Lemierre's Syndrome Caused by Klebsiella pneumoniae: Case Report and Review of the Literature
Abril Aguilar Guerrero, Eduardo Porras Rosales

TL;DR
This paper reports a rare case of Lemierre's syndrome caused by Klebsiella pneumoniae in a diabetic patient and reviews similar cases to highlight key risk factors and treatment strategies.
Contribution
The paper documents the second case of Klebsiella pneumoniae–associated Lemierre's syndrome in Nicaragua and emphasizes early diagnosis and treatment in diabetic patients.
Findings
Diabetes mellitus is the predominant risk factor for K. pneumoniae–associated Lemierre's syndrome.
Odontogenic or oropharyngeal disease is the most common infection source.
Septic pulmonary emboli are a hallmark manifestation of the condition.
Abstract
Klebsiella pneumoniae is an uncommon but increasingly recognized cause of Lemierre's syndrome, a condition classically associated with Fusobacterium necrophorum. This report describes a 32‐year‐old woman with poorly controlled type 2 diabetes mellitus who presented with a progressive odontogenic infection complicated by internal jugular vein thrombosis and cavitary septic pulmonary emboli. Imaging demonstrated a deep neck abscess with adjacent thrombophlebitis, and cultures from surgical drainage yielded K. pneumoniae with a wild‐type susceptibility profile. The patient required invasive mechanical ventilation, broad‐spectrum antibiotics, surgical source control, and therapeutic anticoagulation, resulting in complete clinical recovery. A review of published cases from 1996 to 2025 was performed, highlighting diabetes as the predominant risk factor, odontogenic or oropharyngeal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
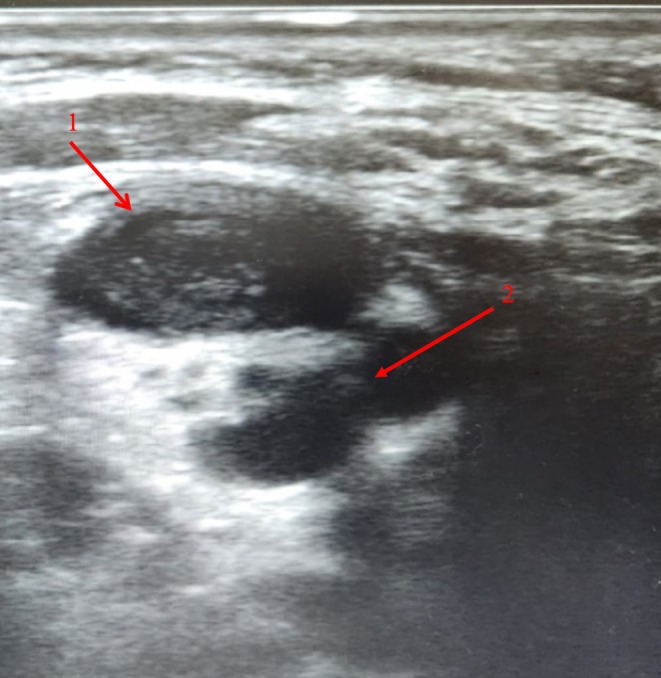 FIGURE 1
FIGURE 1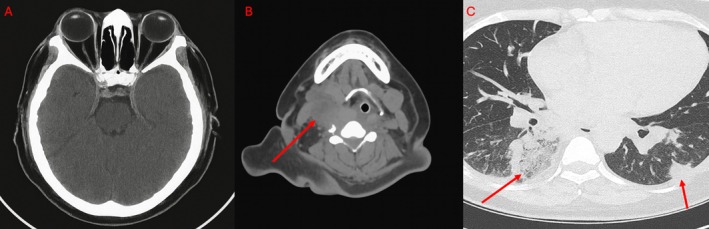 FIGURE 2
FIGURE 2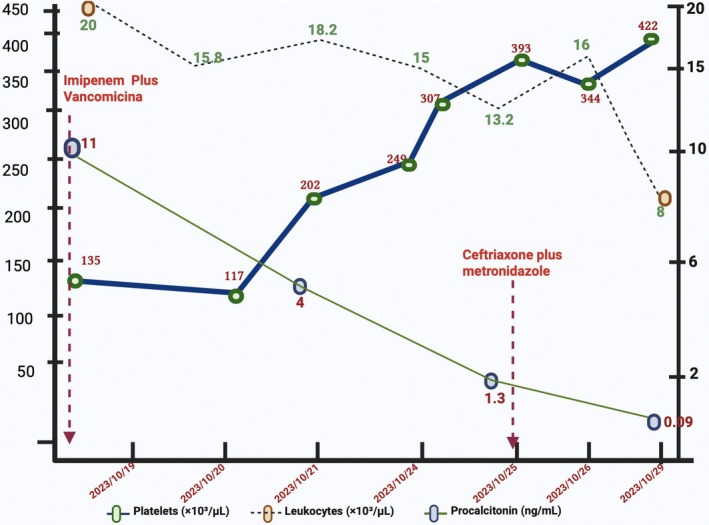 FIGURE 3
FIGURE 3| Parameter | Result | Reference range | Units |
|---|---|---|---|
|
| |||
| Hemoglobin (Hb) | 14.1 | 12.0–16.0 | g/dL |
| Platelet count | 117 × 103 | 150–400 × 103 | /mL |
| White blood cell count (WBC) | 20.9 × 103 | 4.0–10.0 × 103 | /mL |
| Neutrophils | 19.6 × 103 | 2.0–7.5 × 103 | /mL |
| C‐reactive protein (CRP) | 115 | < 10 | mg/L |
| Total bilirubin (TB) | 1.2 | 0.2–1.2 | mg/dL |
| Lactate dehydrogenase (LDH) | 300 | 135–225 | U/L |
| Serum creatinine (Cr) | 1.3 | 0.6–1.2 | mg/dL |
| Procalcitonin | 11.6 | < 0.1 | ng/mL |
| Random blood glucose | 356 | 70–140 | mg/dL |
| HbA1c | 10.8 | < 6.5 | % |
|
| |||
| PaO2 | 56 | 80–100 | mmHg |
| FiO2 | 0.21 | — | — |
| PaCO2 | 34 | 35–45 | mmHg |
| SaO2 | 84 | 95–100 | % |
| PaO2/FiO2 ratio | 267 | > 300 | — |
| Author/year | Country | Patient age/sex | Risk factors | Source of infection | Jugular vein | ABX susc | Treatment | SPE | Outcome | References |
|---|---|---|---|---|---|---|---|---|---|---|
| Bhagat et al. 1996 | USA | 52, M | DM | Odontogenic | IJV | WT | Cefazolin → Cefuroxime (14 days) | Yes | Survived | [ |
| Wu et al. 2012 | Taiwan | 54, F | DM | Oropharyngeal | IJV | WT | Ceftriaxone + Metronidazole (21 days) | Yes | Survived | [ |
| Garbati et al. 2012 | Saudi Arabia | 63, M | DM | Deep neck abscess/oropharyngeal | IJV | WT | Clindamycin + cefuroxime + warfarin (6 weeks) | No | Survived | [ |
| Chuncharunee et al. 2015 | Thailand | 51, F | DM | Right parapharyngeal abscess | IJV | WT | Ceftazidime → ampicillin/sulbactam; later meropenem; + multiple surgical drainages; + enoxaparin | Yes | Died (septic shock + multidrug‐resistant | [ |
| Chen et al. 2023 | Taiwan | 43, M | DM, Alcoholic liver cirrhosis | Right neck soft tissue infection (no clear pharyngeal focus stated) | IJV | WT | Meropenem | Yes | Died (respiratory failure within 24 h of ICU transfer) | [ |
| Sabaka et al. 2019 | Slovakia | 19, M | Previously healthy | Tonsillopharyngitis → cervical abscess | Left IJV thrombosis | WT | Ceftriaxone + Clindamycin → Piperacillin–tazobactam + Clindamycin (21 days) + surgical drainage → oral Moxifloxacin (7 days) | No | Survived; complete recovery | [ |
| Hwang et al. 2021 | South Korea | 56, F | Uncontrolled DM (HbA1c 11%), HTN, chronic otitis media | Oropharyngeal infection (sore throat) → parotid region nodule | No IJV thrombosis | WT | Piperacillin–tazobactam + Levofloxacin → Meropenem + Vancomycin → Meropenem + Amikacin; anticoagulation (LMWH → Apixaban); antifungals (Amphotericin → Itraconazole) | Yes | Survived (prolonged hospitalization; rehospitalized but recovered) | [ |
| Lee SE et al. 2021 | USA | 63, F | HTN, hyperlipidemia, well‐controlled DM | Right oropharyngeal/lateral pharyngeal infection; reactive lymphadenopathy | Right IJV extension into retromandibular vein | WT, hvKp‐K1 | Piperacillin–tazobactam → Meropenem → Ampicillin–sulbactam IV → Amoxicillin–clavulanate PO (6 weeks) + Rivaroxaban (3 months) | Yes | Survived | [ |
| Ngo et al. 2024 | Vietnam | 62, M | DM | Left neck abscess (multiloculated); oropharyngeal mass effect | Left IJV | No ABX susc. | Meropenem + Vancomycin; surgical drainage; glycemic control; vasopressors; mechanical ventilation | Yes | Survived; extubated day 4; discharged day 15 | [ |
| Rangan et al. 2024 | India | 48, M | DM | Odontogenic focus | Rigth IJV | WT | Piperacillin–tazobactam + Metronidazole + Amikacin; surgical I and D; LMWH anticoagulation; glycemic control | No | Survived | [ |
| Wong et al. 2025 | Malaysia | 54, F | DM | Odontogenic infection → deep neck abscesses (parapharyngeal & submandibular) + mandibular osteomyelitis | Right IJV | WT | IV amoxicillin–clavulanate (2 weeks) → PO amoxicillin–clavulanate (6 weeks total); surgical drainage; LMWH → Rivaroxaban anticoagulation | No | Survived | [ |
| Treminio & De la Cruz 2025 | Nicaragua | 65, F | DM, Hypertension, obesity, DKA on admission | Left submandibular abscess + otitis with otorrhea + pharyngotonsillar exudate | Left EJV | WT | Imipenem–cilastatin + Vancomycin → Ciprofloxacin (per susceptibilities) + Enoxaparin → Warfarin + surgical drainage. | Yes | Survived | [ |
| Lee WS et al. 2012 | Taiwan | 56, F | Previously healthy | Left neck abscess | Left IJV | ESBL | Ceftazidime + Metronidazole → Ceftriaxone + Amikacin → Meropenem (monotherapy) → Meropenem + Fosfomycin (IV) for 2 months | Yes | Survived | [ |
| Present case, 2025 | Nicaragua | 32, F | DM | Odontogenic | Right IJV | WT | Imipenem/Vancomycin → Ceftriaxone + Metronidazole → Oral amoxicillin–clavulanate (21 days) | Yes | Survived | — |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOtolaryngology and Infectious Diseases · Infective Endocarditis Diagnosis and Management · Streptococcal Infections and Treatments
Introduction
1
Lemierre's syndrome is an uncommon but potentially life‐threatening condition characterized by septic thrombophlebitis of the internal jugular vein following an oropharyngeal or cervicofacial infection [1, 2]. The classic pathogen, Fusobacterium necrophorum , accounts for most cases, particularly in healthy adolescents and young adults [1, 2]. Although its incidence declined with the widespread use of antibiotics, Lemierre's syndrome remains clinically relevant because of its rapid progression, diagnostic challenges, and high risk of severe complications, including cavitary septic pulmonary emboli [1, 2].
In recent years, non‐fusobacterial organisms have emerged as atypical etiologic agents. Among them, Klebsiella pneumoniae has become increasingly recognized, especially in patients with poorly controlled diabetes mellitus or other metabolic comorbidities [3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15]. Hyperglycemia‐induced immune dysfunction may predispose diabetic individuals to aggressive Gram‐negative infections, deep neck suppuration, and extensive thrombosis [3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15]. Hypervirulent strains (hvKp), particularly K1 serotypes carrying rmpA, rmpA2, and magA, have also been reported, demonstrating the ability to cause invasive, metastatic infections [10]. Compared with classical Fusobacterium‐associated disease, K. pneumoniae –associated cases often show larger cervical collections, a higher inflammatory burden, and more frequent respiratory compromise, sometimes requiring intensive care support [7, 9, 10, 15]. Early diagnosis therefore depends on maintaining a high index of suspicion, especially in diabetic patients presenting with neck swelling, fever, and respiratory distress. This report describes a severe odontogenic case of K. pneumoniae –associated Lemierre's syndrome in a young woman with diabetes mellitus, accompanied by a review of published cases. In this context, Klebsiella pneumoniae has been designated by the World Health Organization as a critical priority pathogen in the 2024 Bacterial Priority Pathogens List, emphasizing the urgent global need for improved prevention strategies and effective therapeutic options.
Case Presentation
2
A 32‐year‐old woman with a 10‐year history of type 2 diabetes mellitus and arterial hypertension presented with a 15‐day history of right facial pain, dysphagia, intermittent fever, and progressive right‐sided neck swelling. The swelling evolved into a tender, erythematous, warm mass extending from the mandibular border to the thyroid cartilage, accompanied by trismus and increasing discomfort. Three days before admission, she developed worsening dyspnea and pleuritic right‐sided chest pain, prompting emergency evaluation.
On arrival, she was febrile (38.5°C), tachycardic (130 bpm), tachypneic (36 breaths/min), and hypoxemic (oxygen saturation 84% on room air). Her random blood glucose was markedly elevated. Physical examination revealed facial asymmetry, multiple dental foci of infection, and a firm, tender cervical mass involving levels III–IV with overlying erythema and warmth. Respiratory assessment demonstrated the use of accessory muscles and bilateral basal crackles.
On admission, the patient had marked hyperglycemia, with a random blood glucose level of 356 mg/dL and a glycated hemoglobin (HbA1c) of 10.8%, consistent with chronically poor glycemic control. Intensive insulin therapy was initiated during hospitalization, achieving progressive metabolic stabilization without hypoglycemic events.
Arterial blood gas analysis confirmed moderate acute hypoxemic respiratory failure. Her SOFA score was 7 [16] and APACHE II score was 14 [17], indicating significant systemic compromise. Due to progressive respiratory distress, the patient was intubated and placed on invasive mechanical ventilation.
Initial laboratory studies revealed leukocytosis with marked neutrophilia, thrombocytopenia, hyperglycemia, and elevated inflammatory markers (Table 1). Two sets of blood cultures were obtained at admission prior to the initiation of antimicrobial therapy, each consisting of aerobic bottles, in accordance with local laboratory availability. All blood cultures remained negative after standard incubation. Microbiological cultures obtained from surgical drainage of the cervical abscess yielded Klebsiella pneumoniae. Antimicrobial susceptibility testing demonstrated a wild‐type susceptibility profile, with sensitivity to third‐generation cephalosporins, carbapenems, β‐lactam/β‐lactamase inhibitor combinations, fluoroquinolones, and aminoglycosides. No extended‐spectrum β‐lactamase production was detected.
Cervical ultrasonography demonstrated thrombosis of the right internal jugular vein adjacent to a 21 mL cervical abscess (Figure 1). Chest computed tomography (CT) revealed multiple peripheral cavitary nodules consistent with septic pulmonary emboli, while cranial CT excluded intracranial extension or venous sinus thrombosis (Figure 2).
Cervical ultrasonography demonstrating a heterogeneous hypoechoic collection with internal echoes (arrow 1) adjacent to a dilated right internal jugular vein containing heterogeneous echogenic intraluminal material without Doppler flow (arrow 2), consistent with a cervical abscess (approximately 21 mL) and associated internal jugular vein thrombosis.
(A) Axial non‐contrast head computed tomography (CT) showing no evidence of intracranial extension, venous sinus thrombosis, or parenchymal abnormalities. (B) Axial contrast‐enhanced neck CT demonstrating a right‐sided hypodense deep neck collection with surrounding soft‐tissue edema and thrombosis of the right internal jugular vein, evidenced by non‐opacified intraluminal material (arrow). (C) Axial contrast‐enhanced chest CT demonstrating multiple peripheral cavitary nodules and consolidations, predominantly in the right lower lobe, consistent with septic pulmonary emboli (arrows).
Because of the evident odontogenic origin, surgical extraction of infected teeth and drainage of the cervical abscess were performed under general anesthesia. Cultures from the drained material grew Klebsiella pneumoniae with a wild‐type susceptibility profile, confirming the etiologic agent.
Empiric therapy with imipenem and vancomycin was initiated. Vancomycin was discontinued after microbiological confirmation, and carbapenem therapy was limited to 4 days, followed by targeted treatment with ceftriaxone and metronidazole. Therapeutic anticoagulation with enoxaparin was administered for internal jugular vein thrombosis and was well tolerated, with platelet recovery by day five (Figure 3).
Temporal evolution of leukocyte count, platelet count, and procalcitonin levels during antimicrobial therapy and therapeutic anticoagulation, demonstrating progressive normalization of inflammatory and hematologic parameters. Figure created with BioRender.com.
The patient showed steady clinical improvement, became afebrile and normoxemic, and was successfully extubated on day seven. She was discharged on oral amoxicillin–clavulanate with scheduled outpatient follow‐up.
Investigations and Management
3
Based on the clinical presentation, targeted diagnostic investigations were promptly initiated, followed by combined medical and surgical management.
The combination of progressive cervical swelling, fever, odynophagia, and respiratory compromise raised several diagnostic possibilities, including deep neck space infection, odontogenic abscess, cervical lymphadenitis, necrotizing fasciitis, Lemierre's syndrome, and septic pulmonary embolism. The presence of a firm, tender cervical mass with overlying inflammatory changes prompted urgent imaging. Cervical ultrasonography revealed thrombosis of the right internal jugular vein adjacent to a deep neck abscess, strongly supporting a diagnosis of Lemierre's syndrome. Chest computed tomography further confirmed multiple cavitated pulmonary nodules consistent with septic emboli, thereby consolidating the diagnosis.
Given the presumed odontogenic origin, empiric broad‐spectrum antimicrobial therapy with imipenem and vancomycin was initiated to ensure coverage of both aerobic and anaerobic organisms. Surgical extraction of the infected teeth and drainage of the cervical abscess provided prompt and effective source control. Culture of the drained material grew Klebsiella pneumoniae with a wild‐type susceptibility profile, allowing de‐escalation to targeted therapy with ceftriaxone and metronidazole. Therapeutic anticoagulation with low molecular weight heparin (enoxaparin) was initiated due to extensive internal jugular vein thrombosis and the presence of septic pulmonary emboli. After careful assessment of bleeding risk, anticoagulation was planned for a total duration of 3 months. Follow up cervical ultrasonography demonstrated partial recanalization of the affected vein without hemorrhagic complications.
This combined medical and surgical approach resulted in rapid clinical stabilization, with resolution of fever, improvement in inflammatory markers, and progressive recovery of respiratory function.
Outcome and Follow‐Up
4
The patient demonstrated rapid and sustained clinical improvement following cervical drainage, targeted antimicrobial therapy, and therapeutic anticoagulation. Fever resolved within 48 h, and her respiratory status improved progressively, allowing successful extubation on day seven.
At 2 weeks postoperatively, follow‐up cervical ultrasonography revealed partial recanalization of the right internal jugular vein and near‐complete resolution of the cervical abscess. A one‐month follow‐up chest CT showed complete resolution of cavitary pulmonary lesions with no new embolic phenomena. She completed a 14‐day course of intravenous antibiotics followed by an additional 7‐day oral regimen. At her six‐week outpatient evaluation, she remained asymptomatic, with normalized inflammatory markers and no evidence of recurrent infection, thrombosis, or respiratory impairment. She had fully returned to her baseline functional status, and her overall prognosis was favorable.
Discussion
5
Lemierre's syndrome is traditionally attributed to Fusobacterium necrophorum and most commonly affects previously healthy adolescents and young adults [1, 2]. In recent years, however, Klebsiella pneumoniae has emerged as an uncommon yet clinically significant alternative pathogen, predominantly in individuals with metabolic derangements or impaired immune function. Since its initial description in 1996 [3], only 13 cases of K. pneumoniae –associated Lemierre's syndrome have been reported worldwide, underscoring both the rarity of this variant and the importance of maintaining diagnostic vigilance.
The epidemiologic profile of this entity differs notably from that of classical Fusobacterium infection. Among the published cases, over 80% of patients had diabetes mellitus, often poorly controlled, highlighting hyperglycemia as a key facilitator of severe Gram‐negative infection [3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15]. Chronic hyperglycemia compromises fundamental functions of the innate immune response, including neutrophil chemotaxis, oxidative burst, and phagocytosis, thereby predisposing patients to aggressive soft tissue infections and vascular complications. Additional comorbidities reported include alcohol use disorder [10], chronic kidney disease [12], and obesity with diabetic ketoacidosis [14], all of which may further impair host defenses. Collectively, these data point to a distinct phenotype characterized by immunometabolic susceptibility, which appears central to the pathogenesis of K. pneumoniae –associated Lemierre's syndrome.
From a microbiological standpoint, most reported isolates demonstrate wild‐type antimicrobial susceptibility. Nevertheless, cases involving hypervirulent K. pneumoniae (hvKp) strains have been documented, particularly those harboring the K1 capsular serotype and virulence determinants such as rmpA, rmpA2, and magA [10]. These genetic features confer a hypermucoviscous phenotype that enhances tissue invasion, intravascular persistence, and metastatic dissemination. Importantly, virulence, hypervirulence, and antimicrobial resistance should not be viewed as mutually exclusive phenotypes, as emerging data indicate that certain strains may exhibit overlapping characteristics. Despite global concern regarding antimicrobial resistance in K. pneumoniae , only one reported case of Lemierre's syndrome involved an extended‐spectrum β‐lactamase–producing strain [15]. Overall, most infections appear to be community‐acquired and remain susceptible to third‐generation cephalosporins and carbapenems.
Clinically, K. pneumoniae ‐associated Lemierre's syndrome mirrors those of the classical form and typically include: fever and systemic inflammatory response, odontogenic or oropharyngeal infection, internal (or, rarely, external) jugular vein thrombosis, and cavitating septic pulmonary emboli, the hallmark metastatic feature [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15]. Notably, several patients developed early acute hypoxemic respiratory failure requiring mechanical ventilation [7, 10, 15], a trend that may reflect the heightened inflammatory response characteristic of Gram‐negative sepsis. Severity scoring systems such as SOFA [16] and APACHE II [17] often reveal early organ dysfunction at presentation. Contrast‐enhanced CT imaging remains the gold standard for identifying jugular vein thrombosis and pulmonary embolic lesions, whereas ultrasonography provides a valuable rapid assessment tool, particularly in unstable patients.
Analysis of the 13 previously reported cases (Table 2) reveals a consistent clinical and epidemiologic pattern: Diabetes mellitus is the predominant risk factor, odontogenic and oropharyngeal infections are the most frequent sources [3, 4, 6, 13]. Internal jugular vein thrombosis is the defining vascular complication, although external jugular involvement has been documented [14]. Cavitating septic pulmonary emboli are common and serve as the characteristic metastatic manifestation [3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15].
TABLE 2: Reported cases of Klebsiella pneumoniae ‐associated Lemierre's syndrome (1996–2025).
Management strategies emphasize early antimicrobial therapy and definitive source control. Empirical antimicrobial regimens should provide coverage against aerobic Gram‐negative organisms and anaerobes. Most reported patients received carbapenems, third‐generation cephalosporins, or β‐lactam/β‐lactamase inhibitor combinations, with subsequent de‐escalation guided by susceptibility results proving consistently effective [3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15]. Treatment duration varied according to disease severity, ranging from 14 to 21 days in uncomplicated cases [3, 4, 8] to 3–6 weeks in patients with extensive deep neck infection or respiratory compromise, and up to 6–8 weeks in the single ESBL associated case complicated by intracranial dissemination [15]. These observations underscore the need for individualized therapy guided by clinical response and radiologic follow‐up.
Odontogenic and oropharyngeal infections represent the most frequent primary foci, underscoring the importance of rapid and definitive surgical source control [3, 4, 6, 13]. Prompt extraction of infected teeth and drainage of deep neck abscesses are essential to reduce bacterial burden, resolve thrombophlebitis, and prevent ongoing embolization. In the present case, timely surgical intervention played a pivotal role in achieving clinical stabilization.
The role of anticoagulation in Lemierre's syndrome remains controversial, as robust randomized controlled data are lacking. However, large observational studies and systematic analyses suggest that selected patients with extensive internal jugular vein thrombosis, thrombus propagation, or recurrent septic embolization may benefit from anticoagulation, without a clear increase in major bleeding events [18, 19]. Careful individualized assessment of bleeding risk is therefore essential. In our patient, anticoagulation was initiated due to extensive jugular thrombosis and septic pulmonary emboli, maintained for 3 months, and guided by follow‐up imaging demonstrating partial recanalization without adverse events.
Klebsiella pneumoniae ‐associated Lemierre's syndrome often follows a more severe clinical course than classical Fusobacterium infection. Several cases have reported early respiratory failure requiring mechanical ventilation [7, 10, 15], and two fatalities (≈15%) have been documented [6, 7, 20]. Poor glycemic control, delayed diagnosis, and extensive cavitating septic pulmonary emboli appear to be key predictors of adverse outcomes.
This report represents the second documented case of K. pneumoniae ‐associated Lemierre's syndrome in Nicaragua, following the case involving external jugular thrombosis described by Treminio and De la Cruz [14]. Together, these cases suggest that Gram‐negative variants of Lemierre's syndrome may be underrecognized in Central America, highlighting the need for early imaging, aggressive source control, and targeted antimicrobial therapy, particularly among diabetic patients.
A structured literature search conducted across PubMed/MEDLINE, EMBASE, Scopus, Web of Science, and Google Scholar from January 1990 to January 2025 identified 13 published cases of K. pneumoniae associated with Lemierre's syndrome, which contextualize the present report within the existing body of evidence.
Overall, this case underscores Klebsiella pneumoniae as an emerging atypical cause of Lemierre's syndrome, particularly in the setting of poorly controlled diabetes mellitus. Compared with classical * Fusobacterium necrophorum‐associated* disease, Gram‐negative variants may present with more severe local infection, extensive thrombosis, and early respiratory failure. Early recognition, prompt imaging, definitive surgical source control, appropriate antimicrobial therapy, and selected use of anticoagulation were essential for a favorable outcome. Increased awareness of non‐fusobacterial Lemierre's syndrome is crucial to avoid diagnostic delay and improve prognosis in high‐risk patients.
Author Contributions
Eduardo Porras Rosales: conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, supervision, writing – review and editing. Abril Aguilar Guerrero: conceptualization, formal analysis, investigation, methodology, project administration, writing – original draft, writing – review and editing.
Funding
The authors have nothing to report.
Consent
Written informed consent was obtained from the patient for the publication of this case report, including all clinical information, diagnostic data, and accompanying imaging studies. The patient explicitly approved the use of de‐identified photographs, radiologic images, and any other potentially identifiable material in accordance with the journal's patient consent requirements and international ethical standards.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A. Tiwari , “Lemierre's Syndrome in the 21st Century: A Literature Review,” Cureus 15 (2023): e 43685, 10.7759/cureus.43685.37724228 PMC 10505273 · doi ↗ · pubmed ↗
- 2K. Kuppalli , D. Livorsi , N. J. Talati , and M. Osborn , “Lemierre's Syndrome due to Fusobacterium necrophorum ,” Lancet Infectious Diseases 12, no. 10 (2012): 808–815, 10.1016/S 1473-3099(12)70089-0.22633566 · doi ↗ · pubmed ↗
- 3B. Bhagat , M. Ahmed , S. W. Ali , and K. Roistacher , “A Case of Lemierre's Syndrome due to Klebsiella pneumoniae ,” Infectious Diseases in Clinical Practice 5, no. 6 (1996): 389–390.
- 4H. M. Wu , Y. J. Tsai , J. C. Lin , and P. R. Hsueh , “A Lemierre Syndrome Variant Caused by Klebsiella pneumoniae ,” Journal of the Formosan Medical Association 111, no. 7 (2012): 403–405, 10.1016/j.jfma.2012.03.012.22817819 · doi ↗ · pubmed ↗
- 5M. A. Garbati , A. M. Ahsan , and A. M. Hakawi , “Lemierre's Syndrome due to Klebsiella pneumoniae in a 63‐Year‐Old Man With Diabetes: A Case Report,” Journal of Medical Case Reports 6 (2012): 97, 10.1186/1752-1947-6-97.22472458 PMC 3337804 · doi ↗ · pubmed ↗
- 6A. Chuncharunee and T. Khawcharoenporn , “Lemierre's Syndrome Caused by Klebsiella pneumoniae in a Diabetic Patient: A Case Report and Literature Review,” Hawaii Journal of Medicine & Public Health 74, no. 8 (2015): 276–279.PMC 453673726279962 · pubmed ↗
- 7T. A. Chen , Y. T. Chuang , H. Y. Lin , and C. H. Chen , “Lemierre's Syndrome Caused by Klebsiella pneumoniae: A Case Report and Literature Review,” Cureus 15, no. 8 (2023): e 44434, 10.7759/cureus.44434.37664341 PMC 10469873 · doi ↗ · pubmed ↗
- 8P. Sabaka , M. Káčerik , M. Bendžala , and H. Káčerová , “Lemierre Syndrome Caused by Klebsiella pneumoniae Complicated by Epidural Abscess – Case Report,” ID Cases 19 (2019): e 00664, 10.1016/j.idcr.2019.e 00664.32226757 PMC 7093747 · doi ↗ · pubmed ↗