
3.3
Table 5 shows that there was no relationship between selected demographic variables, such as maternal age, educational level, marital status, and level of knowledge of ectopic pregnancy, with p values >0.05.
Table 6 shows that there was no relationship between selected obstetrical variables, such as maternal menstrual cycle regularity, number of pregnancies, number of deliveries, number of abortions, mode of previous delivery, and used family planning methods, and level of knowledge toward ectopic pregnancy, with a p value >0,05.
Regarding the definition and risk factors, 60% of the participants exhibited a poor level of knowledge, 30.20% demonstrated fair knowledge, and 9.80% possessed good knowledge. Concerning the signs and symptoms of ectopic pregnancy, 55.30% had poor knowledge, 23% demonstrated good knowledge, and 21.60% had fair knowledge. In terms of diagnosis, 5.20% displayed a good understanding, 18.80% had fair knowledge, and 31% possessed good knowledge. Concerning management, 21.20% exhibited good knowledge, whereas the majority, comprising 53.70%, had poor knowledge, and 25.10% had fair knowledge. Finally, concerning the complications of ectopic pregnancy, the majority, 56.10% of the sample, demonstrated a poor level of knowledge, 23.10% had fair knowledge, and 20.80% exhibited good knowledge.
Discussion
4
This study sought to evaluate awareness levels regarding ectopic pregnancy (EP) among married Saudi women in Riyadh. Our demographic analysis revealed a significant concentration of participants within the 36–45 years age bracket, with a notable representation from the 26–35 years age group. The majority of participants had attained a university education, indicating a relatively educated cohort. Notably, the variation in the age and education level of the participants did not impact their level of awareness of EP. Furthermore, the study sample predominantly comprised married women, thus providing focused insight into this demographic segment's awareness levels.
Regarding knowledge levels, our findings revealed that more than half of the participants exhibited a limited understanding of EP, whereas approximately one-third demonstrated a fair understanding. These results were compared with those of a similar study focusing on married women from Chi Linh district in Vietnam (19), which reported comparable levels of inadequate knowledge. Notably, a study focused on younger participants from Southeastern Nigeria aged 20–24 years has reported a higher prevalence of good knowledge, suggesting potential age-related disparities in awareness levels (15). Also, up to 98% reported poor knowledge related to the signs, symptoms, and risk factors of ectopic pregnancy (13). Based on our analysis, the difference between our study and a similar study can be attributed to the targeted age groups (15). We focused on older women, whereas the other study in Southeastern Nigeria targeted younger women (15). This age difference likely contributed to the positive results observed in the study, as younger participants may have better access to information and educational resources regarding EP. However, a hospital-based study in Pakistan documented how often specific signs/symptoms occur among patients with ectopic pregnancy: amenorrhea (87.5%), abdominal pain (81.3%), vaginal bleeding (68.8%) were among the most frequent. Yet, such evidence underscores how common these symptoms are in EP, highlighting the gap between public awareness and what is clinically typical (20).
Exploring EP risk factors, our study underscored a prevalent lack of knowledge among more than half of the participants. This aligns with findings from the study in India, which emphasized a widespread deficit in understanding EP risk factors among married women (13). Contrary outcomes were reported in a study that was conducted among female undergraduates in southeastern Nigeria (19). The study observed a higher level of knowledge, highlighting the influence of educational background and age on variations in knowledge (19).
Concerning signs and symptom comprehension, our study revealed a substantial knowledge gap, with more than half of the participants exhibiting poor awareness; they did not know that bleeding, abdominal pain, lower back pain, and shoulder pain were signs of EP. A similar trend was reported, indicating a significant lack of understanding of signs and symptoms among participants, where most participants knew only one sign of abnormal pregnancy (13). Nearly half of the participants demonstrated good knowledge of signs and symptoms, suggesting that potential variation in the targeted sample can contribute to the variation in the level of awareness (19). Thus, a lack of awareness of ectopic pregnancy symptoms can lead to delayed diagnosis and mismanagement, which increases the risk of life-threatening complications. Improved education and awareness campaigns are crucial for promoting early detection, effective management, and better outcomes for individuals affected by EP.
The observed variability in knowledge levels across participants, despite similarities in marital status and relatively high educational attainment, suggests substantial heterogeneity within the study population. This heterogeneity may reflect unmeasured factors such as prior healthcare experiences, in vitro fertilization treatment, or interaction with healthcare services. High heterogeneity limits the generalizability of aggregate knowledge scores, indicating that awareness gaps are not confined to specific demographic subgroups. Consequently, uniform educational strategies may be insufficient, and tailored awareness programs addressing diverse informational needs are warranted.
Despite thorough consideration of demographic variables such as maternal age, educational attainment, and marital status, our study did not establish a significant correlation between the level of knowledge about EP and these variables. This finding, which aligns with previous studies (15), further emphasizes that heterogeneity in awareness exists beyond conventional demographic predictors. Therefore, comprehensive public health strategies that deliver consistent, accessible, and culturally appropriate education on ectopic pregnancy are essential to improve early recognition, prompt care-seeking behavior, and maternal health outcomes.
Conclusion
5
In summary, the findings of this study highlight a concerning trend regarding knowledge levels surrounding ectopic pregnancy, with a significant majority of the sample demonstrating a poor understanding. With only a minority possessing a fair or good level of knowledge, there is a pressing need for targeted education and awareness campaigns to improve understanding and ultimately reduce the risks associated with this potentially life-threatening condition. Clinically, inadequate awareness of ectopic pregnancy may contribute to delayed presentation, misinterpretation of symptoms, and increased risk of complications, including tubal rupture and maternal morbidity. Enhancing public knowledge can facilitate earlier recognition of warning signs, prompt medical evaluation, and timely intervention, ultimately improving maternal health outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mullany K Minneci M Monjazeb R C. Coiado O. Overview of ectopic pregnancy diagnosis, management, and innovation. Womens Health. (2023) 19:17455057231160349. 10.1177/17455057231160349 PMC 1007115336999281 · doi ↗ · pubmed ↗
- 2Vadakekut ES Gnugnoli DM. Ectopic Pregnancy. in: Stat Pearls. Treasure Island (FL): Stat Pearls Publishing (2025). Available online at: http://www.ncbi.nlm.nih.gov/books/NBK 539860/ (Accessed September 21, 2025).30969682 · pubmed ↗
- 3Gerema U Alemayehu T Chane G Desta D Diriba A. Determinants of ectopic pregnancy among pregnant women attending referral hospitals in southwestern part of Oromia regional state, Southwest Ethiopia: a multi-center case control study. BMC Pregnancy Childbirth. (2021) 21(1):130. 10.1186/s 12884-021-03618-733579224 PMC 7881641 · doi ↗ · pubmed ↗
- 4Sivalingam VN Duncan WC Kirk E Shephard LA Horne AW. Diagnosis and management of ectopic pregnancy. J Fam Plan Reprod Health Care Fac Fam Plan Reprod Health Care R Coll Obstet Gynaecol. (2011) 37(4):231–40. 10.1136/jfprhc-2011-0073 PMC 321385521727242 · doi ↗ · pubmed ↗
- 5Stabile G Vona L Carlucci S Pitsillidi A Restaino S Vizzielli G Uterine ectopic pregnancies and live births: systematic review of the literature and concepts underlying favorable outcomes. Medicina (Mex). (2025) 61(11):1915. 10.3390/medicina 61111915 PMC 1265399741303752 · doi ↗ · pubmed ↗
- 6Papakonstantinou A Moustakli E Potiris A Zikopoulos A Tsarna E Christodoulaki C Behind-the-Scenes actors in fertility: a comprehensive review of the female reproductive tract microbiome and its clinical relevance. Life. (2025) 15(6):916. 10.3390/life 1506091640566568 PMC 12193755 · doi ↗ · pubmed ↗
- 7Mc Queen BE Kiatthanapaiboon A Fulcher ML Lam M Patton K Powell E Human fallopian tube epithelial cell culture model to study host responses to Chlamydia trachomatis infection. Infect Immun. (2020) 88(9):10.1128/iai.00105-20. 10.1128/IAI.00105-20PMC 744075732601108 · doi ↗ · pubmed ↗
- 8American College of Obstetricians and Gynecologists. ACOG Practice bulletin No. 193: tubal ectopic pregnancy. Obstet Gynecol. (2018) 131(3):e 91. 10.1097/AOG.000000000000256029470343 · doi ↗ · pubmed ↗