Oral hygiene and caries experience in children with down syndrome and autism spectrum disorder: a systematic review and meta-analysis
Nurzhamal Bainazarova, Kuralay Zhumabayeva, Gulzhan Yermukhanova, Yagut H. Hajiyeva, Kulmira Abdykerimova, Lyazat Orakbay, Farida Zhumageldiyeva, Indira Karibayeva, Nurlan Jainakbayev

TL;DR
This study finds that children with Down syndrome or autism have similar oral health to neurotypical children, despite facing more challenges.
Contribution
The study provides a systematic review and meta-analysis comparing oral health indices in children with Down syndrome, autism, and neurotypical peers.
Findings
Children with Down syndrome and autism showed no consistent differences in plaque or gingival indices compared to neurotypical peers.
Most differences in dental caries and oral hygiene indices were not statistically significant due to high heterogeneity.
Sensitivity analysis suggested a significant effect on plaque index after excluding an influential study.
Abstract
Children with Down syndrome (DS) and autism spectrum disorder (ASD) are at increased risk for oral health problems due to anatomical, behavioral, and socioeconomic factors. However, evidence on their caries experience and oral hygiene remains inconsistent. This study systematically reviewed and meta-analyzed case–control and cross-sectional studies comparing oral health indices in children with DS or ASD to neurotypical peers. A systematic search was conducted in PubMed, Web of Science, Science Direct, and Google Scholar using a standardized strategy. Eligible studies included children aged 0–18 years. Pooled mean differences (MD) in Plaque Index (PI), Gingival Index (GI), DMFT (decayed, missing, and filled permanent teeth), dmft (primary teeth), and Simplified Oral Hygiene Index (OHI-S) with 95% confidence intervals (CI) were calculated in R using meta and metafor packages.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
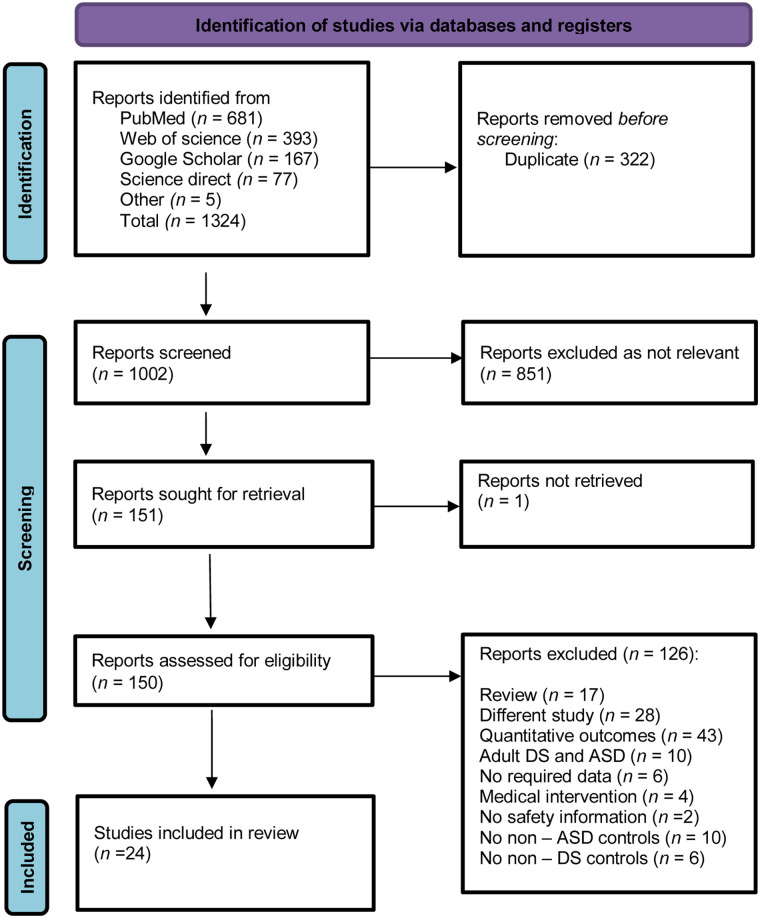 Figure 1
Figure 1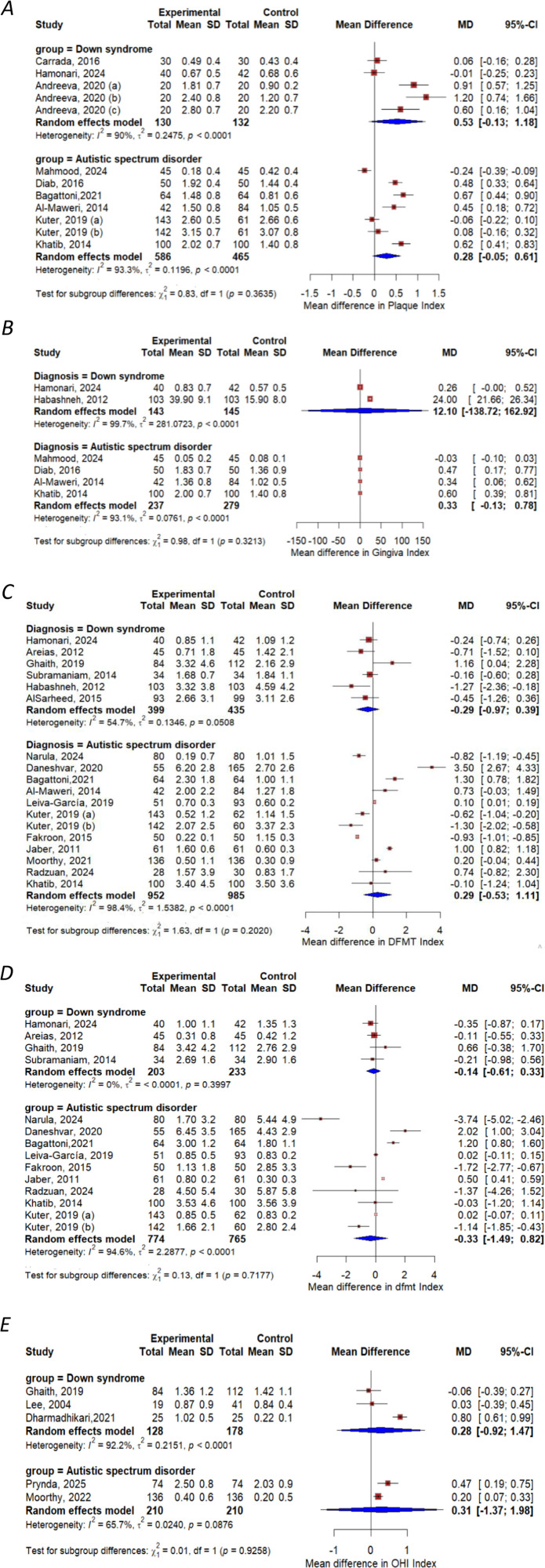 Figure 2
Figure 2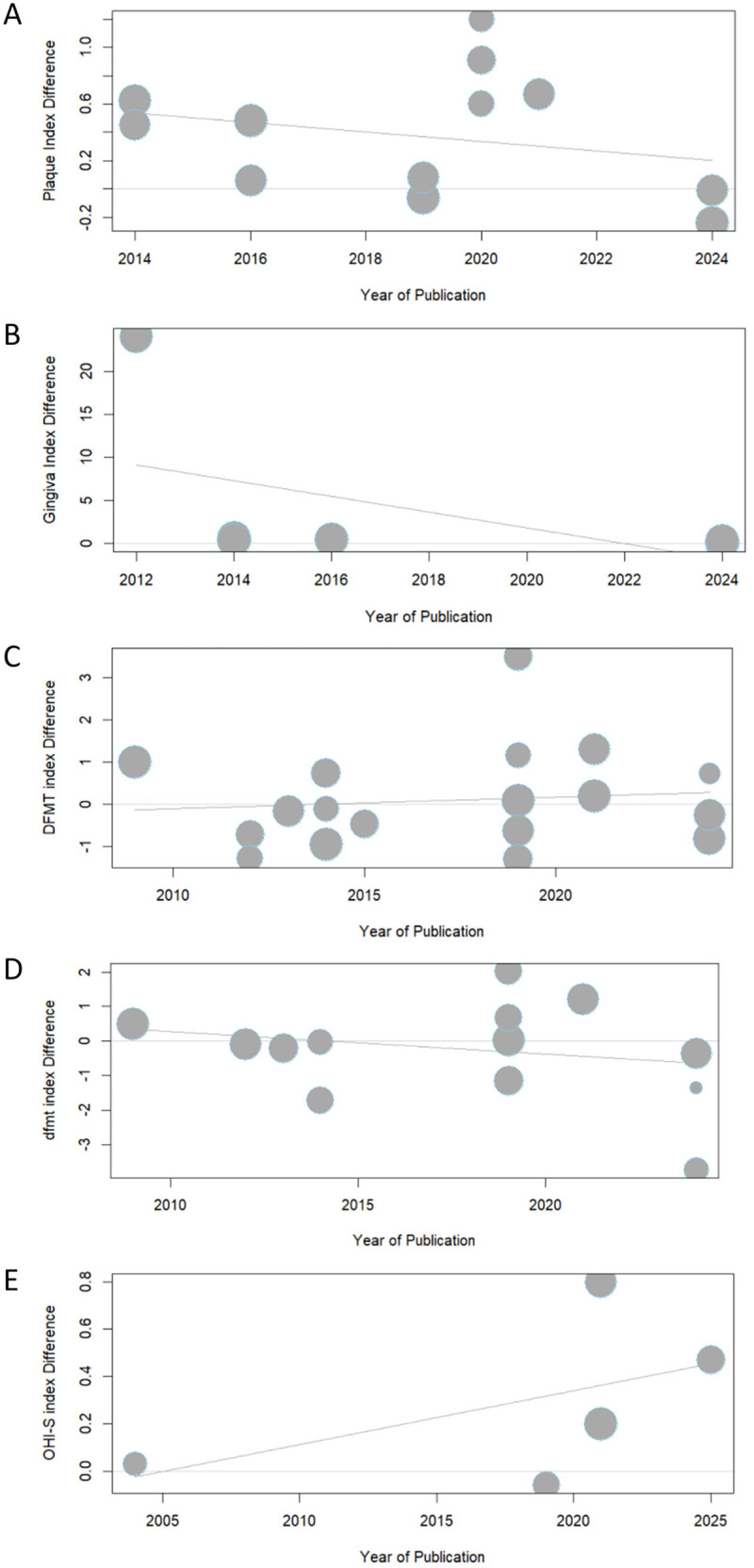 Figure 3
Figure 3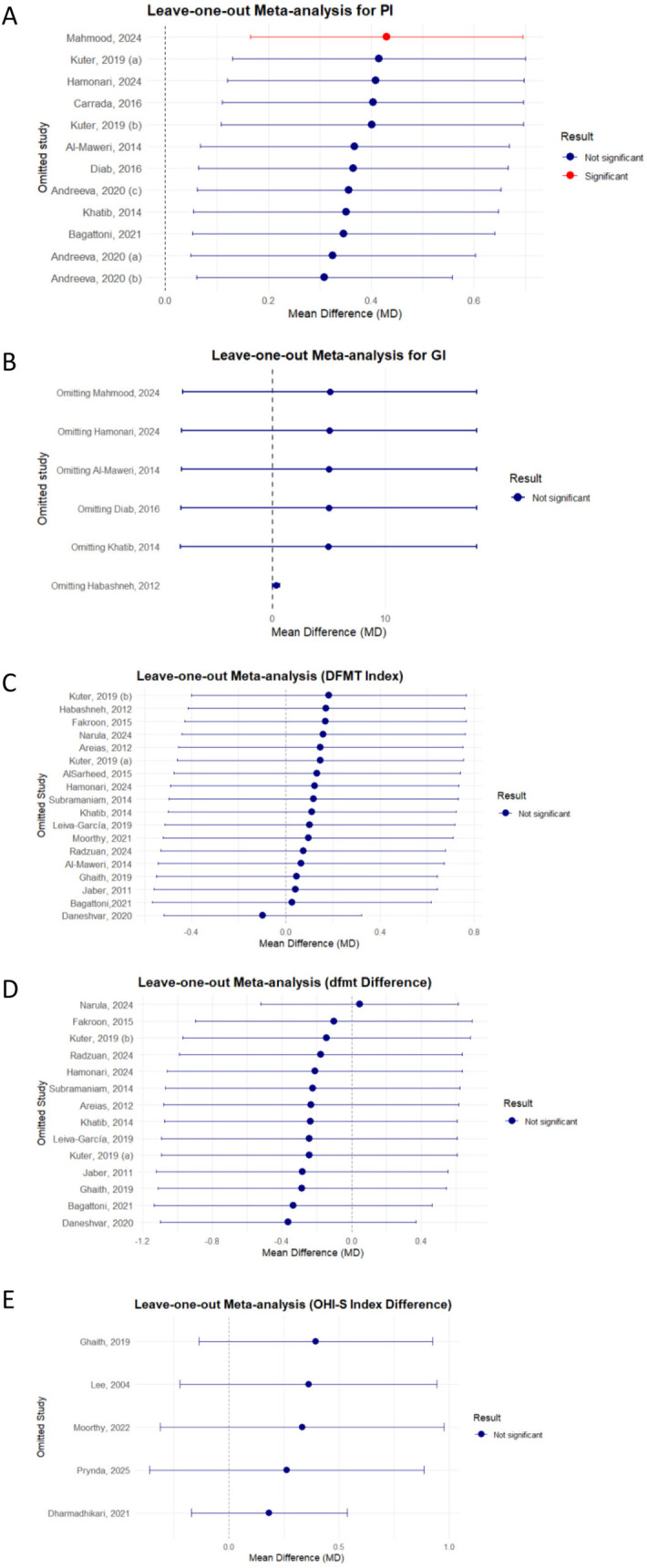 Figure 4
Figure 4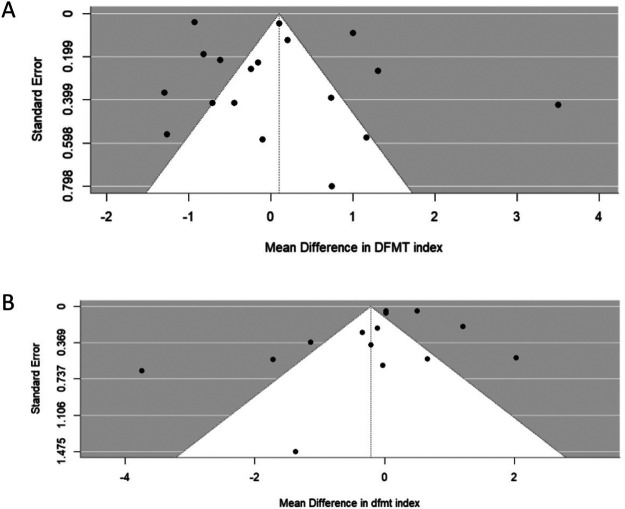 Figure 5
Figure 5| Database | Search Fields | Filters |
|---|---|---|
| PubMed | Title, Abstract, Keywords | Language: English, Russian |
| Human | ||
| Web of Science | Title, Abstract, Keywords | Language: English, Russian |
| Source Type: Articles | ||
| ScienceDirect | Title, Abstract, Keywords | Language: English |
| Document Type: Articles | ||
| Google Scholar | Title, Abstract, Keywords | Language: English |
| Document Type: Articles |
| PICOS framework | Inclusion | Exclusion |
|---|---|---|
| Population | Studies involving children aged 0–18 years | Studies involving adults with DS and ASD |
| Exposure | Studies involving children diagnosed with DS or ASD | Studies including children with co—occurring DS and ASD |
| Comparison | Studies reporting the outcomes of interest in DS vs. healthy controls and ASD vs. healthy controls | Studies on children with other neurodevelopmental disorders |
| Outcome | Studies reporting following outcome DFMT, dfmt, OHI-S, PI, GI | Studies reporting other outcomes on oral health |
| Study design | Case—control and cross—sectional with comparison group | RCT, review, case reports, congress abstracts, commentaries and editorials |
| Author, year | Question 1 | Question 2 | Question 3 | Question 4 | Question 5 | Question 6 | Question 7 | Total “Yes” score |
|---|---|---|---|---|---|---|---|---|
| Cross—sectional | ||||||||
| Habashneh, et al. ( | Yes | Yes | Yes | Yes | Yes | Yes | Can’t tell | 6 |
| Carrada, et al. ( | Yes | Yes | Yes | Yes | Yes | Yes | Can’t tell | 6 |
| Leiva-García, et al. ( | Yes | Yes | Yes | Yes | Can't tell | Yes | Yes | 6 |
| Kuter, et al. ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 7 |
| Dharmadhikari, et al. ( | Yes | Yes | Yes | Yes | Yes | Yes | Can't tell | 6 |
| Hamonari, et al. ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 7 |
| Case—control | ||||||||
| Lee, et al. ( | Yes | yes | Yes | Yes | yes | yes | Can’t tell | 6 |
| Jaber, et al. ( | Yes | Yes | Yes | Yes | Yes | Yes | Can’t tell | 6 |
| Areias, et al. ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 7 |
| Subramaniam, et al. ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 7 |
| Al—Maweri, et al. ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 7 |
| Khatib, et al. ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 7 |
| AlSarheed, et al. ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 7 |
| Fakroon, et al. ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 7 |
| Diab, et al. ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 7 |
| Ghaith, et al. ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 7 |
| Daneshvar, et al. ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 7 |
| Andreeva, et al. ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 7 |
| Bagattoni, et al. ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 7 |
| Moorthy, et al. ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 7 |
| Radzuan, et al. ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 7 |
| Narula, et al. ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 7 |
| Mahmood, et al. ( | Yes | Yes | Yes | Yes | Yes | Yes | Can’t tell | 6 |
| Prynda, et al. ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 7 |
| Last name, year | Design | Country | Age | Cases | Controls | Oral health data collected |
|---|---|---|---|---|---|---|
| Studies with DS patients | ||||||
| Lee, et al. ( | Case—control | Korea | 8–17 | 19 | 41 | OHI –S |
| Areias, et al. ( | Case—control | Portugal | 6–18 | 45 | 45 | DFMT, dfmt |
| Habashneh, et al. ( | Cross—sectional | Jordan | 12–16 | 103 | 103 | GI, DFMT |
| Subramaniam, et al. ( | Case—control | India | 7–12 | 34 | 34 | DFMT, dfmt |
| AlSarheed et al. ( | Case—control | Saudi Arabia | 7–15 | 93 | 99 | DFMT |
| Carrada, et al. ( | Cross—sectional | Brazil | 3–12 | 30 | 30 | PI |
| Ghaith, et al. ( | Case—control | United Arab Emirates | 4–18 | 84 | 112 | DFMT, dfmt, OHI |
| Andreeva, et al. ( | Case—control | Bulgaria | 3–15 | 60 | 60 | PI |
| Dharmadhikari, et al. ( | Cross—sectional | India | 4–14 | 25 | 25 | OHI –S |
| Hamonari, et al. ( | Cross—sectional | Iraq | 7–12 | 40 | 42 | DFMT, dfmt, PI,GI |
| Studies with ASD patients | ||||||
| Jaber, et al. ( | Case—control | United Arab Emirates | 6–18 | 61 | 61 | DFMT,dfmt |
| Al—Maweri, et al. ( | Case—control | Yemen | 5–18 | 42 | 84 | DFMT, PI,GI |
| Khatib, et al. ( | Case—control | Egypt | 3–13 | 100 | 100 | DFMT, PI, GI |
| Fakroon, et al. ( | Case—control | Libya | 3–14 | 50 | 50 | DFMT, dfmt |
| Diab, et al. ( | Case—control | Saudi Arabia | 4–15 | 50 | 50 | PI, GI |
| Daneshvar, et al. ( | Case—control | Iran | 6–12 | 55 | 165 | DFMT, dfmt |
| Leiva-García, et al. ( | Cross—sectional | Spain | 3–15 | 51 | 93 | DFMT, dfmt |
| Kuter, et al. ( | Cross—sectional | Turkey | 5–16 | 285 | 122 | DFMT, dfmt, PI |
| Bagattoni, et al. ( | Case—control | Italy | M ± SD = 9.0 ± 2.9 | 64 | 64 | DFMT, dfmt, PI |
| Moorthy, et al. ( | Case—control | India | 5–12 | 136 | 136 | DFMT, dfmt, PI |
| Radzuan, et al. ( | Case—control | Malaysia | 3–16 | 2.8 | 30 | DFMT, dfmt |
| Narula, et al. ( | Case—control | India | 5–14 | 80 | 80 | DFMT, dfmt |
| Mahmood, et al. ( | Case—control | Iraq | 5–12 | 45 | 45 | PI, GI |
| Prynda, et al. ( | Case—control | Poland | 3–12 | 74 | 74 | OHI -S |
| Outcome | Risk of Bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Certainty of Evidence |
|---|---|---|---|---|---|---|
| MD in PI score | Low | Serious | Not serious | Not serious | Not assessed | Low |
| MD in GI score | Low | Serious | Not serious | Serious | Not assessed | Low |
| MD in DFMT score | Low | Serious | Not serious | Serious | No | Low |
| MD in dfmt score | Low | Serious | Not serious | Serious | No | Low |
| MD in OHI – S score | Low | Serious | Not serious | Serious | Not assessed | Low |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Health and Care Utilization · Down syndrome and intellectual disability research · Autism Spectrum Disorder Research
Introduction
1
Down syndrome (DS) and Autism Spectrum Disorder (ASD) represent two of the most prevalent neurodevelopmental conditions in children. According to the World Health Organization, DS occurs in approximately 1 out of every 1,000–1,100 live births (1), whereas ASD is currently identified in about 1 in 100 children (2). Both are associated with lifelong cognitive, behavioral, and health challenges that require substantial healthcare resources (3–5). Overall, children with disabilities have poorer health than their non-disabled peers, and studies consistently show health disparities between these groups (6). In this context, children with DS and ASD have higher rates of oral health problems than typically developing peers (7, 8). A meta-analysis reported a high burden of oral diseases among children with ASD, with pooled prevalence estimates of 60.6% for dental caries and 69.4% for periodontal disease (9).
Children with DS often have a smaller midface and breathe through the mouth (10). Typical oral findings are open bite, a large-appearing tongue, cracks on the tongue and lips, late tooth eruption, small or misshapen teeth, missing teeth, a poor bite, and crowded teeth (11–14). These factors contribute to an increased risk of dental caries, periodontal disease, inflammation, and plaque accumulation (15, 16). Although ASD does not directly cause oral disease, affected individuals have elevated oral-health risk due to communication barriers, atypical sensory processing, and behavioral challenges that limit cooperation with hygiene and treatment (17, 18).
Moreover, children with neurodevelopmental disorders incur higher healthcare costs than their peers (19); dental care is often costlier due to frequent use of behavior management, sedation, or general anesthesia (20). A survey that included 40,840 children with special health care needs (SHCN) and 6,113 children without SHCN shows that they represent about 8.8 million and 61 million children nationally. Among children with SHCN, 81% needed preventive dental care and 24% needed other dental care in the past 12 months (21).
However, the literature regarding the oral health status of children with DS and ASD is conflicting and inconclusive. While some studies have reported higher rates of caries and plaque accumulation (22, 23), some investigations have paradoxically indicated that children with DS and ASD may exhibit fewer carious lesions and reduced dental plaque (24–26), and healthier gingival conditions (27) compared to their healthy counterparts.
In the existing literature, several systematic reviews and meta-analyses have assessed the oral health status of individuals with DS and ASD, including pediatric populations. With respect to DS, Martins et al. (25) conducted a systematic review and meta-analysis entitled “The Incidence of Dental Caries in Children with Down Syndrome,” which evaluated dental caries using the DMFT/dfmt indices and included studies published up to December 2020**.** In contrast, Scalioni et al. (28) performed a systematic review focusing on periodontal disease in patients with DS, with database searches conducted through March 2017**; this** review predominantly included case–control studies and did not undertake a quantitative meta-analysis. Furthermore, Deps et al. (29), in their systematic review and meta-analysis “Association between Dental Caries and Down Syndrome,” applied broader inclusion criteria that encompassed mixed-age populations, including individuals older than 18 years, thereby limiting the specificity of conclusions applicable to children.
Regarding ASD, Lam et al. (30) conducted a systematic review and meta-analysis examining the oral health status of children and adolescents with ASD, restricting inclusion to case–control studies published up to March 2018**.** Similarly, Silvana Nunes da Silva et al. (9), performed a systematic review and meta-analysis titled “Oral health status of children and young adults with autism spectrum disorders,” which evaluated oral health outcomes in individuals with ASD; however, the inclusion of young adults aged 18 years and older alongside pediatric populations constrains the applicability of findings specifically to children.
This inconsistency likely stems from non-standard outcome definitions**,** mixing of age groups**.** As a result, we still lack clear, comparable, age-stratified, and severity-focused estimates of oral health in these populations. Therefore, there is a need for an updated systematic review and meta-analysis that focuses exclusively on pediatric populations, applies standardized oral health outcome measures, and accounts for methodological heterogeneity across studies.
Understanding oral health status among children DS and ASD is essential for effectively promoting their oral health. The hypothesis guiding this review is that children with DS and ASD experience significantly poorer oral health outcomes than their healthy counterparts. This study aims to systematically review the literature and conduct meta-analysis to address the evidence gap, involving children aged 0–18 years with DS or ASD that report standardized outcomes.
Materials and methods
2
Study registration
2.1
The review protocol was submitted to PROSPERO (ID: CRD420251155866) on 26 September 2025, after confirming that no similar reviews existed.
Search strategy
2.2
Before conducting the comprehensive search the PROSPERO data base was searched, and no similar reviews were found.
The following databases were searched: PubMed, Web of Science, Science Direct, Google Scholar, Other sources, including manual searching of references (Table 1). Filters applied included publication in English and Russian, publication in scholarly journals, and document types limited to articles, research articles, and early access articles. No restrictions were placed on the year of publication.
To define the search terms, a preliminary search was conducted in PubMed to identify relevant keywords from the titles and abstracts of studies focusing on the prevalence of oral health conditions specifically oral hygiene, dental caries, and related indices among pediatric populations with DS and ASD.
Based on this initial exploration, the following keywords were used in the final search strategy: “oral health” OR “oral hygiene” OR “dental caries” OR “tooth decay” OR “plaque index” OR “gingival index” OR “OHI-S” OR “DMFT” OR “dmft” OR “Down Syndrome” OR “Trisomy 21” OR “Autism Spectrum Disorder” OR “autistic children” OR “children” OR “pediatric” OR “healthy children” OR “neurotypical”.
Eligibility criteria, study selection and data collection
2.3
Table 2 presents the eligibility criteria used to select articles in accordance with the Population, Exposure, Comparator, Outcome, and Study Design (PECOS) framework.
The population criterion included studies involving children aged 0–18 years with DS and ASD**,** while studies focusing on adults with DS and ASD were excluded. Regarding exposure**,** only studies on children diagnosed with DS or ASD**,** were included. Studies involving children with co—occurring DS and ASD were excluded.
In terms of comparison, the review included studies that assessed outcomes in children with DS or ASD compared to healthy children. Studies that other neurodevelopmental disorders were excluded.
The outcome criteria focused on oral health indicators, including DFMT (dental caries experience in permanent teeth), dfmt (dental caries in primary teeth), OHI-S (Simplified Oral Hygiene Index), PI (Plaque Index), and GI (Gingival Index). Studies reporting other unrelated oral health outcomes were excluded.
Finally, eligible study designs included case–control and cross-sectional studies with a comparison group. Excluded study types were randomized controlled trials (RCT), reviews, case reports, conference abstracts, commentaries, and editorials.
The eligibility assessment and data collection were conducted in accordance with the PRISMA guidelines (31). Two independent reviewers (K.Zh. and N.B.) carried out a standardized literature search across all relevant databases. The search results were compiled in Mendeley, and duplicates were removed. Only unique records were then screened for relevance based on their titles and abstracts. In the next stage of eligibility assessment, full-text articles were reviewed against the inclusion and exclusion criteria outlined in Table 2, based on the PECOS framework. This review was carried out independently by both reviewers. Standardized data extraction forms were developed in advance, informed by preliminary search findings.
Data collection form included the following information: first author's last name, year of publication, country, study design, mean age of participants, neurodevelopmental condition (DS or ASD), comparator group (neurotypical children), and the reported mean values and standard deviations for oral health outcomes, including DFMT, dfmt, OHI-S, PI, and GI. Two independent data extraction sheets were compared and merged in the final stage. Any discrepancies in study selection or data interpretation were resolved through discussion with a third reviewer (N.J.), and full consensus was achieved for all included studies.
Meta-analysis
2.4
The meta-analysis of pooled mean differences was conducted using RStudio (version 2024.12.1.563) with R (version 4.3.2, released 2023-10-31) (32). We calculated pooled mean differences for five clinical indices (DMFT, dmft, OHI-S, PI, and GI) to compare outcomes between (1) children with DS and healthy controls, and (2) children with ASD and healthy controls. Analyses were performed using the meta and metafor packages. A random-effects model, based on the DerSimonian–Laird estimator, was employed to derive pooled mean differences with 95% confidence intervals. Forest plots were generated to visually represent the pooled mean differences. Heterogeneity was assessed using the I^2^ statistic, and potential moderating factors were investigated via meta-regression based on the year of publication. Sensitivity analyses were conducted using leave-one-out resampling to evaluate the robustness of the findings. Publication bias was assessed through funnel plot asymmetry and Egger's regression test for outcomes with at least ten studies. Finally, subgroup analyses were performed separately for DS vs. control and ASD vs. control comparisons to identify group-specific effects.
Risk of bias
2.5
The risk of bias (quality) assessment was conducted using the Mixed Methods Appraisal Tool (MMAT), which is specifically designed to appraise the methodological quality of qualitative, quantitative, and mixed-methods studies. For this review, we applied the quantitative descriptive criteria from the MMAT (version 2018) (33), appropriate for evaluating cross-sectional studies and case-control studies.
Each included study was assessed according to the following seven MMAT criteria**:**
- Are the research questions well-defined?
- Can the research questions be addressed using the data that has been gathered?
- Does the sample plan adequately answer the research question?
- Does the sample accurately reflect the intended audience?
- Are the measurements accurate, valid, and trustworthy?
- Is there little chance of nonresponse bias?
- Can the research question be addressed by the statistical analysis? Each criterion was rated as “Yes”, “No”, or “Can't tell” based on the reported methods and results in each article. Two reviewers independently performed the assessments after reaching consensus on the evaluation procedures. Any disagreements were resolved through discussion with a third reviewer.
Although the MMAT does not recommend computing an overall score, we report the total number of “Yes” ratings for transparency. Studies that met at least 5 out of 7 criteria with a “Yes” rating were considered to be of satisfactory quality and were included in the final synthesis. The detailed results of the quality assessment for all included studies are presented in Table 3.
Certainty of evidence evaluation
2.6
Adhering to the guidelines from the Cochrane Handbook for Systematic Reviews of Interventions, we assessed the certainty of evidence using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework (58). Furthermore, this assessment followed the procedures outlined in research notes on the evaluation of GRADE in systematic reviews (59). Certainty of evidence was calculated in RStudio, using the “GRADE” package. This framework comprises five domains: Risk of Bias, assessed using the MMAT scores mentioned above; Inconsistency, assessed via the I^2^ statistic; Indirectness, assessed via PECOS criteria; Imprecision, assessed by determining if the 95% CI of the pooled estimate crosses the threshold of interest; and Publication Bias, assessed using Egger's test results.
Results
3
Study selection and characteristics of the included studies
3.1
A comprehensive search across PubMed, Web of Science, Google Scholar and ScienceDirect databases identified 1,324 records**.** After removing duplicates, 1,002 titles and abstracts were screened, of which 151 articles were selected for full-text evaluation. Following a full-text assessment, 24 studies met the PICOS eligibility criteria and were included in the meta-analysis. A total of 126 studies were excluded, including six that did not include healthy control groups for comparison with patients with DS. References for these six excluded studies are provided (60–63). The PRISMA flowchart illustrating the study selection and inclusion process is presented in Figure 1 (31).
PRISMA flowchart of study inclusion.
The 24 included studies originated from a diverse range of countries. Ten studies focused on children with DS, while 14 investigated children with ASD, each compared to age-matched healthy control group. The majority of studies were conducted in Asia. In total, 527 children with DS, 1,221 children with ASD, and 1,875 controls were assessed. Participant ages ranged from 3 to 18 years**.** Various oral health indicators were collected from each study. Detailed study characteristics are presented in Table 4.
Meta-analysis results
4
Figure 2 presents the pooled mean difference analysis of oral health indices among children with DS and ASD compared to healthy controls. Panel A illustrates the mean difference in PI scores between children with DS (five studies) and those with ASD (seven studies) relative to healthy peers. In the DS subgroup, the pooled mean difference was 0.53 (95% CI: −0.13–1.18), maintaining high heterogeneity (I^2^ = 90%, p < 0.0001), while in the ASD subgroup, the pooled mean difference in PI scores was 0.28 (95% CI: −0.05–0.61), with high heterogeneity (I^2^ = 93.3%, p < 0.0001).
Meta-analysis of oral health Status among children with DS, ASD, and their healthy controls: (A) PI; (B) GI; (C) DFMT; (D) dfmt; (E) OHI – S. DFMT, dental caries experience for permanent teeth; dfmt, dental caries experience for primary teeth; OHI-S, simplified oral hygiene index; PI, plaque index; GI, gingiva index; DS, down syndrome; ASD, autism spectrum disorder. Group definitions: Kuter, 2019 (A): 5–11 years (37); Kuter, 2019 (B): 12–16 years (37). Andreeva, 2020 (A): 3–6 years (51), Andreeva, 2020 (B): 6–12 years (51), Andreeva, 2020 (C): 12–14 years (51).
Panel B shows the mean difference in GI between children with DS (two studies) and those with ASD (four studies) relative to healthy peers. In the DS subgroup, the pooled mean difference was 12.10 (95% CI: −0.138.72–162.92), maintaining heterogeneity (I^2^ = 99.7%, p < 0.0001), while in the ASD subgroup, the pooled mean difference in GI scores was 0.33 (95% CI: −0.13–0.78), with high heterogeneity (I^2^ = 93.1%, p < 0.0001).
Panel C shows the mean difference in DFMT index between children with DS (six studies) and those with ASD (twelve studies) relative to healthy peers. In the DS subgroup, the pooled mean difference was −0.29 (95% CI: −0.97–0.39), maintaining high heterogeneity (I^2^ = 54.7%, p < 0.05), while in the ASD subgroup, it was 0.29 (95% CI: −0.53–1.11), with high heterogeneity (I^2^ = 97.6%, p < 0.0001).
Panel D shows the mean difference in dfmt index between children with DS (four studies) and those with ASD (ten studies) relative to healthy peers. In the DS subgroup, the pooled mean difference was −0.14 (95% CI: −0.61–0.33), maintaining homogeneity (I^2^ = 0%, p < 0.39), while in the ASD subgroup, it was −0.33 (95% CI: −1.49–0.82), with high heterogeneity (I^2^ = 94.6%, p < 0.0001).
Panel E shows the mean difference in OHI-S index between children with DS (three studies) and those with ASD (two studies) relative to healthy peers. In the DS subgroup, the pooled mean difference was 0.28 (95% CI: −0.92–1.47), (I^2^ = 92.2%, p < 0.0001), while in the ASD subgroup, it was 0.31 (95% CI: −1.37–1.98), with heterogeneity (I^2^ = 65.7%, p < 0.08).
The results of the meta-regression of oral health status among children with DS and ASD based on the year of publication are presented in Figure 3. In the meta-regression analysis, no significant associations were found between the year of publication and any of the oral health indices analyzed: (A) PI (p = 0.3991), (B) GI (p = 0.3075), (C) DMFT (p = 0.6679), (D) dmft (p = 0.4322), (E) OHI–S (p = 0.4005).
Meta-regression of the the oral health Status by the year of pubication among children with DS, ASD and healthy children (A) PI; (B) GI; (C) DFMT; (D) dfmt; (E) OHI – S. DFMT, dental caries experience for permanent teeth; dfmt, dental caries experience for primary teeth; OHI-S, simplified oral hygiene index; PI, plaque index; GI, gingiva index; DS, down syndrome; ASD, autism spectrum disorder.
Sensitivity analyses are summarized in Figure 4. In Plot A (Plaque Index), one study, Mahmood, 2024 (56), showed a significant influence on the overall effect size. Its exclusion altered the effect to 0.43 (0.17–0.70), p = 0.0047, with heterogeneity reduced to 88.5%. In Plots B–E (Gingival Index, DMFT, dmft, OHI–S), no single study significantly impacted the overall results.
Sensitivity analysis of the oral health Status among children with DS, ASD and healthy children: (A) PI; (B) GI; (C) DFMT; (D) dfmt; (E) OHI – S. DFMT, dental caries experience for permanent teeth; dfmt, dental caries experience for primary teeth; OHI-S, simplified oral hygiene index; PI, plaque index; GI, gingiva index; DS, down syndrome; ASD, autism spectrum disorder. Group definitions: Kuter, 2019 (A): 5–11 years (37); Kuter, 2019 (B): 12–16 years (37). Andreeva, 2020 (A): 3–6 years (51), Andreeva, 2020 (B): 6–12 years (51), Andreeva, 2020 (C): 12–14 years (51).
Publication bias assessment results are presented in Figure 5 (Panels A,B). For the DMFT and dmft indexes, the funnel plots appeared symmetrical, and Egger's test results were non-significant (p = 0.5466 and p = 0.1597, respectively), indicating no evidence of publication bias. However, for the PI, GI, and OHI-S indexes, fewer than 9 articles were included, and therefore, publication bias assessment was not performed.
Publication bias assessment.
The certainty of evidence assessment results for all pooled estimates are detailed in Table 5, based on the GRADE framework. The five meta-analytic outcomes incorporated data from case—control and cross—sectional analysis. Risk of bias was low across all outcomes. Inconsistency was judged “serious” for every outcome, whereas indirectness was considered “not serious.” Imprecision was serious for GI, DMFT, dmft, and OHI-S, but not for PI. Publication bias was not present for DMFT and dmft, while it was not assessed for PI, GI, and OHI-S because fewer than nine studies were available. Overall, the certainty of evidence was rated as low for all five pooled outcomes.
Discussion
5
Our systematic review and meta-analysis yielded several key findings regarding oral health indices in children. First, contrary to our initial hypothesis that neurodevelopmental disorders would be associated with poorer oral health outcomes in children with DS and ASD, the results indicated no statistically significant differences compared with healthy peers for the following indices: GI, DMFT, dmft, and OHI-S. Second, sensitivity analyses largely confirmed the robustness of these findings, with the exception of one influential study affecting the PI estimates. Furthermore, no evidence of substantial publication bias was identified in analyses where formal assessment was feasible.
Our findings contribute to the broader literature on oral health disparities among children with neurodevelopmental conditions. Firouzeh N. et al. (64) previously reported significantly higher PI and GI scores in individuals with DS compared to healthy controls. In contrast, our subgroup analysis of children with DS did not reveal statistically significant differences in these indices, although the pooled estimate for the combined DS and ASD group did suggest elevated PI. One plausible explanation for this discrepancy may be the influence of age-related changes in oral hygiene behaviors and dental health outcomes, which tend to converge across populations as children mature. This interpretation is supported by prior studies indicating that DS does not significantly affect DMFT scores (8, 29). Similarly, Flávia et al. (11) found no significant difference in OHI between individuals with DS and healthy controls.
Regarding children with ASD, two meta-analyses have reported that, compared with their neurotypical peers, children with ASD tend to have poorer oral hygiene and greater susceptibility to dental caries (65, 66). Da Silva et al. (9) and Magdalena et al. (57) found that the prevalence of dental caries and periodontal disease in children and young adults with ASD can be considered high compared with healthy children. Similarly, Xiaoqin et al. (67) reported a higher mean DMFT, as well as higher PI and GI, in children with ASD compared to healthy controls suggesting that children with ASD have poorer oral hygiene, and higher risk of caries. Our findings showing no significant difference in GI, DMFT, dmft, or OHI-S scores contrast with some prior literature due to factors like the heterogeneity of included studies.
However, some studies have produced controversial results. For example, a few investigations reported lower caries prevalence in children with ASD compared to healthy controls (68, 69). Robertson et al. (70) reported no significant difference in dental caries levels between children with learning disabilities and their neurotypical peers, but subgroup analysis revealed lower caries levels in permanent teeth among children with DS and ASD. Such discrepancies may reflect differences in study populations, diagnostic criteria, dietary patterns, or preventive dental care.
Socioeconomic status also plays a critical role in shaping oral health outcomes. According to Costacurta et al. (71), healthy children under 12 years of age from families with very low income (<€6,000) exhibited significantly higher DMFT scores compared with those from higher-income households (>€20,000), underscoring the strong link between economic disadvantage and oral health. Cultural differences may also influence oral health outcomes. For instance, Zhang et al. (17) found that Asian children with ASD had significantly higher dmft scores compared with their non-Asian counterparts. This disparity may reflect the influence of cultural and socioeconomic determinants such as parental attitudes toward oral health, and societal stigma related to disability which collectively contribute to poorer oral health outcomes among Asian children with ASD (72).
In our study, the absence of significant differences across most oral health indicators for children with DS and ASD may reflect the complex interplay of multiple factors influencing oral health in these populations. These include caregiver involvement, socioeconomic conditions, access to dental services, and behavioral challenges. Furthermore, barriers to care—such as practitioners' limited confidence and specialized training, restricted access to specialist services, and inadequate behavioral or communication support during treatment may contribute to unmet oral health needs (73, 74).
This review has several limitations, including substantial heterogeneity, the overall low certainty of evidence, and reliance on case–control and cross-sectional study designs. Therefore the findings of our study should be interpreted with caution. The lack of statistically significant differences in some oral health indices between children with learning disabilities and neurotypical children does not eliminate the need for targeted interventions. Instead, it highlights persistent barriers to care. From a practical perspective, the observed disparities in PI indicators underscore the need to strengthen care delivery and address systemic barriers. Public health initiatives should focus on inclusive, community-based programs that integrate oral health education into family support systems, expand provider training in special care dentistry, and ensure equitable access to preventive and therapeutic services. These efforts are crucial to reducing oral health disparities and promoting long-term well-being among children with neurodevelopmental disorders.
Future research should focus on improving study design and evidence quality, particularly through longitudinal studies, and should examine how socioeconomic status, cultural background, and dentists' experience influence the evaluation of oral health indices.
This review found that children with DS and ASD generally tend to have no consistent differences in oral health indicators such as PI, GI, DMFT, dmft, or OHI-S scores. The absence of consistent differences in certain indices does not reduce the importance of addressing oral health needs in these populations. Public health strategies should prioritize inclusive oral health education, improved provider training, and equitable access to dental services to achieve better outcomes for children with neurodevelopmental disorders.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chen L Wang L Wang Y Hu H Zhan Y Zeng Z Global, regional, and national burden and trends of down syndrome from 1990 to 2019. Front Genet. (2022) 13:908482. 10.3389/FGENE.2022.90848235910218 PMC 9337874 · doi ↗ · pubmed ↗
- 2Zeidan J Fombonne E Scorah J Ibrahim A Durkin MS Saxena S Global prevalence of autism: a systematic review update. Autism Res. (2022) 15:778–90. 10.1002/AUR.269635238171 PMC 9310578 · doi ↗ · pubmed ↗
- 3Antonarakis SE Skotko BG Rafii MS Strydom A Pape SE Bianchi DW Down syndrome. Nat Rev Dis Prim. (2020) 6:9. 10.1038/S 41572-019-0143-732029743 PMC 8428796 · doi ↗ · pubmed ↗
- 4Lord C Elsabbagh M Baird G Veenstra-Vanderweele J. Autism spectrum disorder. Lancet (London, England). (2018) 392:508–20. 10.1016/S 0140-6736(18)31129-230078460 PMC 7398158 · doi ↗ · pubmed ↗
- 5Junnarkar VS Tong HJ Hanna KMB Aishworiya R Duggal M. Qualitative study on barriers and coping strategies for dental care in autistic children: parents’ perspective. Int J Paediatr Dent. (2023) 33:203–15. 10.1111/IPD.1303536271894 · doi ↗ · pubmed ↗
- 6Allerton LA Welch V Emerson E. Health inequalities experienced by children and young people with intellectual disabilities: a review of literature from the United Kingdom. J Intellect Disabil. (2011) 15:269–78. 10.1177/174462951143077222129526 · doi ↗ · pubmed ↗
- 7Anders PL Davis EL. Oral health of patients with intellectual disabilities: a systematic review. Spec Care Dentist. (2010) 30:110–7. 10.1111/J.1754-4505.2010.00136.X 20500706 · doi ↗ · pubmed ↗
- 8da Silva MCPM Lyra MCA de Almeida HCR de Alencar Filho AV Heimer MV Rosenblatt A. Caries experience in children and adolescents with down syndrome: a systematic review and meta-analysis. Arch Oral Biol. (2020) 115:104715. 10.1016/j.archoralbio.2020.10471532422361 · doi ↗ · pubmed ↗