The Effectiveness of Respiratory Syncytial Virus Prophylaxis Programme using Palivizumab in Preterm Infants: A single institute retrospective study
Hilal Al Mandhari, Saif Al Kendi, Noura Al-Balushi, Aqeela Bintaqi, Abdulrahman Al Saadi, Mohamed Abdellatif

TL;DR
This study evaluated how well a program using Palivizumab to prevent RSV in preterm infants worked, finding it effective with low hospitalization rates.
Contribution
This is the first evaluation of RSV immunoprophylaxis in Oman among high-risk preterm infants.
Findings
Only 1.8% of preterm infants receiving Palivizumab experienced RSV-related hospitalizations.
Infants born before 28 weeks and those with bronchopulmonary dysplasia were at higher risk for RSV hospitalization.
The study supports the effectiveness of RSV prophylaxis in reducing hospitalizations among high-risk preterm infants.
Abstract
This study aimed to evaluate the effectiveness of an established respiratory syncytial virus (RSV) prophylaxis programme by assessing RSV-related hospitalisations (RSVH) and identify associated risk factors among preterm infants born at <32 weeks' gestation. This retrospective cohort study was conducted at Sultan Qaboos University Hospital, Muscat, Oman. Eligible participants were preterm infants <32 weeks' gestation, born between January 2015 and December 2020, who received RSV prophylaxis. Data were extracted from electronic medical records and analysed. A total of 282 infants were included. The mean gestational age was 28.56 ± 2.03 weeks and the mean birth weight was 1.23 ± 0.35 kg. A total of 5 infants (1.8%) experienced RSV-related hospitalisation while receiving palivizumab prophylaxis. Infants with RSVH were significantly more likely to be born at <28 weeks' gestation than…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
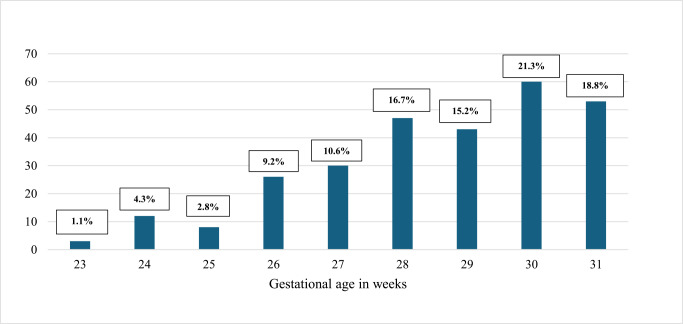 Fig. 1
Fig. 1| Reasons for exclusion | N |
|---|---|
| Transferred out | 16 |
| Non-Omani | 2 |
| Multiple congenital malformations | 2 |
| Did not received PVZ | 4 |
|
| |
| Total | 24 |
| n (%) | ||||
|---|---|---|---|---|
|
| ||||
| Characteristic | Total (N = 282) | Hospitalised (n = 5) | Non-hospitalised (n = 277) | |
| Gender (female) | 140 (49.6) | 4 (80.0) | 136 (49.1) | 0.358 |
| SVD | 123 (43.6) | 3 (60.0) | 120 (43.3) | 0.77 |
| Birth weight (<1 kg) | 75 (26.6) | 3 (60.0) | 72 (26.0) | 0.232 |
| Extreme preterm (<28 weeks) | 78 (27.7) | 4 (80.0) | 74 (26.7) |
|
| Incomplete course (<5 doses) | 107 (37.9) | 0 (0) | 107 (38.6) | 0.194 |
| Non-RSV respiratory viruses-related admissions | 107 (37.9) | 3 (60.0) | 104 (37.5) | 0.315 |
| BPD | 42 (14.9) | 3 (60.0) | 39 (14.1) |
|
| Seasonal birth | 156 (55.3) | 1 (20.0) | 155 (56.0) | 0.251 |
| Received 2 seasons | 79 (28.0) | 3 (60.0) | 76 (27.4) | 0.269 |
| Received 1 season | 203 (72.0) | 2 (40.0) | 201 (72.6) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRespiratory viral infections research · Neonatal Respiratory Health Research · Delphi Technique in Research
1. Introduction
Respiratory syncytial virus (RSV) is among the leading viral pathogens and a common cause of lower respiratory tract infections (LRTIs) in infants.^1^ Specific populations are at a higher risk for developing severe RSV LRTIs due to pre-existing chronic health conditions.^2^ These individuals include healthy term infants under 3 months of age, preterm infants, children with congenital heart disease (CHD), chronic lung disease (CLD) and those with neuromuscular disorders.^23^
Preterm infants are particularly vulnerable to infections due to their immature immune system and CLD, often resulting from bronchopulmonary dysplasia (BPD).^456^ Preterm infants who contract RSV are more likely to experience complications, require hospitalisation in the paediatric intensive care unit (PICU) and need both non-invasive and invasive mechanical ventilation compared to other RSV-infected patients.^7^
Palivizumab (PVZ) is a humanised monoclonal antibody targeting the RSV-F protein.^8^ It is administered once a month at a dose of 15 mg/kg intramuscularly for a total of 5 doses. It has been shown that the use of PVZ can reduce the severity of infections and result in a reduced rate of hospitalisation related to RSV infection.^9^ PVZ is recommended for individuals at risk of developing severe RSV-related illnesses to decrease the prevalence and severity of the disease. The National Advisory Committee on Immunization has provided updated recommendations for using PVZ to prevent RSV complications in infants at risk.^10^ A working group conducted systematic reviews on RSV burden and PVZ effectiveness to support these recommendations.^11^ PVZ prophylaxis has significantly reduced the risk of RSV hospitalisation in infants at high risk of severe RSV infection.^12^
In Oman, the live birth rate in 2020 was 80,959, with approximately 10% of these births being preterm less than 37 weeks.^13^ There is currently no national RSV immunoprophylaxis programme in Oman, and RSV immunoprophylaxis is only offered at two individual tertiary healthcare institutions within the country. There are no studies that have investigated the impact of RSV immunoprophylaxis in preterm infants in Oman yet. Therefore, this study was designed and conducted with the primary objective of assessing the outcome of the RSV immunoprophylaxis programme using PVZ and, secondarily, to identify key risk factors associated with RSV-hospitalisation (RSVH) among preterm infants who received RSV prophylaxis.
2. Methods
This retrospective cohort study was conducted at Sultan Qaboos University Hospital, an academic perinatal centre in Oman with an annual delivery rate of 3,000–4,000. It is also a referral centre for surgical, metabolic and complex neonatal cases from all over the country. RSV prophylaxis is administered to at-risk infants and children including preterm infants born <32 weeks of gestation and are <6 months of age at the start of RSV season, infants born at ≤28 weeks of gestation and are <12 months at the start of RSV season and infants/children with haemodynamically significant CHD and BPD/CLD who are younger than 24 months at the start of RSV season. The first dose is administered before discharge if a patient is discharged home during the RSV season and subsequent doses are administered in an outpatient setting every 4 weeks for a total of 5 doses between September and March.
Eligible individuals were preterm infants born at less than 32 weeks' gestation who received RSV prophylaxis, including those born at Sultan Qaboos University Hospital (inborn) and those born at other healthcare facilities and subsequently referred to SQUH (outborn), between January 2015 and December 2020. Individuals were excluded if they were non-Omani infants, had never received RSV prophylaxis, had died during NICU stay, had multiple congenital anomalies or were transferred to other health institutions during the NICU stay.
BPD was defined according to the 2018 National Institute of Child Health and Human Development workshop definition and classified as the need for respiratory support or oxygen at a postmenstrual age (PMA) of 36 weeks.^14^ RSVH was defined as hospitalisation due to bronchitis/pneumonia with a positive RSV PCR while receiving RSV prophylaxis during the season of RSV. The RSV season was defined as the period from September of one year to March of the following year. An incomplete RSV prophylaxis course was defined as any course less than 5 doses. Extreme low birth weight (ELBW) was defined as a birth weight less than 1,000 g.
The primary outcome of the study was the rate of hospitalisation due to RSV infection among preterm infants who received PVZ prophylaxis. The secondary outcome included the risk factors associated with RSVH in preterm infants who receive PVZ prophylaxis.
A predefined data set was collected from the hospital's electronic patient records. Data included gestational age, birth weight, gender, mode of delivery, year of birth, month of birth, month of discharge, PMA at discharge, respiratory status at post-PMA of 36 weeks, diagnosis of BPD, discharge on home oxygen, chronologic age at the beginning of first RSV season (September of the year), corrected age at the beginning of first RSV season (September), number of doses of RSV prophylaxis in first season, if received during a second season and the number of doses as well RSV-related hospitalisation during the RSV season (September–March). For each RSVH, the following data were also collected: age at admission, need for non-invasive ventilation (NIV) respiratory support, need for admission to the ICU, need for intubation and invasive ventilation, length of stay for each hospitalisation and outcome (survival or death).
The data analysis was done using Statistical Package for Social Sciences (SPSS) software, Version 26 (IBM Corp., Armonk, New York, USA). Continuous variables were expressed as mean ± standard deviation or median and interquartile range (IQR), while categorical variables were reported as frequencies and percentages. The study population was categorised into two groups: RSV-hospitalised and non-hospitalised groups. The differences in variables between the two groups was compared and assessed using the Chi-square test for categorical variables and the T-test or the Mann-Whitney test for continuous variables. A P value of less than 0.05 indicated a significant association.
3. Results
A total of 306 infants <32 weeks of gestation were eligible for the study during the specified period but 24 were excluded due to the exclusion criteria [Table 1]. Therefore, a final total of 282 preterm infants <32 weeks received RSV prophylaxis during the study period and were included. The gender distribution was fairly balanced, with 142 males (50.4%) and 140 females (49.6%). The mean gestational age was 28.56 ± 2.03 weeks and the mean birth weight was 1.23 ± 0.35 kg [Fig. 1].
Within the total cohort of 282, 5 (1.8%) had seasonal RSVH while receiving seasonal RSV prophylaxis and 275 (98.2%) did not have seasonal RSVH while receiving RSV prophylaxis. While there was an approximately equal distribution of males and females in the cohort, a higher proportion of females were hospitalised; however, this discrepancy did not reach statistical significance. Moreover, most births were via lower-segment Caesarean section (56.4%), but no significant difference was observed in the mode of delivery between the RSV-hospitalised and non-hospitalised groups who delivery via spontaneous vaginal delivery (SVD) or Caesarean section (SVD: 60% versus 43.3%; P = 0.77). A detailed analysis of birth weight distribution reveals a trend of extremely low birth weights (<1 kg) in those with RSVH, although this finding did not reach statistical significance (60% versus 26%; P = 0.232). Further exploration into gestational age revealed that a significant majority of infants were very preterm (28–32 weeks), or extremely preterm infants (<28 weeks) who were significantly more predisposed to RSVH (80% versus 26.7%; P = 0.033). Incomplete RSV prophylaxis courses (<5 doses) occurred in none of the 5 RSV-hospitalised infants compared to 37.9% of the non-RSVH group. No significant differences were observed between RSV-hospitalised and non-hospitalised in seasonal birth, non-RSVH and in receiving one and two seasons of PVZ. BPD was observed in a total of 42 out of 282 (14.9%). A total of 5 infants with BPD were discharged on home oxygen. Only 1 out of the 5 on home oxygen had RSVH. The RSV-hospitalised group had a significantly higher rate of BPD (60% versus 14.1%; P = 0.026) [Table 2].
Further examination of the clinical severity of RSVH revealed that only 1 infant required NIV, while 2 infants received supplemental oxygen via low-flow nasal cannula. The remaining 2 cases did not require any form of respiratory support. None of the infants required invasive mechanical ventilation or admission to the PICU. The mean chronological age and corrected age at hospitalisation were 8.8 months (range: 3–18 months) and 5.6 months (range: 0–14), respectively. The mean duration of hospital stay was 4.6 days (range: 3–7 days). Importantly, all affected infants recovered fully and were discharged home in a good condition.
Gestational age distribution of the study cohort (N = 282).
4. Discussion
At present, there is no national RSV prophylaxis programme in high-risk infants in Oman. The use of PVZ is presently limited to two non-Ministry of Health healthcare institutions. This study retrospectively reviewed and analysed the impact of the RSV prophylaxis programme established in one of Oman's tertiary healthcare institutions, aiming to ascertain the effectiveness of the programme and determine the risk factors associated with RSVH in infants and children receiving PVZ RSV prophylaxis.
The effectiveness of palivizumab for RSV prophylaxis in preterm infants was first demonstrated in the IMpact RSV study.^9^ The IMpact RSV study showed that PVZ resulted in a 55% reduction in RSVH (10.6% placebo versus 4.8% PVZ). The rate of RSVH was even lower in the current study, as only 1.8% of the population had RSVH. The IMpact RSV study also showed that children with prematurity, but without BPD, had a 78% reduction in the rate of RSVH (8.1% versus 1.8%) and preterm children with BPD had a 39% reduction (12.8% versus 7.9%).^9^ This study reports similarly low rates of RSVH in children with and without BPD (7.1% and 0.83%, respectively). A similar study from the UAE, which included preterm infants <32 weeks who received PVZ prophylaxis, showed a similarly low rate of RSVH of 2.68% (n = 11/410).^15^ These findings demonstrate and support the effectiveness of the RSV prophylaxis programme established at Sultan Qaboos University Hospital.
The risk factors significantly associated with RSVH in this study are extreme prematurity (GA<28 weeks) and BPD. A statistically non-significant trend of increased rate of RSVH was observed in children born ELBW and of the female gender. In the retrospective study by Chida-Nagai et al, the risk factors for RSVH in infants and children who received PVZ were preterm ≤ 28 weeks, BPD and trisomy 21.^16^ Whereas, in the study by Paes et al., hospitalisation rates due to RSV were similar among infants born at or before 32 weeks of gestational age (GA) and those born between 33 and 35 weeks of GA.^17^ While in Mulot et al.'s study, the very severe lower respiratory tract infections (LRTI) correlated with a younger corrected age for prematurity.^3^ Another study by Packnett et al. showed that the risk of RSVH in preterm infants <29 weeks was 3–4 times higher, and ICU admissions and mechanical ventilation were more common during RSVH in very preterm infants compared to term infants.^18^
The strength of this study is that it is the first study reporting the effectiveness of the RSV prophylaxis programme using PVZ in Oman. The duration of 6 years and the total number of preterm infants (<32 weeks) included are relative strengths as well. However, there are limitations to this study worth discussing. Its retrospective design limits its ability to determine causality. The lack of a comparison or control group, the fact that it was a single-centre study and that only RSV hospitalisations at Sultan Qaboos University Hospital could be captured limit the reliability and generalisability of the study.
5. Conclusion
This is the first study from Oman to evaluate the effectiveness of RSV prophylaxis in preterm infants. The low RSVH rate observed supports the programme's success and aligns with international data. Extreme prematurity and BPD emerged as the most significant risk factors for RSVH, underscoring the need for targeted protection. These results advocate for a national RSV prophylaxis policy for high-risk infants in Oman.
Authors' Contribution
Hilal Al Mandhari: Conceptualization, Methodology, validation, Formal analysis, Writing -Original Draft, Writing - Review & Editing, Supervision. Saif Al Kendi: Methodology, Data Curation, Formal analysis. Noura Al-Balushi: Methodology, Data Curation, Writing - Review & Editing. Aqeela Bintaqi: Writing - Review & Editing, Project administration. Abdulrahman Al Saadi: Validation, Writing - Review & Editing. Mohamed Abdellatif: Conceptualization, Validation, Writing - Review & Editing, Supervision.
Ethics Statement
Ethical approval for this study was obtained from the Medical Research Ethical Committee at the College of Medicine and Health Sciences, Sultan Qaboos University, Muscat, Oman (MREC #3020). Ensuring confidentiality is a critical ethical consideration in a retrospective cohort study. Therefore, this research ensured the safeguarding of confidentiality by avoiding the collection of any identifying information from the patients. Each patient was assigned a study code for anonymity. Additionally, the data was stored on password-protected computers to prevent unauthorised access.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
No funding was received for this study.
Data Availability
Data is available upon reasonable request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jain H Schweitzer JW Justice NA. Respiratory Syncytial Virus Infection in Children. 2023 Jun 20. In: Stat Pearls [Internet]. Treasure Island, Florida, USA: Stat Pearls Publishing, 2025.
- 2Rossi GA Medici MC Arcangeletti MC Lanari M Merolla R Paparatti UD Risk factors for severe RSV-induced lower respiratory tract infection over four consecutive epidemics. Eur J Pediatr 2007; 166:1267–72. https://doi.org/10.1007/s 00431-007-0418-y.10.1007/s 00431-007-0418-y 17308898 PMC 2042510 · doi ↗ · pubmed ↗
- 3Mulot G Benchaib M Plaisant F Ploin D Gillet Y Javouhey E Risk Factors of Very Severe RSV Infections in a Multicenter Cohort of Very Preterm and Extreme Preterm Babies Receiving or Not Palivizumab. Front Pediatr 2022; 10:884120. https://doi.org/10.3389/fped.2022.884120.10.3389/fped.2022.88412035874569 PMC 9301069 · doi ↗ · pubmed ↗
- 4Melville JM Moss TJ. The immune consequences of preterm birth. Front Neurosci 2013; 7:79. https://doi.org/10.3389/fnins.2013.00079.10.3389/fnins.2013.0007923734091 PMC 3659282 · doi ↗ · pubmed ↗
- 5Salimi U Dummula K Tucker MH Dela Cruz CS Sampath V. Postnatal Sepsis and Bronchopulmonary Dysplasia in Premature Infants: Mechanistic Insights into “New BPD”. Am J Respir Cell Mol Biol 2022; 66:137–45. https://doi.org/10.1165/rcmb.2021-0353 PS.10.1165/rcmb.2021-0353 PS 34644520 PMC 8845139 · doi ↗ · pubmed ↗
- 6Carpenter TC Stenmark KR. Predisposition of infants with chronic lung disease to respiratory syncytial virus-induced respiratory failure: a vascular hypothesis. Pediatr Infect Dis J 2004; 23:S 33–40. https://doi.org/10.1097/01.inf.0000108191.13799.09.10.1097/01.inf.0000108191.13799.0914730268 · doi ↗ · pubmed ↗
- 7Resch B Kurath S Manzoni P. Epidemiology of respiratory syncytial virus infection in preterm infants. Open Microbiol J 2011; 5:135–43. https://doi.org/10.2174/1874285801105010135.10.2174/187428580110501013522262986 PMC 3258570 · doi ↗ · pubmed ↗
- 8Krivitskaya V Petrova E Sorokin E Tsareva T Sverlova M Komissarova K Characterization of a Panel of Monoclonal Antibodies Targeting the F-Protein of the Respiratory Syncytial Virus (RSV) for the Typing of Contemporary Circulating Strains. Trop Med Infect Dis 2023; 9:1. https://doi.org/10.3390/tropicalmed 9010001.10.3390/tropicalmed 901000138276631 PMC 10819491 · doi ↗ · pubmed ↗