An Adult Case of Chest Wall Langerhans Cell Histiocytosis Mimicking Malignancy and Responding to Targeted Therapy
Michael W Alchaer, Trina Capelli, Thomas A Abbruzzese, Alene Wright

TL;DR
A rare case of chest wall Langerhans cell histiocytosis in an adult was misdiagnosed as malignancy but successfully treated with targeted therapy after molecular testing.
Contribution
This case highlights the diagnostic challenge of adult LCH mimicking malignancy and demonstrates the effectiveness of BRAF/MEK inhibition in treatment.
Findings
Adult chest wall LCH can radiographically resemble malignancy, requiring biopsy for diagnosis.
Molecular testing identified a BRAF V600E mutation, leading to successful treatment with dabrafenib and trametinib.
Targeted BRAF/MEK inhibition may be an effective therapeutic option when conventional treatments fail.
Abstract
Langerhans cell histiocytosis (LCH) is a rare clonal proliferation of dendritic cells that is exceptionally uncommon in adults and only rarely affects the chest wall. Adult rib lesions often radiographically mimic malignancy, necessitating biopsy for accurate diagnosis. We report the case of a 52-year-old woman with Class III (severe) obesity and newly diagnosed type 2 diabetes who developed a painful right chest wall mass following severe coughing during coronavirus disease 2019 (COVID-19). Imaging revealed a lobulated lesion with rib erosion and pleural indentation concerning for malignancy. Surgical debridement yielded histiocytic inflammation, and cultures grew Staphylococcus epidermidis. Final histopathology confirmed LCH. Despite wound re-closures and antibiotic therapy, persistent drainage continued until molecular testing identified a B-Raf proto-oncogene,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
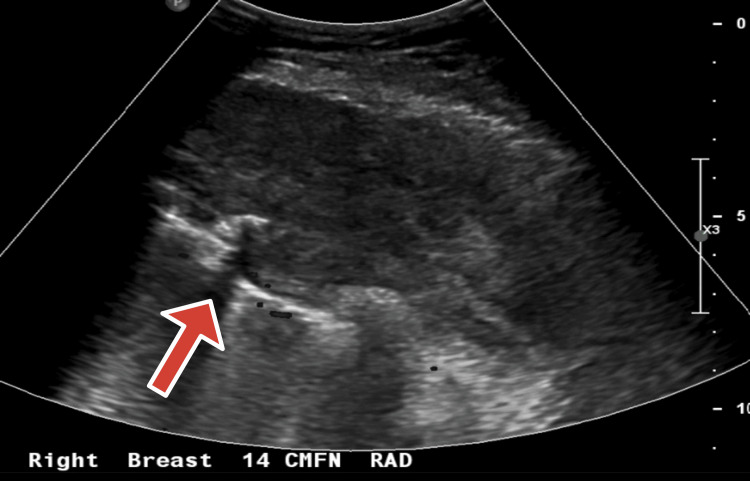 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHistiocytic Disorders and Treatments · Skin Diseases and Diabetes · Lymphadenopathy Diagnosis and Analysis
Introduction
Langerhans cell histiocytosis (LCH) is a clonal proliferation of myeloid dendritic cells, rare in adults with an estimated incidence of 1-2 per million [1,2]. Chest wall involvement, such as rib or sternal lesions, is exceedingly uncommon and frequently misinterpreted as bone malignancy or infection [3-5].
Radiographically, LCH may mimic neoplastic processes due to findings such as rib erosion and soft-tissue extension, underscoring the importance of obtaining tissue diagnosis [6]. Molecular profiling has revealed activating mutations in the mitogen-activated protein kinase (MAPK) pathway, particularly the B-Raf proto-oncogene, serine/threonine-protein kinase (BRAF) V600E mutation, in approximately 40%-60% of adult LCH cases. This has enabled the use of targeted BRAF/mitogen-activated protein kinase kinase (MEK) inhibitors [7,8].
We present an adult case of chest wall LCH mimicking malignancy, complicated by refractory wound drainage, and successfully treated with dabrafenib and trametinib.
Case presentation
A 52-year-old woman with Class III (severe) obesity; body mass index (BMI) 41.6, hypertension, and newly diagnosed type 2 diabetes presented with a painful right chest wall mass that developed following severe bouts of coughing during coronavirus disease 2019 (COVID-19) approximately five months prior to presentation [9]. Initially suspected to represent a rib fracture, the lesion progressively enlarged, prompting further evaluation.
Mammography revealed fatty-replaced breasts with focal asymmetry, calcifications, and axillary lymph nodes. Ultrasound demonstrated a heterogeneous 9.1 × 0.5 cm mass in the right anterior chest wall extending to the subpleural space (Figure 1). Chest computed tomography (CT) showed a 9.7 × 6.4 × 10.2 cm lobulated mass eroding the T3 rib and indenting the pleura, with extension between the T3-T6 ribs and an associated 3.3 × 2.1 cm anterior mediastinal lesion; no lymphadenopathy was identified (Figure 2).
Ultrasound showing a heterogenous mass in the right anterior chest wall, extending to the subpleural spaceArrow pointing at heterogeneous mass
Chest CT with lobulated mass eroding the T3 rib and indenting the pleura, with extension between T3 and T6 ribs and an associated 3.3 × 2.1 cm anterior mediastinal lesionArrow pointing at lobulated massCT, computed tomography
Two months later, incision and drainage of a retropectoral abscess, debridement (4 × 5 × 6 cm), and sinus tract excision were performed. Preliminary pathology showed histiocytes, acute and chronic inflammation, multinucleated giant cells, necrosis, and granulation tissue. Cultures grew Staphylococcus epidermidis; fungal and acid-fast bacilli (AFB) cultures were negative. A 10-day course of levofloxacin was administered, resulting in initial improvement.
Final pathology (one month after the procedure) confirmed LCH with histiocytes extending to the surgical margins. Immunohistochemical staining demonstrated positivity for cluster of differentiation 1a (CD1a), S100 protein (S100), and langerin (CD207), consistent with LCH. Molecular testing identified a BRAF V600E mutation using polymerase chain reaction-based analysis.
Despite multiple attempts at wound closure and a course of trimethoprim-sulfamethoxazole, drainage and bleeding persisted. Approximately two months later, the patient commenced targeted therapy with dabrafenib and trametinib, resulting in complete wound resolution. At the three-month follow-up, she was asymptomatic with minimal residual skin changes.
Discussion
Adult chest wall LCH is exceedingly rare, with only a handful of rib or sternal lesions reported in the literature [3-5]. The scarcity of documented cases makes clinical suspicion challenging, particularly when imaging reveals aggressive features such as cortical destruction and pleural invasion that can mimic malignancy and delay diagnosis [4].
Approximately 40%-60% of adult LCH cases harbor the BRAF V600E mutation, which drives disease pathogenesis and enables the use of molecularly targeted therapy [7,8,10]. Early pediatric trials of dabrafenib, alone or in combination with trametinib, demonstrated high response rates and durable remissions, and subsequent adult case series have reported similarly favorable outcomes [11-13]. The recent tissue-agnostic approval by the U.S. Food and Drug Administration (FDA) of dabrafenib and trametinib for BRAF V600E-mutated solid tumors further supports their role in histiocytic neoplasms [14].
In the present case, impaired wound healing and persistent drainage were likely exacerbated by diabetes and local infection, both well-recognized barriers to recovery in hyperglycemic patients. Chronic hyperglycemia is associated with macrophage dysfunction, impaired neutrophil chemotaxis and phagocytosis, reduced angiogenesis, and delayed granulation tissue formation, all of which contribute to impaired wound healing and increased susceptibility to infection [15,16]. Durable lesion resolution occurred only after systemic disease control with combined BRAF/MEK inhibition, underscoring the importance of addressing underlying disease activity when conventional surgical or antibiotic interventions fail [12,13].
This case emphasizes that LCH should remain in the differential diagnosis for destructive chest wall lesions in adults. Early histopathologic confirmation and molecular profiling are essential to guide effective management, avoid unnecessary repeat operations, and improve overall outcomes [3].
Conclusions
This case emphasizes that adult chest wall masses with aggressive radiographic features may represent LCH rather than malignancy. Accurate diagnosis requires biopsy and molecular testing. In BRAF V600E-positive disease, targeted therapy with dabrafenib and trametinib can provide rapid, durable control, even when surgical interventions are complicated by infection and impaired healing. Incorporating LCH into the differential diagnosis of chest wall tumors is critical to avoid misdiagnosis and to guide patients toward effective, precision-based treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Incidence, prevalence and survival in patients with Langerhans cell histiocytosis: a national registry study from England, 2013-2019 Br J Haematol Liu H Stiller CA Crooks CJ 72873819920223612257410.1111/bjh.18459 PMC 9826274 · doi ↗ · pubmed ↗
- 2Langerhans-cell histiocytosis N Engl J Med Allen CE Merad M Mc Clain KL 85686837920183015739710.1056/NEJ Mra 1607548 PMC 6334777 · doi ↗ · pubmed ↗
- 3Langerhans cell histiocytosis of the rib presenting with pathological fracture: a case report J Cardiothorac Surg Zuo T Jiang P Yu J Zhao K Liu Y Chen B 3321520203322594710.1186/s 13019-020-01368-9PMC 7682065 · doi ↗ · pubmed ↗
- 4Langerhans cell histiocytosis of the rib in an adult: a case report and review of the literature Int J Surg Case Rep Zhao S Luo C Tang B Chen L Xiang M Dai J Li H 1074329720223593986410.1016/j.ijscr.2022.107432 PMC 9403175 · doi ↗ · pubmed ↗
- 5Langerhans cell histiocytosis of the rib of an adult female patient: a case report Investig Magn Reson Imaging Oh CH Kang WY Lee OJ 6165242020
- 6Genetic homogeneity of adult Langerhans cell histiocytosis lesions: insights from BRAF(V 600E) mutations in adult populations Oncol Lett Selway JL Harikumar PE Chu A Langlands K 444944541420172908544110.3892/ol.2017.6774 PMC 5649643 · doi ↗ · pubmed ↗
- 7Recurrent BRAF mutations in Langerhans cell histiocytosis Blood Badalian-Very G Vergilio JA Degar BA 1919192311620102051962610.1182/blood-2010-04-279083 PMC 3173987 · doi ↗ · pubmed ↗
- 8Mutually exclusive recurrent somatic mutations in MAP 2K 1 and BRAF support a central role for ERK activation in LCH pathogenesis Blood Chakraborty R Hampton OA Shen X 3007301512420142520214010.1182/blood-2014-05-577825 PMC 4224195 · doi ↗ · pubmed ↗