Impact of smoking on immune feature and prognosis in unresectable stage III anaplastic lymphoma kinase positive non-small-cell lung cancer
Ying Jiang, Zhihui Zhang, Jianzhong Cao, Jianchun Duan, Tao Zhang, Yu Wang, Weihua Li, Fengwei Tan, Jianming Ying, Nan Bi

TL;DR
Smoking worsens survival in ALK-positive lung cancer patients by affecting immune features, suggesting a need for tailored treatment strategies.
Contribution
This study identifies smoking as an independent prognostic factor affecting survival and immune features in ALK-positive NSCLC patients.
Findings
Smokers had significantly poorer overall survival compared to never-smokers.
CRT improved locoregional-free survival in these patients.
Smoking modulates the tumor immune microenvironment, affecting immune cell infiltration and interactions.
Abstract
Smoking is the primary risk factor for lung cancer, and 37% - 42% of patients with non-small-cell lung cancer (NSCLC) harboring anaplastic lymphoma kinase (ALK) mutation being smokers. Nevertheless, the specific impact of smoking on prognosis in patients with unresectable stage III ALK-positive NSCLC remains to be elucidated. This two-centric, retrospective cohort study included 48 patients with unresectable stage III ALK-positive NSCLC. Gene ontology (GO) enrichment analysis was conducted on data from 25 patients who underwent NGS. We further performed Gene Set Enrichment Analysis (GSEA) and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway analysis to validate these findings, using the GSE31852 dataset (n = 34) patients from the Gene Expression Omnibus (GEO) database. In these 48 patients, the median age was 55.2 (range, 33-80) years; approximately half of the patients were men…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
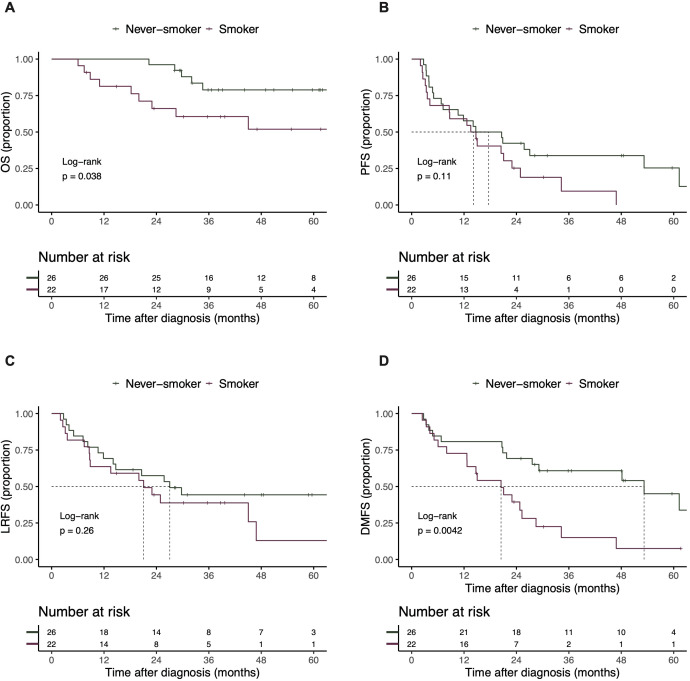 Figure 1
Figure 1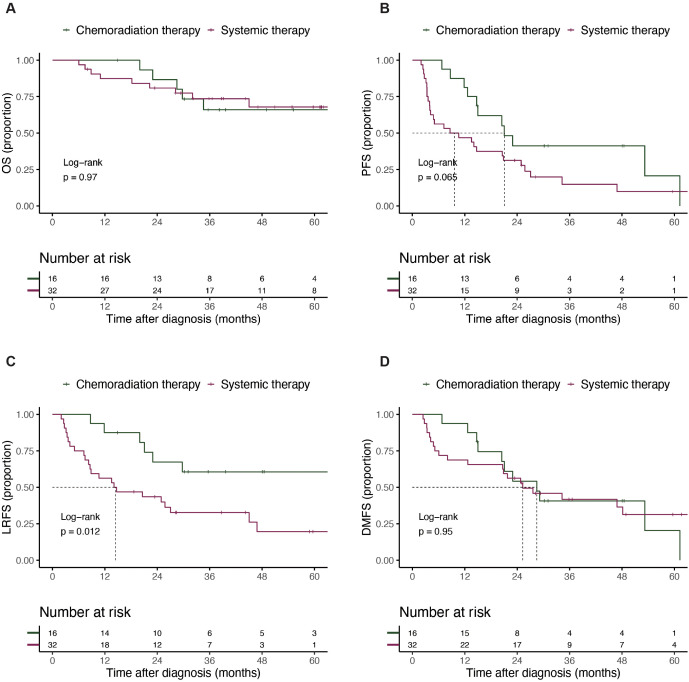 Figure 2
Figure 2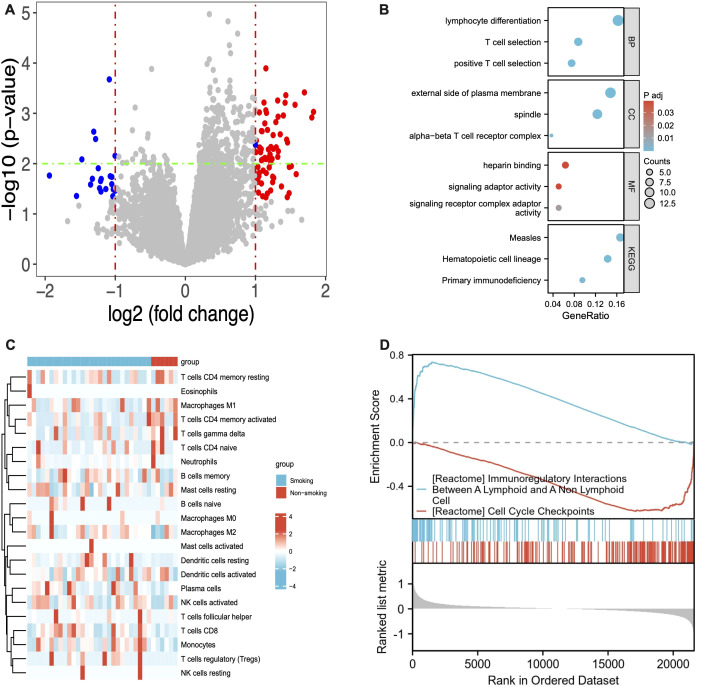 Figure 3
Figure 3| Characteristics |
|
|---|---|
| Age (range) | 55.2 (33-80) |
| Sex: | |
| Woman | 24 (50.0%) |
| Man | 24 (50.0%) |
| ECOG PS: | |
| 0 | 20 (41.7%) |
| 1 | 28 (58.3%) |
| Smoking: | |
| No | 26 (54.2%) |
| Yes | 22 (45.8%) |
| Stage: | |
| IIIA | 12 (25.0%) |
| IIIB | 30 (62.5%) |
| IIIC | 6 (12.5%) |
| Histological type: | |
| Adenocarcinoma | 45 (93.8%) |
| Non-adenocarcinoma | 3 (6.25%) |
| V3 | 14 (29.2%) |
| Others | 14 (29.2%) |
| Unknown | 20 (41.7%) |
| Treatment: | |
| Chemoradiation therapy | 16 (33.3%) |
| Sequential chemoradiation therapy | 6 (12.5%) |
| Concurrent chemoradiation therapy | 10 (20.8%) |
| Systemic therapy | 32 (66.7%) |
| Characteristics | Univariate analysis | Multivariate analysis* | ||||
|---|---|---|---|---|---|---|
| HR | CI |
| aHR | CI |
| |
| Age | ||||||
| 1 | 1 | |||||
| 0.43 | 0.12 – 1.54 | 0.193 | 0.47 | 0.11 – 2.02 | 0.313 | |
| ECOG PS | ||||||
| 0 | 1 | |||||
| 1 | 1.06 | 0.35 – 3.16 | 0.919 | |||
| Smoker | ||||||
| No | 1 | 1 | ||||
| Yes | 3.01 | 1.01 – 9.02 | 0.049 | 3.92 | 1.21 - 12.73 | 0.023 |
| Stage | ||||||
| IIIA | 1 | |||||
| IIIB | 0.18 | 0.06 – 0.53 | 0.002 | |||
| IIIC | 0 | 0 – Inf | ||||
| Treatment | ||||||
| CRT | 1 | 1 | ||||
| Systemic therapy | 0.98 | 0.33 – 2.92 | 0.969 | 1.16 | 0.36 – 3.73 | 0.801 |
| EML4-ALK | ||||||
| Others | 1 | |||||
| V3 | 2.66 | 0.52 – 13.73 | 0.244 | 1.94 | 0.35 – 10.79 | 0.447 |
| Unknown | 3.73 | 0.77 – 18.10 | 0.102 | 3.05 | 0.53 – 17.40 | 0.211 |
| Characteristics | Univariate analysis | Multivariate analysis* | ||||
|---|---|---|---|---|---|---|
| HR | CI |
| aHR | CI |
| |
| Age | ||||||
| 1 | ||||||
| 1.24 | 0.65 – 2.36 | 0.515 | ||||
| ECOG PS | ||||||
| 0 | 1 | |||||
| 1 | 0.78 | 0.41 - 1.49 | 0.451 | |||
| Smoker | ||||||
| No | 1 | |||||
| Yes | 1.72 | 0.88 – 3.33 | 0.111 | 1.64 | 0.83 - 3.24 | 0.154 |
| Stage | ||||||
| IIIA | 1 | |||||
| IIIB | 0.55 | 0.27 – 1.15 | 0.113 | 0.38 | 0.16 – 0.91 | 0.029 |
| IIIC | 0.78 | 0.27 – 2.28 | 0.653 | 0.38 | 0.11 – 1.31 | 0.125 |
| Treatment | ||||||
| CRT | 1 | |||||
| Systemic therapy | 1.92 | 0.95 – 3.89 | 0.069 | 3.04 | 1.32 – 7.01 | 0.009 |
| EML4-ALK | ||||||
| Others | 1 | |||||
| V3 | 1.44 | 0.62 – 3.36 | 0.393 | |||
| Unknown | 1.49 | 0.67 – 3.33 | 0.332 | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · Cancer Immunotherapy and Biomarkers · Lung Cancer Diagnosis and Treatment
Introduction
Lung cancer is the leading cause of death worldwide, with non-small-cell lung cancer (NSCLC) accounting for 85% of all lung cancer (1). Anaplastic lymphoma kinase (ALK) rearrangements are found in approximately 5% of NSCLC (2). The proportion of smokers among patients with ALK-positive NSCLC is slightly higher than that among those with EGFR-mutated NSCLC, although approximately 37–42% of ALK-positive patients are current or former smokers (3–11). Previous molecular epidemiology studies have demonstrated distinct mutation patterns and frequencies between smokers and never-smokers with NSCLC, including differences in TP53, KRAS, and EGFR mutations (12, 13). It is therefore important to identify the impact of smoking on unresectable stage III ALK-positive NSCLC.
The introduction of ALK tyrosine kinase inhibitors (TKIs) has substantially improved survival in advanced-stage disease. Smoking status does not appear to significantly efficacy of first-line treatment (14). Although ALK TKIs have been evaluated in resectable disease in several recent clinical trials (15, 16), evidence in unresectable stage III ALK-positive NSCLC remains limited. Currently, chemoradiotherapy (CRT) and immunotherapy remain the standard treatment for patients with unresectable stage III NSCLC who have good performance status (17). However, due to exclusion of ALK-positive NSCLC in the majority of clinical trials and poor outcomes of immunotherapy in ALK-positive NSCLC, the optimal treatment for stage III ALK-positive unresectable NSCLC remains unclear. The clinical characteristics and prognosis of these patients have been rarely reported, leaving limited evidence to guide clinical practice.
In this study, we aimed to evaluate the clinical outcomes and the impact of smoking on unresectable stage III ALK-positive NSCLC.
Methods
Patients
This two-centric, retrospective cohort study included patients who met the following criteria: pathologically unresectable stage III NSCLC; ALK-positive status was identified by one of Ventana D5F3 immunohistochemistry (IHC), fluorescent in situ hybridization (FISH), reverse transcription-polymerase chain reaction (RT-PCR) or next-generation sequencing (NGS); and adequate follow-up data. The follow-up period ranged from the date of diagnosis to either the last follow-up or death. Participants were followed every 6 months through clinic visits or telephone interviews.
Patients were categorized into two treatment groups: the definitive radiation therapy (RT) group and the systemic therapy group. Definitive RT was defined as volumetric modulated arc therapy (VMAT) or intensity-modulated radiation therapy (IMRT) with a prescribed dose of 60–70 Gy, delivered sequentially or concurrently with at least two cycles of platinum-based doublet chemotherapy. The systemic therapy group comprised patients who were unsuitable for definitive RT or those who refused it, opting for drug therapy as their initial treatment.
Detection of gene mutation and identification of ALK variant
NGS was used to detect the ALK rearrangements. EML4-ALK v3 was defined as the fusion of exon 6a/b in EML4 to exon 20 in ALK, while non-EML4-ALK v3 variants included other EML4–ALK fusions (e.g., EML4–ALK v1, v2) and additional ALK fusion partners such as TMEM178A-ALK and KCNK2-ALK. Co-mutation was defined as ALK-positive status combined with other mutation, such as EGFR and BRCA2. Gene ontology (GO) enrichment analysis was performed on data from 25 patients who underwent NGS.
Enrichment analysis
GO enrichment analysis was performed to investigate the cellular functions of smoking-related genes. Smoking-related genes were defined as differentially expressed genes between smokers and never-smokers in the GSE31852 cohort, with an absolute log2 fold change (|log2FC|) > 2 and P < 0.05, yielding 89 genes. The Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway enrichment analysis was performed. Analysis was conducted using the online Database for Annotation, Visualization, and Integrated Discovery (DAVID 6.8, https://david.ncifcrf.gov/) to explore the potential biological roles of smoking-related genes. Gene set variation analysis (GSVA) was performed using R 3.5.1 to estimate variation in gene set enrichment according to the expression data, using the GSE31852 dataset (n = 34) from the Gene Expression Omnibus (GEO) database. The GSVA package was freely available at http://www.bioconductor.org.
Statistical analysis
Progression-free survival (PFS), locoregional-free survival (LRFS), distant metastasis-free survival (DMFS), and overall survival (OS) were defined as the time from diagnosis to disease progression or death, locoregional recurrence or death, distant recurrence or death, and death, respectively. Kaplan–Meier curves were used to estimate survival outcomes. Baseline characteristics between the groups were compared using the Chi-square test or Fisher’s exact test for categorical variables, as appropriate. Landmark analysis was employed to reduce the impact of long-term events on outcomes. Univariate and multivariate regression analyses were carried out using a Cox proportional hazards model, and covariates with P<0.2 in the univariate analysis were included in the multivariate analysis. All statistical analyses were performed using R software (version 4.3.2), with two-sided P < 0.05 was considered statistically significant.
Results
Patients characteristics
A total of 48 patients with stage III unresectable ALK-positive NSCLC met the eligibility criteria and were included in the analysis (Supplementary Figure S1). The baseline characteristics of patients are summarized in Table 1. The median age was 55.2 (33–80) years; almost half of the patients were men (50.0%) and current or former smokers (45.8%); 62.5% had stage IIIB disease; most patients (93.8%) had adenocarcinoma; all patients had an Eastern Cooperative Oncology Group performance status (ECOG PS) of 0-1. 16 (33.3%) patients received definitive CRT as the initial treatment; 14 (29.2%) patients had EML4-ALK v3 status. Regarding treatment-related toxicities, pneumonitis was observed in 6/16 patients in the RT group, including one case of grade 3 case.
Survival analysis and first failure pattern
The median follow-up time for the entire cohort was 49.02 (interquartile range [IQR], 35.84 -62.03) months. The 1-, 3-, 5-year OS, and median OS for all patients were 91.6% (95% confidence interval [CI]: 84.0% - 99.8%), 70.7% (95% CI: 58.4% - 85.6%), 67.0% (53.8% - 83.4%) and not reached, respectively; the 1-, 3-, 5-year PFS, and median PFS was 58.3% (95% CI: 45.9% - 74.1%), 24.1% (95% CI: 14.0% - 41.4%), 15.1% (95% CI: 6.7% - 35.8%) and 14.7 months (95% CI: 10.6-24.9), respectively (Supplementary Figure S2). Compared with systemic therapy, the Kaplan-Meier curves showed that CRT improved the mPFS (21.1 vs. 9.6 months, P = 0.065; Figure 1B) and mLRFS (NA vs. 14.4 months, P = 0.012; Figure 1C). In contrast, no significant difference was observed in OS or DMFS between the CRT and systemic therapy. Subsequently, we examined the effect of smoking status on OS, PFS, LRFS, and DMFS (Figure 2). The 5-year OS rate was significantly higher in the never-smokers group at 78.9% (95% CI: 63.9% - 97.3%) compared to 51.9% (95% CI: 32.6% - 82.8%) in the smokers group (P = 0.038; Figure 2A). Similar trends were observed for DMFS, with a 5-year DMFS of 45.0% (95% CI: 26.6% - 76.4%) versus 7.5% (95% CI: 1.2% - 45.6%) in the never-smokers and smokers groups, respectively (P = 0.004; Figure 2D).
Kaplan-Meier curves for the OS (A), PFS (B), LRFS (C) and DMFS (D) between CRT group and systemic therapy group. OS, overall survival; PFS, progression-free survival; LRFS, locoregional free survival; DMFS, distant metastasis-free survival; CRT, chemoradiation therapy.
Kaplan-Meier curves for the OS (A), PFS (B), LRFS (C) and DMFS (D) between never-smokers group and smokers group. OS, overall survival; PFS, progression-free survival; LRFS, locoregional free survival; DMFS, distant metastasis-free survival.
As summarized in Supplementary Table S2, 77.1% of patients had relapsed. 15 (31.3%) patients had distant recurrence only and 13 (27.1%) patients had locoregional and distant recurrence simultaneously. Brain (14/28) was the most common metastasis site. Compared with systemic therapy, CRT significantly decreased the locoregional recurrence rate (18.8% vs. 59.4%, P = 0.018, Supplementary Table S2).
Univariate and multivariate Cox regression analysis for PFS and OS
The univariate Cox regression analysis revealed that smoking status (hazard ratio [HR] = 3.01, 95% CI: 1.01 - 9.02, P = 0.049) and stage (IIIB vs. IIIA, HR = 0.18, 95% CI: 0.06 - 0.53, P = 0.002) were significantly associated with OS (Table 2). In the univariate Cox regression analysis, the variable stage IIIC produced an infinite HR due to the absence of observed deaths in this category, which this variable was excluded from the multivariate Cox regression analysis to ensure model stability and reliability. In the multivariate Cox regression analysis, after adjusting for confounders, smoking status (HR = 3.92, 95% CI: 1.21 - 12.73, P = 0.023) remained a significant predictor of OS (Table 2), indicating smoking status was the independent prognostic factor for OS in stage III ALK-positive NSCLC. As for PFS (Table 3), univariate COX analysis suggested that patients who received systemic therapy tended to have a poorer PFS (HR = 1.92, 95%CI 0.95 - 3.89 P = 0.069). However, after adjusting for potential confounders (Covariates with P<0.2 in the univariate analysis) in the multivariate analysis, treatment was found to be significantly associated with PFS (aHR: 3.04, 95% CI: 1.32 - 7.01, p = 0.009), which indicates CRT exerts a significant effect on PFS when accounting for other covariates.
GO and pathway enrichment analysis in smokers vs. non-smokers
To further investigate the differences between smokers and never-smokers, we performed GO analyses. As illustrated in Supplementary Figure S3, the results revealed distinct revealed distinct enrichment patterns. For biological processes (BP), never-smokers exhibited enrichment in peptidyl-tyrosine modification, positive regulation of kinase activity, and peptidyl-tyrosine phosphorylation, whereas smokers showed enrichment in gland development, epithelial cell proliferation, and regulation of the mitotic cell cycle. In terms of cellular components (CC), never-smokers were enriched in transcription repressor complex, transcription regulator complex, and PML body, whereas smokers were enriched in chromosome, telomeric region, DNA repair complex, and PML body. For molecular functions (MF), both smokers and never-smokers demonstrated enrichment in transmembrane protein kinase activity, protein serine/threonine/tyrosine kinase activity, and transmembrane receptor protein tyrosine kinase activity. Additionally, KEGG pathway analyses indicated that smokers were particularly enriched in pathways related to cellular senescence.
The GSE31852 cohort was used for subsequent analysis to explore the differences between smokers and never-smokers. Initially, 89 differentially expressed genes were identified. Figure 3B shows a heatmap presenting the detailed expression of smoking-related genes. GO analysis indicated that these genes were enriched in lymphocyte differentiation, T cell selection, and positive T cell selection in the BP category; external side of plasma membrane, spindle, and alpha-beta T cell receptor complex in the CC category; and heparin binding and signaling receptor complex adaptor activity in the MF category. KEGG enrichment analysis revealed that these smoking-related genes might be associated with measles, hematopoietic cell lineage, and primary immunodeficiency (Figure 3C). To gain a deeper understanding of the mechanisms underlying these differentially expressed genes, we utilized GSEA and found that the genes were related to immunoregulatory interactions between a lymphoid and a non-lymphoid cell, as well as cell cycle checkpoints.
Volcano plot (A) and Heatmap (C) showing the DEGs between smokers and never-smokers; GO (B) and KEGG (D) enrichment analysis for the smokers. DEGs, differentially expressed genes; GO, Gene Ontology; KEGG, Kyoto Encyclopedia of Genes and Genomes.
Discussion
This study explored the clinical outcomes and impact of smoking on patients with unresectable stage III ALK-positive NSCLC. In terms of treatment strategy, CRT can improve disease control. Our findings demonstrate significant differences in the prognosis and molecular characteristics between smokers and never-smokers, indicating smokers may require more risk-adapted treatment strategies, such as the combination of CRT with upfront ALK TKIs.
Our data show that the smoking status is a critical prognostic factor for OS in patients with unresectable stage III ALK-positive NSCLC. Both univariate and multivariate Cox regression analysis confirmed that smokers had a significantly higher risk of mortality compared with never-smokers, with a HR for overall survival of 3.92. These findings highlight the detrimental impact of smoking on survival outcomes in this population. Several mechanisms may explain the negative prognostic effect of smoking. Tobacco exposure induces widespread genomic instability and increases tumor mutational burden, potentially reducing sensitivity to targeted therapies and chemoradiotherapy (12, 13, 18, 19). The prognostic value of tumor-infiltrating lymphocytes is influenced by smoking, indicating smoking may alter the immune microenvironment (20). Consistent with our findings, previous studies have reported that smokers with advanced ALK-positive NSCLC have poorer survival than never-smokers (21). The biological basis of these observations should be further explored to determine whether this might be due to a specific mutation pattern produced by tobacco exposure.
CRT remains the standard treatment for patients with good performance status and unresectable stage III ALK-positive NSCLC. Our study found that CRT improved PFS and LRFS compared to systemic therapy, underscoring its importance in this cohort. Importantly, patients in the CRT group were not deprived of targeted therapy; most received ALK TKIs at relapse, and three patients received upfront ALK TKI without subsequent recurrence. However, no significant difference in OS or DMFS was observed between the two groups. Considering the robust efficacy of ALK TKIs, combining CRT with upfront ALK TKIs may be the optimal treatment option, especially in smokers. Recently, the integration of local therapy with targeted agents has shown significant clinical benefits in NSCLC and is changing treatment paradigms. Although the ALINA trial demonstrated that ALK TKIs significantly improved PFS in patients with resected early-stage ALK-positive NSCLC, its results highlight the potential value of ALK inhibition across different disease settings (8). Similarly, the LAURA study demonstrates that EGFR TKIs after CRT significantly prolong the PFS compared to placebo in stage III EGFR-mutated NSCLC (3). These results indicate that the strategy of local treatment combined with upfront TKIs is highly promising. A meeting abstract retrospectively reported that upfront ALK TKI demonstrated clinically meaningful improvement in PFS and OS over consolidation immunotherapy and observation (22). Currently, results from clinical trials investigating CRT combined with upfront ALK TKIs have not yet been reported, which necessitates further exploration.
The GO and KEGG enrichment analysis suggested distinct BP, CC and MF between smokers and never-smokers. Non-smokers exhibited enrichment in processes related to peptidyl-tyrosine modification and kinase activity, which are consistent with pathways that are important for cellular signaling and growth regulation. In contrast, smokers showed enrichment in gland development and epithelial cell proliferation, which may potentially contribute to more aggressive tumor phenotypes and poorer outcomes (23). Furthermore, smokers were particularly enriched in pathways related to cellular senescence, a hallmark of aging and cancer progression. Prior studies have shown that the pro-inflammatory senescence-associated secretory phenotype (SASP) can promote tumor progression (24). In our study, however, these enrichment patterns should be interpreted as associative and exploratory rather than causal. These molecular findings generate hypotheses about potential biological differences between smokers and never-smokers in stage III ALK-positive NSCLC, but they do not establish a direct causal link between smoking, the altered molecular pathways, and the observed survival differences. The results were then further explored in the GSE31852 cohort. The GO analysis indicated that these genes were enriched in immune-related processes, such as lymphocyte differentiation and T cell selection, suggesting a potential link between smoking, immune dysregulation, and NSCLC progression. The KEGG enrichment analysis further implicated these genes in pathways related to measles, hematopoietic cell lineage, and primary immunodeficiency, highlighting the complex interaction between smoking, immunity, and cancer. The GSEA revealed associations with immunoregulatory interactions and cell cycle checkpoints, which are crucial for maintaining genomic stability and preventing tumor development in general.
Our study has several limitations. First, its retrospective design and the relatively small sample size inevitably restrict statistical power. The limited sample size also prevented further investigation into the potential interplay between smoking status and sex. Second, the systemic therapy group consisted of patients receiving different ALK TKI generations or chemotherapy, and this inherent heterogeneity may affect survival comparisons with the CRT group. Given the limited sample size, further stratified analyses were not feasible, and the enrichment results based on the small NGS subset should therefore be regarded as exploratory. Moreover, the external dataset used for molecular validation differed from our cohort in baseline characteristics, and detailed information on treatment history was not available. Therefore, it was used solely to provide an independent molecular comparison between smokers and never-smokers, rather than to replicate clinical outcomes. Finally, given the distinct genomic and immunologic features associated with smoking, further mechanistic studies in larger, prospectively collected cohorts are required to validate and extend these observations.
In conclusion, our study highlights the significant impact of smoking on the prognosis of patients with unresectable stage III ALK-positive NSCLC. Smoking status emerges as an independent negative prognostic factor for OS, which should be considered when designing treatment strategies. CRT exhibits advantages in controlling locoregional disease, while systemic therapy may be necessary to address distant metastases. Future prospective studies with larger cohorts are needed to validate our results and further explore the molecular mechanisms underlying the impact of smoking on ALK-positive NSCLC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Siegel RL Miller KD Wagle NS Jemal A . Cancer statistics, 2023. CA Cancer J Clin. (2023) 73:17–48. doi: 10.3322/caac.21763, PMID: 36633525 · doi ↗ · pubmed ↗
- 2Schneider JL Lin JJ Shaw AT . ALK-positive lung cancer: a moving target. Nat Cancer.Nature Res. (2023) 4:330–43. doi: 10.1038/s 43018-023-00515-0, PMID: 36797503 PMC 10754274 · doi ↗ · pubmed ↗
- 3Lu S Kato T Dong X Ahn MJ Quang LV Soparattanapaisarn N . Osimertinib after chemoradiotherapy in stage III EGFR-mutated NSCLC. New Engl J Med. (2024) 391:585–97. doi: 10.1056/NEJ Moa 2402614, PMID: 38828946 · doi ↗ · pubmed ↗
- 4Wu YL Tsuboi M He J John T Grohe C Majem M . Osimertinib in resected EGFR -mutated non–small-cell lung cancer. New Engl J Med. (2020) 383:1711–23. doi: 10.1056/nejmoa 2027071, PMID: 32955177 · doi ↗ · pubmed ↗
- 5Soria JC Ohe Y Vansteenkiste J Reungwetwattana T Chewaskulyong B Lee KH . Osimertinib in untreated EGFR -mutated advanced non–small-cell lung cancer. New Engl J Med. (2018) 378:113–25. doi: 10.1056/nejmoa 1713137, PMID: 29151359 · doi ↗ · pubmed ↗
- 6Shaw AT Kim DW Nakagawa K Seto T CrinóL Ahn MJ . Crizotinib versus chemotherapy in advanced ALK -positive lung cancer. New Engl J Med. (2013) 368:2385–94. doi: 10.1056/nejmoa 1214886, PMID: 23724913 · doi ↗ · pubmed ↗
- 7Camidge DR Kim HR Ahn MJ Yang JC Han JY Lee JS . Brigatinib versus crizotinib in ALK -positive non–small-cell lung cancer. New Engl J Med. (2018) 379:2027–39. doi: 10.1056/nejmoa 1810171, PMID: 30280657 · doi ↗ · pubmed ↗
- 8Peters S Camidge DR Shaw AT Gadgeel S Ahn JS Kim DW . Alectinib versus crizotinib in untreated ALK -positive non–small-cell lung cancer. New Engl J Med. (2017) 377:829–38. doi: 10.1056/nejmoa 1704795, PMID: 28586279 · doi ↗ · pubmed ↗