Atypical Early Presentation of Multicentric Carpotarsal Osteolysis: Ankle Pain and Cavovarus Deformity Without Osteolysis
Daniel Kim, Marty McGraw, Jennifer Kucera, Tushar Chandra, Manish Bajaj

TL;DR
A rare bone disorder called MCTO presented with ankle pain and foot deformity in a child, diagnosed through genetic testing despite lack of typical bone loss.
Contribution
Highlights an atypical early presentation of MCTO without visible bone loss, emphasizing the importance of genetic testing for accurate diagnosis.
Findings
A 9-year-old female presented with ankle pain and cavovarus deformity but no visible osteolysis.
Genetic testing confirmed a pathogenic MAFB variant, diagnosing MCTO despite atypical imaging findings.
Early recognition of subtle symptoms can prevent misdiagnosis and unnecessary interventions.
Abstract
Multicentric carpotarsal osteolysis (MCTO) is a rare skeletal dysplasia classically associated with carpal and tarsal osteolysis. Its presentation is highly variable, ranging from subtle musculoskeletal deformities to progressive bone loss and renal involvement. We report a nine-year-old female who presented with progressive ankle pain, cavovarus foot deformity, and gait disturbance. Initial radiographs demonstrated osteopenia and bilateral pes cavus without frank osteolysis. Genetic testing identified a pathogenic MAFB variant, confirming the diagnosis of MCTO. This case highlights the broad clinical and radiologic spectrum of MCTO, in which early or atypical presentations may have subtle, nondiagnostic imaging findings. Recognizing these early features can raise clinical suspicion and prompt genetic evaluation, helping to avoid misdiagnosis and unnecessary interventions. Awareness of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1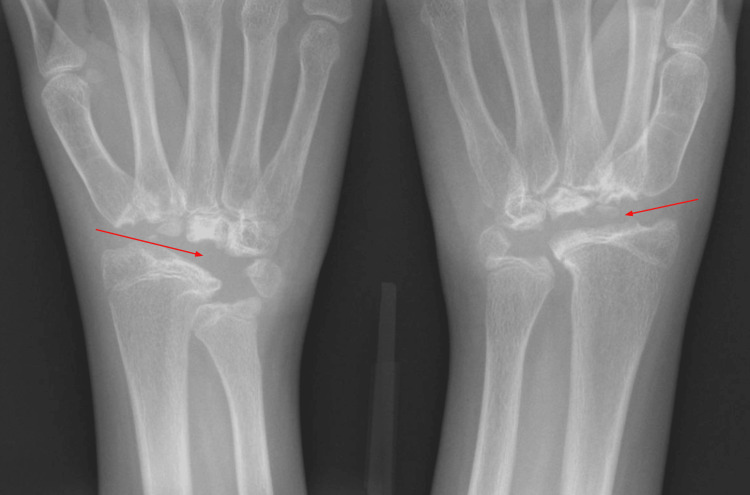 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsConnective tissue disorders research · Dermatological and Skeletal Disorders · Genetic Syndromes and Imprinting
Introduction
Multicentric carpotarsal osteolysis (MCTO) is a rare hereditary skeletal disorder characterized by progressive osteolysis of the carpal and tarsal bones, often associated with nephropathy, with fewer than 60 documented cases as of 2022 [1]. Most cases of MCTO present in early childhood with advanced bone resorption, manifested as joint pain, swelling, deformity, and radiographic signs of aggressive osteolysis of the carpal and tarsal bones. In contrast, early or subtle presentations pose a diagnostic challenge, as imaging findings can mimic benign orthopedic variations, metabolic bone disorders, or inflammatory arthropathies [2]. The clinical and radiographic spectrum is broad. Some patients initially exhibit nonspecific findings, such as osteopenia, deformity, or gait abnormalities, before obvious osteolysis is seen [3]. A literature review of 54 reported cases revealed a mean age of symptom onset of two years and a mean age at diagnosis of nine years, demonstrating an average delay of seven years [1]. Recognizing these subtler manifestations is important, as delayed diagnosis can lead to inappropriate treatment and missed opportunities for early surveillance of systemic complications, particularly renal function.
We present the case of a nine-year-old with progressive foot deformities that highlights the early spectrum of symptoms in MCTO and the importance of considering MCTO in the differential diagnosis of pediatric patients presenting with nonspecific joint pain, in the absence of radiographic osteolysis.
Case presentation
A nine-year-old female with no significant past medical history presented to neurology for progressive bilateral foot deformities, neuropathic pain, and gait abnormalities that began around four years of age. The initial radiograph was nonspecific and revealed generalized osteopenia with bilateral pes cavus, right worse than left (Figure 1). Further workup included electromyography, magnetic resonance imaging of the spine, a comprehensive neuropathy genetic panel, and serum inflammatory markers, all of which were normal.
Initial radiographs of bilateral feet show pes cavus, right worse than left, and generalized osteopenia.Red arrows depict bilateral pes cavus.
The patient was then referred to orthopedic surgery to address the pain and functional impairment associated with the right cavovarus deformity. At the same time, whole-exome genetic testing was ordered and revealed a heterozygous pathogenic variant in the MAFB gene, confirming the diagnosis of MCTO. The patient underwent surgical reconstruction of the right foot and aggressive physical therapy. She eventually reported improved function and minimal foot pain without the use of orthotics. At age 11, the patient presented again with bilateral wrist pain. She slowly began to lose function and mobility in her wrists and had difficulty closing her fists, playing the violin, and combing her hair. Radiographs of the bilateral wrists demonstrated diffuse osteolysis of multiple carpal bones, with degenerative changes at the carpometacarpal joints (Figure 2). No definitive treatment was offered for her wrists due to her known diagnosis of MCTO. Fusion of the wrists is being considered once she is skeletally mature. She currently does not have any renal complications, but will continue to be monitored annually.
Radiographs of the bilateral wrists show extensive osteolysis of the carpal bones, with degenerative changes at the carpometacarpal joints.Red arrows depict bilateral osteolysis of carpal bones.
Discussion
MCTO is a rare skeletal dysplasia, most commonly caused by heterozygous mutations in the MAFB gene. Pathogenic variants disrupt transcriptional regulation of osteoclast differentiation, leading to progressive bone resorption. MCTO can also impact renal podocytes, resulting in proteinuria or nephrotic syndrome in some patients [4]. It remains diagnostically challenging due to its rarity and variable presentation. The age of onset typically falls in early childhood, but symptoms can range from subtle joint discomfort to severe pain and deformity. Some patients present with progressive swelling, pain, and stiffness, while others may remain relatively asymptomatic until functional impairment becomes evident, at which point significant osteolysis is already apparent on imaging [5].
Early radiologic findings, as seen in our case, may present as generalized osteopenia, subtle irregularity, or mild resorption/collapse of the carpal and tarsal bones. These nonspecific findings are often bilateral and symmetrical, and mimic inflammatory changes seen in juvenile idiopathic arthritis (JIA) [3]. Other cases of MCTO, with nonspecific polyarticular pain without definitive carpal or tarsal bone resorption, are often misdiagnosed as JIA, contributing to diagnostic delay. Outside of joint pain, MCTO can further be distinguished by renal, ocular, or craniofacial abnormalities [3]. As MCTO progresses, findings of advanced disease are overt, and show complete disappearance of the carpal and tarsal bones, leading to joint instability, deformity, and loss of function [6]. Just like in our case, a few years after the initial diagnosis, the patient developed near-complete osteolysis of both wrists. Nevertheless, imaging alone is insufficient in early disease, and genetic confirmation is necessary.
Treatment for MCTO is primarily supportive, as many patients present with advanced disease. However, denosumab has been proposed, in case reports, as a potential therapy aimed at preventing osteolysis [7]. Other reports state that denosumab does not stop the progression of disease [8]. Specific factors regarding the decision to start the medicine were not available for review, and there is not enough evidence of standardized treatment guidelines. In our case, the patient underwent surgical reconstruction for her right cavovarus deformity before being diagnosed with MCTO. At the time, the absence of frank osteolysis and the presence of foot deformity supported a more common orthopedic etiology. She reported subjective improvement of her symptoms and gait following repair; however, in retrospect, this highlights a potential risk of surgical management in patients with underlying osteolytic disorders, as there may be further complications and altered biomechanics in relation to progressive tarsal osteolysis, with retained metallic hardware in the foot.
Conclusions
In summary, MCTO is a rare but important consideration in pediatric patients with progressive musculoskeletal symptoms and nonspecific radiographic findings. Our case aims to highlight the atypical, early presentation of MCTO and emphasize that the absence of overt osteolysis does not exclude the diagnosis. In these situations, a comprehensive approach that integrates clinical suspicion, careful radiologic evaluation, and genetic testing ensures an accurate diagnosis of MCTO and facilitates early monitoring for systemic complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Multicentric carpotarsal osteolysis syndrome associated nephropathy: novel variants of MAFB gene and literature review J Clin Med Drovandi S Lugani F Boyer O 44231120223595603810.3390/jcm 11154423 PMC 9369440 · doi ↗ · pubmed ↗
- 2Multicentric carpotarsal osteolysis: a contemporary perspective on the unique skeletal phenotype Curr Osteoporos Rep Ma NS Mumm S Takahashi S Levine MA 85942120233647736610.1007/s 11914-022-00762-7PMC 10393442 · doi ↗ · pubmed ↗
- 3Multicentric carpo-tarsal osteolysis syndrome mimicking juvenile idiopathic arthritis: two case reports and review of the literature Front Pediatr Wu J Wang L Xu Y 745812920213472242610.3389/fped.2021.745812 PMC 8554157 · doi ↗ · pubmed ↗
- 4A familial case of multicentric carpotarsal osteolysis syndrome and treatment outcome J Pediatr Genet Upadia J Gomes A Weiser P Descartes M 174179720183043003510.1055/s-0038-1657760 PMC 6234043 · doi ↗ · pubmed ↗
- 5Multicentric carpotarsal osteolysis syndrome with variants of MAFB gene: a case report and literature review Pediatr Rheumatol Online J Gao X Fang X Huang D Zhang S Zeng H 372220243848122410.1186/s 12969-024-00964-6PMC 10935943 · doi ↗ · pubmed ↗
- 6Multicentric carpotarsal osteolysis syndrome: long-term follow-up of three patients Skeletal Radiol Klein C Bellity J Finidori G Glorion C Pannier S 101510194720182939669710.1007/s 00256-018-2874-z · doi ↗ · pubmed ↗
- 7Multicentric carpotarsal osteolysis syndrome (MCTO) with generalized high bone turnover and high serum RANKL: response to denosumab Bone Rep Regev R Sochett EB Elia Y 1007471420213350607810.1016/j.bonr.2021.100747 PMC 7815641 · doi ↗ · pubmed ↗
- 8Denosumab treatment does not halt progression of bone lesions in multicentric carpotarsal osteolysis syndrome JBMR Plus Lerman MA Francavilla M Waqar-Cowles L Levine MA 07202310.1002/jbm 4.10729 PMC 1018401937197321 · doi ↗ · pubmed ↗