Two-layer closure method using anchor pronged clips for endoscopic full-thickness resection
Takashi Kodato, Yoichi Yamamoto, Masao Yoshida, Noboru Kawata, Kenichiro Furukawa, Etsuro Bando, Hiroyuki Ono

Abstract
Click any figure to enlarge with its caption.
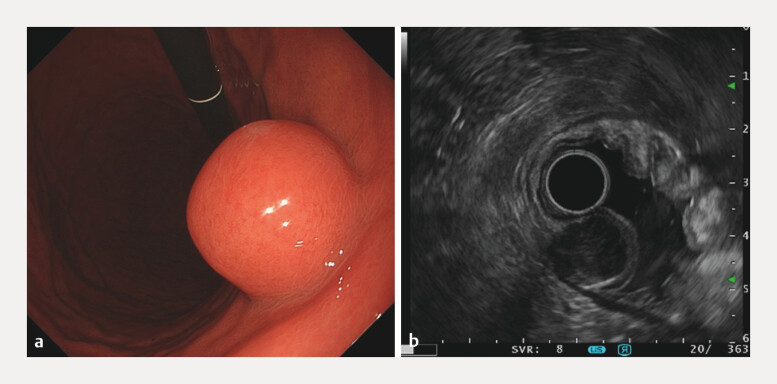 Fig. 1
Fig. 1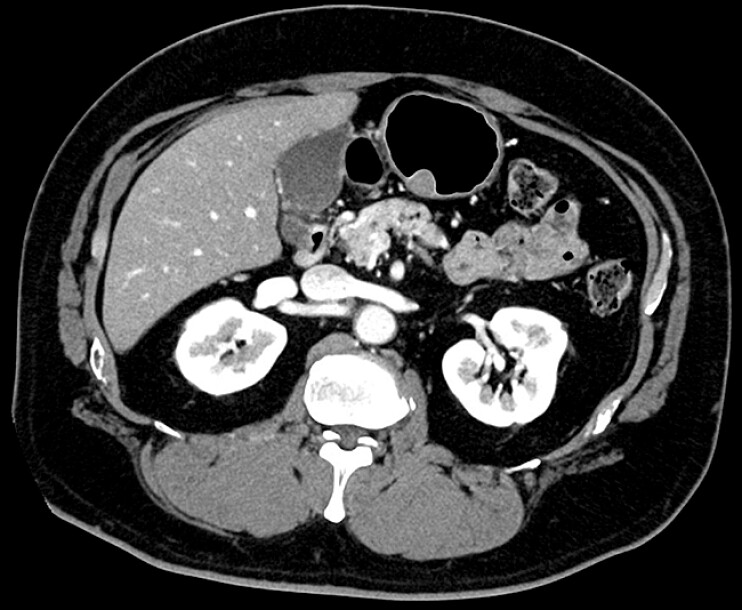 Fig. 2
Fig. 2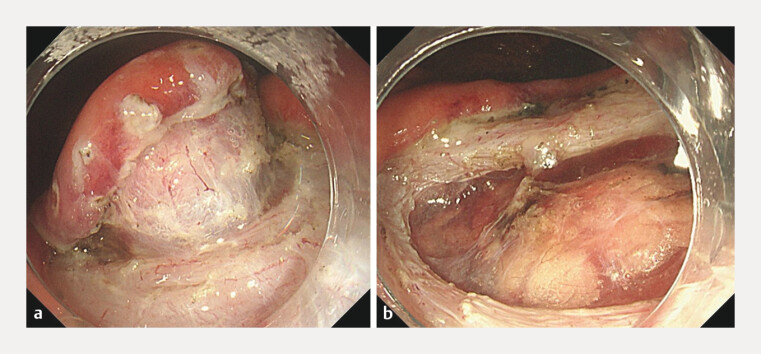 Fig. 3
Fig. 3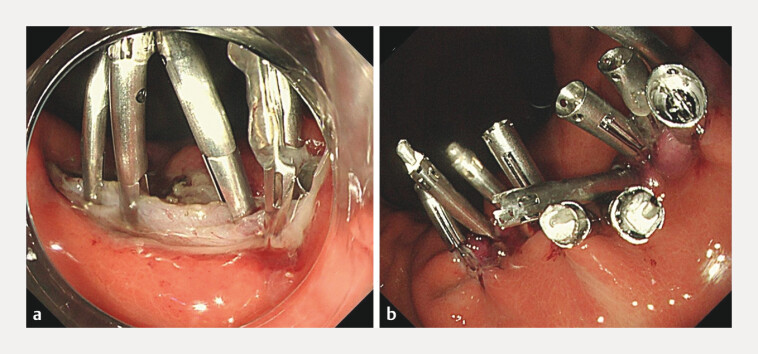 Fig. 4
Fig. 4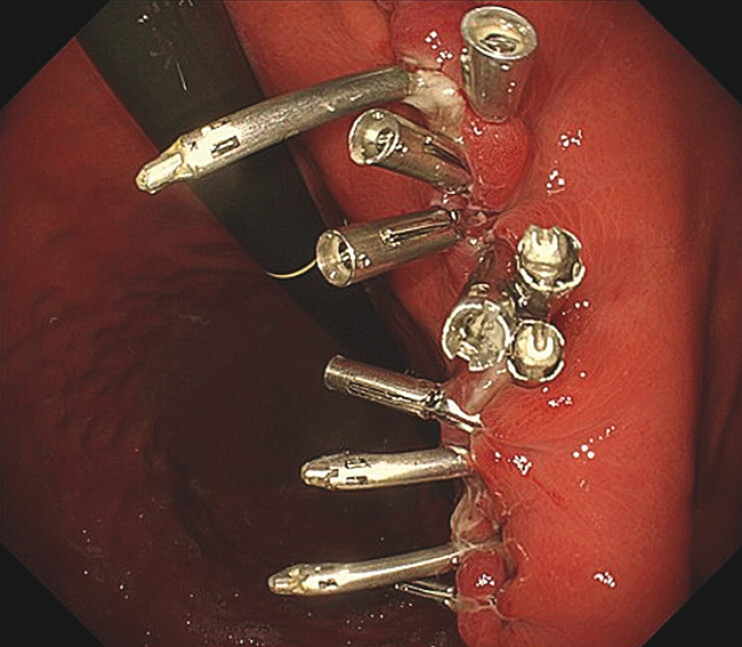 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Minimally Invasive Surgical Techniques · Gastric Cancer Management and Outcomes
A 54-year-old man underwent esophagogastroduodenoscopy, which revealed a 25 mm submucosal tumor in the lower gastric body ( Fig. 1 a ). Endoscopic ultrasound-guided fine-needle biopsy led to a diagnosis of gastric gastrointestinal stromal tumors (GISTs; Fig. 1 b ). Computed tomography revealed no evidence of metastasis ( Fig. 2 ). We therefore proceeded with endoscopic full-thickness resection (EFTR) to treat this submucosal tumor ( Video 1 ).
Esophagogastroduodenoscopy a and EUS b revealed a 25-mm submucosal tumor in the lower gastric body. EUS, endoscopic ultrasound.
Computed tomography revealed a 25-mm gastric submucosal tumor and no evidence of metastasis.
The defect after EFTR was closed with four MANTIS clips for the muscle layer and additional clips for the mucosa following successful specimen extraction. EFTR, endoscopic full-thickness resection.Video 1
Under general anesthesia, we carefully dissected the submucosa to minimize any resulting full-thickness defects prior to specimen removal ( Fig. 3 a ). The specimen was successfully extracted via a minimal muscle layer incision without capsule injury ( Fig. 3 b ).
a The submucosa to minimize any resulting full-thickness defects prior to specimen removal. b Extraction of specimens with minimal muscle dissection.
Four anchor-pronged clips (MANTIS clips; Boston Scientific) were used to close the defect between the muscle layers of the stomach wall ( Fig. 4 a ). Subsequently, we used three additional MANTIS and five conventional clips to close the mucosal defects, achieving complete closure ( Fig. 4 b ).
a Use anchor-pronged clips (MANTIS clips; Boston Scientific) to close the wound between the muscle layers. b Use MANTIS clips and conventional clips to close the mucosal defects.
Esophagogastroduodenoscopy on postoperative day 3 confirmed complete closure of the resection site ( Fig. 5 ). No postoperative complications such as bleeding or delayed perforation were observed, and the patient was discharged on postoperative day 6.
Postoperative day 3: complete closure of the treatment site was maintained.
Postoperative histopathological evaluation confirmed negative horizontal and vertical margins, with a final diagnosis of very low risk GIST (Modified Fletcher Classification).
EFTR represents an effective treatment option for small GISTs 1 . However, delayed perforation at full-thickness closure sites after resection remains a major concern 2 .
While earlier methods focused on mucosal layer closure 1 , various techniques have since been proposed to improve closure security, averting perforation 3 4 . Our recommended approach employs MANTIS clips for the independent closure of the muscle and mucosal layers, similar to the standard two-layer surgical suturing technique 5 . This method offers more robust closure than mucosal-only suturing, and is therefore expected to reduce postoperative complications.
Endoscopy_UCTN_Code_TTT_1AO_2AO
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zhou PH Yao LQ Qin XY Endoscopic full-thickness resection without laparoscopic assistance for gastric submucosal tumors originated from the muscularis propria Surgical Endoscopy 2011252926293121424195 10.1007/s 00464-011-1644-y · doi ↗ · pubmed ↗
- 2Guo J Liu Z Sun S Endoscopic full-thickness resection with defect closure using an over-the-scope clip for gastric subepithelial tumors originating from the muscularis propria Surgical Endoscopy 2015293356336225701060 10.1007/s 00464-015-4076-2PMC 4607707 · doi ↗ · pubmed ↗
- 3Huberty V Leclercq L Hiernaux M Endoscopic full-thickness resection using an endoluminal-suturing device: A proof-of-concept study Endoscopy International Open 20197 E 1310 E 131510.1055/a-0860-538731673599 PMC 6805186 · doi ↗ · pubmed ↗
- 4Goto O Koizumi E Higuchi K Endoscopic full-thickness resection with double-layer closure by endoscopic hand suturing for a gastric subepithelial tumor Endoscopy 202254 E 964E 96535913062 10.1055/a-1884-0065 PMC 9736897 · doi ↗ · pubmed ↗
- 5Shikata S Yamagishi H Taji Y Single- versus two- layer intestinal anastomosis: A meta-analysis of randomized controlled trials BMC Surgery 20066210.1186/1471-2482-6-216438733 PMC 1373646 · doi ↗ · pubmed ↗