Adopting telehealth for mental health support in stroke rehabilitation in Sub-Saharan Africa: A conceptual analysis using Rogers’ Diffusion of Innovation Theory
Delight Tsogbe, Tettey Martin, Akuffo Bernice Gyanmea, Razak Gyasi, Razak Gyasi

TL;DR
This paper explores how telehealth can improve mental health support for stroke rehabilitation in Sub-Saharan Africa, using a theory to understand adoption challenges and solutions.
Contribution
The study applies Rogers’ Diffusion of Innovation Theory to analyze telehealth adoption for mental health in stroke rehabilitation in Sub-Saharan Africa.
Findings
Telehealth adoption is influenced by cultural compatibility, simplicity, and perceived benefits.
Successful telehealth initiatives in SSA require localized adaptation and user engagement.
Policy alignment and capacity-building are critical for effective telehealth implementation.
Abstract
Stroke rehabilitation in Sub-Saharan Africa (SSA) faces persistent gaps in mental health service integration. Post-stroke depression, anxiety, and cognitive impairments remain underdiagnosed due to workforce shortages, stigma, and infrastructural constraints. Telehealth technologies offer a potential mechanism to expand access to psychological care, yet adoption across SSA remains uneven. This paper provides a conceptual, theory-driven synthesis exploring telehealth adoption for mental health support in stroke rehabilitation across SSA, guided by Rogers’ Diffusion of Innovation Theory. A structured conceptual review was conducted using literature from PubMed, Scopus, AJOL, and Google Scholar (2005–2024). Inclusion criteria focused on SSA studies addressing telehealth or mHealth in mental health or rehabilitation contexts. Thematic synthesis was guided by Rogers’ five innovation…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
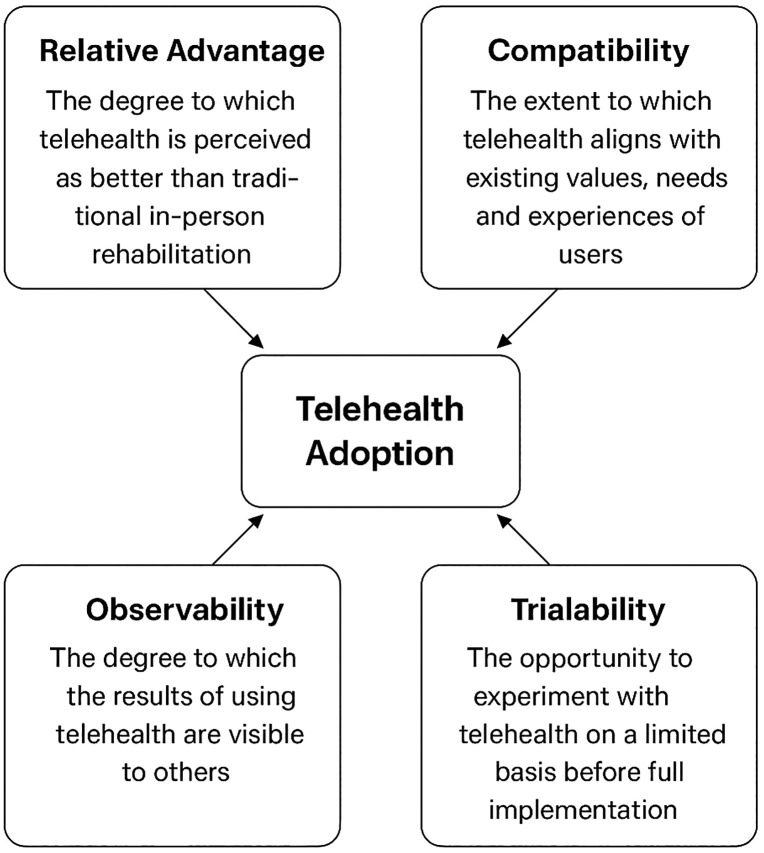 Fig 1
Fig 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStroke Rehabilitation and Recovery · Telemedicine and Telehealth Implementation · Acute Ischemic Stroke Management
Introduction
Stroke remains one of the leading causes of disability and mortality in Sub-Saharan Africa (SSA). The mental health sequelae of stroke, such as depression, anxiety, and cognitive impairment, significantly reduce recovery outcomes. However, mental health services are severely limited due to infrastructural barriers, insufficient specialists, and sociocultural stigma [1,2].
Telehealth, encompassing video consultations, mobile health (mHealth), and remote rehabilitation, has emerged as a potential solution to overcome geographic and workforce barriers [3]. Despite increasing attention, telehealth adoption in SSA remains inconsistent, constrained by cost, digital literacy, and fragmented policy environments [4].
To understand these challenges conceptually, this paper applies Rogers’ Diffusion of Innovation Theory [5] to synthesize evidence on telehealth adoption for mental health support in stroke rehabilitation across SSA.
Methods
Conceptual design
This study adopts a theory-driven conceptual synthesis approach using Rogers’ Diffusion of Innovation Theory as the analytical framework. The approach integrates existing empirical and theoretical evidence to derive implementation insights rather than generating primary data.
Theoretical framework
Rogers’ Diffusion of Innovation Theory provides a systematic lens for understanding how new technologies, such as telehealth, are adopted within health systems. The theory categorizes adopters into five groups, innovators, early adopters, early majority, late majority, and laggards, each differing in their readiness to embrace innovation. It also identifies five key innovation attributes that influence adoption decisions: relative advantage (the perceived improvement over existing methods), compatibility (alignment with users’ values and needs), complexity (ease of use), trialability (the ability to experiment on a limited basis), and observability (visibility of benefits and outcomes). Applying this framework offers a structured understanding of how telehealth can be effectively adopted to provide mental health support during stroke rehabilitation across Sub-Saharan Africa, highlighting the social, technological, and contextual factors that shape diffusion dynamics. A schematic representation of these five innovation attributes and their relationship to telehealth adoption in stroke rehabilitation is illustrated in Fig 1.
The five innovation attributes influencing telehealth adoption in stroke rehabilitation (adapted from Rogers, 2003).
Search strategy
Databases searched included PubMed, Scopus, AJOL, and Google Scholar between 2005 and 2024. Search terms included:
“telehealth”, “mental health”, “stroke rehabilitation”, “Sub-Saharan Africa”, “digital health”, and “Diffusion of Innovation Theory”.
Inclusion criteria
Focus on Sub-Saharan AfricaTelehealth or mHealth interventions for mental health or stroke rehabilitationArticles discussing implementation, barriers, or adoption outcomesPeer-reviewed or credible institutional reports
Exclusion criteria
Non-SSA contextsStudies unrelated to telehealth or mental healthCommentary pieces lacking implementation evidence
Data extraction and synthesis
Eligible studies were screened manually and coded under Rogers’ five innovation attributes. Key data extracted included country, intervention type, health condition, findings, and coded attribute. Reporting transparency followed ENTREQ and PRISMA-ScR recommendations. A summary of the reviewed studies across Sub-Saharan Africa is presented in Table 1.
Table 1: Summary of Reviewed Studies (2005–2024).
Results and discussion
Compatibility
Telehealth initiatives aligning with local clinical routines and cultural contexts show better uptake. Culturally adapted interventions, such as Ghana’s community telepsychiatry model, demonstrated higher engagement due to language inclusivity and integration with existing health infrastructure [6]. Lack of alignment with cultural norms or poor stakeholder involvement often hinder scalability [7].
Complexity
Adoption depends heavily on technology usability and digital literacy. Simplified platforms with training modules have succeeded in Kenya and Ethiopia [8]. Conversely, high system complexity, unstable connectivity, and English-only interfaces create barriers for rural populations [9].
Relative advantage
Perceived benefits, such as reduced travel costs, improved access to specialists, and enhanced continuity of care, drive adoption. Evidence from South Africa and Nigeria indicates that telehealth can complement face-to-face models by reducing logistical burdens [10,11].
Trialability and observability
Pilot programs in Ghana and Uganda improved stakeholder trust by allowing experimentation in controlled settings. Observable benefits, such as improved therapy attendance and patient satisfaction, further encouraged diffusion [12]. Documented visibility of success is a strong determinant of scaling efforts across SSA [13].
Critical appraisal of evidence
Most studies reviewed were small-scale or pilot interventions, limiting generalizability. Few reported long-term outcomes or cost-effectiveness analyses. The evidence base remains fragmented, highlighting the need for empirical studies that measure clinical outcomes, sustainability, and economic viability.
Equity and ethical considerations
Digital health adoption in SSA must address digital exclusion, particularly among rural women, the elderly, and low-literacy groups [14]. Ethical concerns around data privacy, informed consent, and trust are also significant, given limited digital governance structures. Culturally sensitive design and strong data protection frameworks are essential for equitable telehealth expansion.
Policy and implementation recommendations
Integrate telehealth within national eHealth and UHC frameworks.Establish digital literacy training for health workers and patients.Support pilot-to-scale pathways through public-private partnerships.Ensure affordable digital infrastructure and regulatory oversight.Align strategies with African Union’s Digital Health Strategy (2023).
Conclusion
Telehealth represents a transformative opportunity to strengthen post-stroke mental health rehabilitation in SSA. Adoption success depends on alignment with cultural and infrastructural realities, simplicity of design, visible benefits, and supportive policy ecosystems. A systems-level, equity-focused approach can ensure that telehealth advances inclusion rather than exacerbating digital divides.
Limitations
This conceptual synthesis draws on secondary literature and does not include primary data collection. Findings depend on the quality and availability of existing evidence, which varies across SSA contexts.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Adjorlolo S, Ellingsen G. Readiness assessment for implementation of electronic patient record in Ghana: a case of university of Ghana hospital. Journal of Health Informatics in Developing Countries. 2013;7(2).
- 2Hackett ML, Köhler S, O’Brien JT, Mead GE. Neuropsychiatric outcomes of stroke. Lancet Neurol. 2014;13(5):525–34. doi: 10.1016/S 1474-4422(14)70016-X 24685278 · doi ↗ · pubmed ↗
- 3Kruse CS, Krowski N, Rodriguez B, Tran L, Vela J, Brooks M. Telehealth and patient satisfaction: a systematic review and narrative analysis. BMJ Open. 2017;7(8):e 016242. doi: 10.1136/bmjopen-2017-016242 28775188 PMC 5629741 · doi ↗ · pubmed ↗
- 4Fatehi F, Samadbeik M, Kazemi A. What is digital health? Review of definitions. Integrated citizen centered digital health and social care. IOS Press. 2020. p. 67–71.10.3233/SHTI 20069633227742 · doi ↗ · pubmed ↗
- 5Rogers EM. Diffusion of Innovations. 5th ed. New York: Free Press; 2003.
- 6Keteku-Atiemo WI. An Evaluation Of A Telehealth Intervention For A Chronic Care Group In Accra, Ghana (Doctoral dissertation, University of Ghana).
- 7Manyazewal T, Woldeamanuel Y, Blumberg HM, Fekadu A, Marconi VC. The potential of digital health technologies in African context, Ethiopia. med Rxiv. 2021 Mar 29:2021-03.10.1038/s 41746-021-00487-4PMC 837101134404895 · doi ↗ · pubmed ↗
- 8Dodoo JE, Al-Samarraie H, Alzahrani AI. Telemedicine use in Sub-Saharan Africa: Barriers and policy recommendations for Covid-19 and beyond. Int J Med Inform. 2021;151:104467. doi: 10.1016/j.ijmedinf.2021.104467 33915421 PMC 9761083 · doi ↗ · pubmed ↗