Rare Infection with Precise Detection: Abiotrophia defectiva septic arthritis following anterior cruciate ligament reconstruction
Ahmed Al Mamari, Shouq Al Hudar, Maya Al Salti

TL;DR
A rare case of knee infection caused by Abiotrophia defectiva after surgery was successfully diagnosed and treated using advanced techniques.
Contribution
Demonstrates the effectiveness of enrichment media and advanced diagnostics in identifying fastidious pathogens in postoperative infections.
Findings
Abiotrophia defectiva was identified as the cause of septic arthritis following anterior cruciate ligament reconstruction.
Use of enrichment broth and MALDI-TOF MS enabled detection when standard cultures failed.
Targeted antibiotic therapy and surgical debridement led to full patient recovery.
Abstract
Abiotrophia defectiva, a nutritionally variant streptococcus, is an uncommon yet significant pathogen primarily associated with infective endocarditis and, more rarely, septic arthritis. We report a 23-year-old male patient who presented to a tertiary care centre in Rustaq, Oman, in 2024 with right knee pain and fever following an anterior cruciate ligament reconstruction. Standard cultures remained negative, but enrichment broth and matrix-assisted laser desorption/ionisation time-of-flight mass spectrometry enabled prompt identification of A. defectiva. Subsequently, the patient was diagnosed with native knee septic arthritis due to A. defective. Following surgical debridement, the patient completed a 4-week course of targeted antibiotic therapy, resulting in full recovery and normalisation of inflammatory markers. This case highlights the value of enrichment media and advanced…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
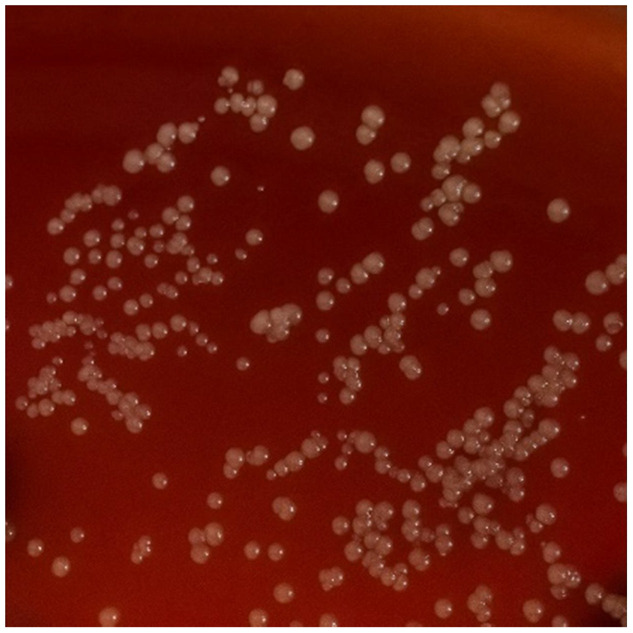 Fig. 1
Fig. 1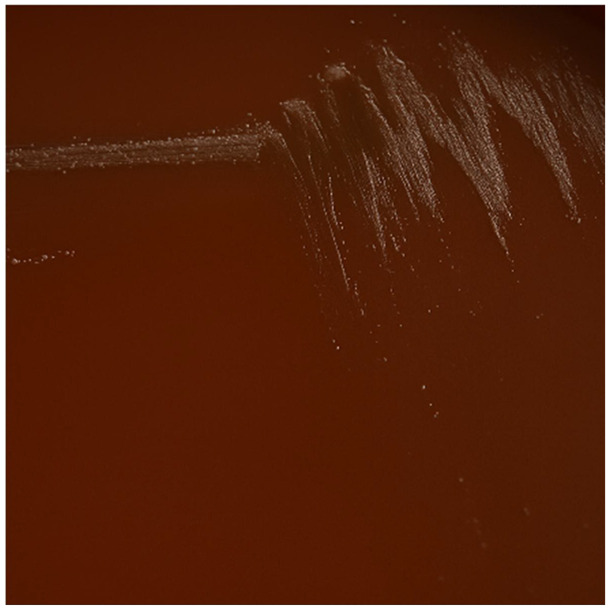 Fig. 2
Fig. 2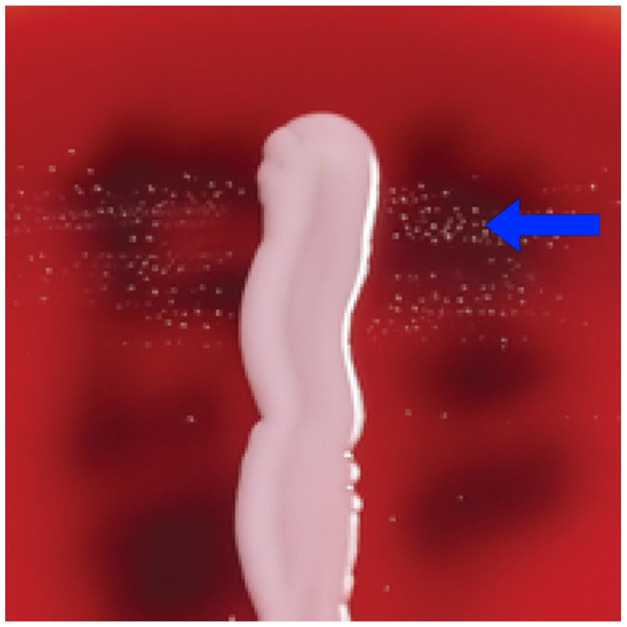 Fig. 3
Fig. 3| Day | Clinical course and interventions |
|---|---|
| 0 | Arthroscopic anterior cruciate ligament reconstruction performed. |
| 7 | Patient developed right knee pain, fever and generalised body aches. |
| 10 | Presented to the emergency department; laboratory tests revealed elevated CRP and ESR. Patient was discharged with a prescription for oral amoxicillin-clavulanate. |
| 12 | Orthopaedic clinic; synovial fluid was aspirated and arthroscopic washout was performed. IV cloxacillin therapy was initiated. |
| 14 | Enrichment broth culture yielded gram-positive cocci; organism identified as |
| 14–28 | IV ceftriaxone was initiated as targeted therapy. |
| 28–42 | Transitioned to oral levofloxacin, completing a 4-week course of antimicrobial therapy. |
| 63 | Achieved full clinical recovery with normalisation of inflammatory markers and restoration of knee function. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Infections and Treatments · Infective Endocarditis Diagnosis and Management · Bacterial Identification and Susceptibility Testing
1. Introduction
Infection following anterior cruciate ligament reconstruction (ACLR) is uncommon, with reported rates ranging from 0.4–1.4%. When it occurs, it can lead to serious complications, including articular cartilage damage, arthrofibrosis and both local and systemic infections. Staphylococcus aureus and coagulase-negative staphylococci are the predominant pathogens, accounting for 60–90% of postoperative ACLR infections.^1^ However, atypical organisms may also be responsible and are often more challenging to detect. Accurate identification of these atypical pathogens is crucial for guiding effective antimicrobial therapy.^2^ Abiotrophia defectiva is a rare cause of septic arthritis, with only a few native joint cases reported in the literature.^34^ In this report, we present an additional case of native knee septic arthritis caused by A. defectiva following ACLR.
2. Case report
A 23-year-old male presented to the emergency department of a tertiary care centre in Rustaq, Oman, in 2024 with a 3-day history of right knee pain and fever (38 °C). He had undergone right knee ACLR 10 days earlier for a traumatic sports-related injury and had received routine surgical prophylaxis. He had no known medical comorbidities, was not taking any regular medications, had no known drug allergies and reported no dental procedures within the past 3 months.
On examination, the surgical wound appeared clean and dry without signs of inflammation. The remainder of the clinical assessment was unremarkable. Laboratory investigations revealed a white blood cell count of 8.47 × 10^3^/μL (6.1 × 10^3^/μL neutrophils), haemoglobin of 11.26g/dL, platelet count of 313 × 10^9^/L, C-reactive protein (CRP) of 236mg/L and erythrocyte sedimentation rate (ESR) of 102mm/h. Renal function and electrolyte levels were within normal limits. A sterile dressing was applied and the patient was discharged on oral amoxicillin-clavulanate 625mg 3 times daily for 5 days, with a follow-up appointment scheduled at the orthopaedic clinic in 2 days. Given that symptoms appeared within 10 days post-ACLR, the presentation was consistent with an acute surgically related infection.
He was seen in the orthopaedic clinic 2 days later, still complaining of right knee pain, fever and generalised body aches. On examination, the knee was swollen, tender and exhibited mildly restricted range of motion, while the surgical wound remained dry and clean. A synovial fluid aspiration under aseptic conditions yielded a bloody effusion, which was sent for analysis and culture. Given the concern for infection, an emergency arthroscopic washout of the knee was performed. During the procedure, extensive synovitis with soft tissue fibrosis was found, with an intact ACL graft and no gross injury. Debridement of fibrotic tissue was performed and the knee was thoroughly irrigated.
Intravenous cloxacillin 2,000 mg 4 times daily was initiated empirically. Synovial fluid was inoculated onto routine media and enrichment broth (paediatric blood culture bottle) to enhance the population density of the possible pathogen. Direct inoculation onto standard media showed no growth after 5 days of incubation. However, the enrichment broth flagged positive after 48 hours. The gram stain revealed gram-positive cocci in chains. The broth was subsequently subcultured, with initial fine growth observed on chocolate agar. Further subcultures were performed on blood, chocolate and MacConkey agars. After 24 hours of incubation, small white colonies grew prominently on blood agar, showed minimal growth on chocolate agar, and no growth on MacConkey agar [Fig. 1,Fig. 2].
Growth of Abiotrophia defectiva colonies on blood agar.
Growth of Abiotrophia defectiva on chocolate agar.
Further biochemical testing confirmed that the organism was catalase-negative, aiding in narrowing the differential diagnosis. A subsequent Gram stain of the cultured isolate revealed gram-positive cocci arranged in pairs and short chains, suggesting a streptococcal species. Additionally, the isolate exhibited a positive satellitism test indicating satellite growth, a distinguishing feature of certain fastidious organisms that depend on specific growth factors [Fig. 3]. Definitive identification was achieved using matrix-assisted laser desorption/ionisation time-of-flight mass spectrometry (MALDI-TOF MS), which confirmed the organism as A. defectiva. A transthoracic echocardiogram was not performed because the infection was localised, the patient was not septic and blood cultures remained negative, excluding the possibility of infective endocarditis (IE). Unfortunately, antibiotic susceptibility testing could not be performed, as the specialised media required were not available at the time.
Satellite growth pattern of Abiotrophia defectiva (blue arrow).
The patient was treated with intravenous ceftriaxone at 2g once daily for 14 days, followed by oral levofloxacin 500mg twice daily for an additional 14 days, for a total antimicrobial treatment duration of 4 weeks. On orthopaedic review 1 month later, there was improvement in his symptoms, but significant muscle wasting, which required rehabilitation with physiotherapy. His white blood cell count, CRP and ESR were all within normal limits; 9 weeks after discharge, he was walking almost normally, with full weight-bearing and a good range of pain-free knee movements [Table 1].
3. Discussion
Abiotrophia species are nutritionally variant streptococci commonly colonising the gastrointestinal, urogenital and upper respiratory tracts as part of normal flora. These organisms account for approximately 1–2% of all cases of IE and are associated with higher morbidity and mortality compared with other streptococcal pathogens. Beyond IE, A. defectiva can cause severe invasive infections such as septic arthritis and brain abscess.^5^ Osteoarticular infections due to A. defectiva are exceptionally rare and have most often been reported in the context of recent dental procedures, arthroscopic interventions or the presence of prosthetic material.^2467^ Generally, this bacterium is unable to grow on standard media. It requires a medium that contains pyridoxal or L-cysteine to grow. This requirement is a challenge in the detection of this organism, making the diagnosis delayed or easily missed.^24^
In contrast to other A. defectiva strains, the current case's isolate unexpectedly grew on blood agar that does not contain supplemental L-cysteine or pyridoxal. Although Gram stains of A. defectiva usually reveal gram-positive cocci, the organisms may exhibit pleomorphism and variable staining characteristics, further complicating early recognition.^5^ Traditional phenotypic identification methods such as analytical profile index panels and automated systems often misidentify or fail to detect these nutritionally demanding bacteria. In contrast, advanced techniques such as MALDI-TOF MS and targeted molecular assays provide rapid and reliable species-level identification of A. defectiva isolates.^8^ When culture-based methods, including enriched media, fail to isolate an organism, metagenomic next-generation sequencing can serve as a valuable adjunct, enabling detection of fastidious or non-culturable pathogens in postoperative infections.^9^
The antimicrobial susceptibility of Abiotrophia species is challenging to determine, owing to their fastidious growth requirements and the lack of readily available testing media. Although many isolates demonstrate susceptibility to agents such as vancomycin, carbapenems, levofloxacin and cephalosporins, marked inter-strain variability has been reported. For example, the A. defectiva C1-2 strain exhibited multidrug resistance to cefazolin, ceftazidime, cefaclor, piperacillin, gentamicin, erythromycin and minocycline, yet remained susceptible to amoxicillin and ceftriaxone.^10^ In the current case, susceptibility testing was not performed as the specialised pyridoxal-supplemented media necessary for reliable assessment were unavailable. Early arthroscopic washout combined with prompt initiation of antimicrobial therapy likely prevented biofilm establishment on the ACL graft.^11^ Biofilm formation is a major concern in surgically related joint infections, as delayed diagnosis or inadequate early treatment may necessitate graft or hardware removal.^12^ In this case, early intervention enabled successful graft preservation and avoidance of revision surgery.
Due to the rarity of musculoskeletal infections caused by A. defectiva, no treatment guidelines exist. Previous reports have described successful management with 3 weeks of intravenous penicillin plus gentamicin followed by 4 weeks of oral levofloxacin in septic arthritis, and with 6 weeks of intravenous ceftriaxone combined with oral levofloxacin in a patient presenting with pseudogout.^34^ In contrast, the current patient achieved complete clinical and biochemical resolution following a 4-week regimen, 2 weeks of intravenous ceftriaxone followed by 2 weeks of oral levofloxacin, without graft removal. Although durations of up to 6 weeks are often recommended for A. defectiva related infections, a shorter course was chosen based on early surgical debridement, absence of prosthetic involvement, rapid normalisation of inflammatory markers and prompt symptomatic improvement.
4. Conclusion
This case highlights the importance of considering fastidious organisms such as A. defectiva in the differential diagnosis of postoperative joint infections. Use of enrichment media and advanced diagnostic techniques such as MALDI-TOF MS are crucial for early detection. A 4-week antibiotic regimen achieved full recovery in this case, suggesting shorter courses may be adequate with prompt surgical and laboratory intervention. Optimising microbiology laboratories to detect rare pathogens can significantly improve patient outcomes.
Authors' Contribution
Ahmed: Visualization, Supervision, Writing – Review & Editing. Shouq Al Hudar: Writing – Original Draft Preparation. Maya Al Salti: Supervision, Writing – Review & Editing.
Declaration of Generative AI Use
Portions of this case report were proofread and edited for clarity and readability with the assistance from ChatGPT. The authors have reviewed and approved all content.
Acknowledgement
The authors would like to acknowledge all healthcare professionals who contributed to the care and management of the patient.
Ethics Statement
Informed consent was obtained from the patient for publication of this case report.
Conflict of Interest
The authors declare no conflicts of interest.
Data Availability
Data is available upon reasonable request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cassano GD Moretti L Vicenti G Buono C Albano F Ladogana T Infection after anterior cruciate ligament reconstruction: A narrative review of the literature. Healthc (Basel) 2024; 12:894. 10.3390/healthcare 12090894.PMC 1108307938727451 · doi ↗ · pubmed ↗
- 2Tooley TR Siljander MP Hubers M. Development of a periprosthetic joint infection by Abiotrophia defectiva years after total knee arthroplasty. Arthroplasty Today 2019; 5:49–51. https://doi.org/10.1016/j.artd.2018.12.002.10.1016/j.artd.2018.12.00231020021 PMC 6470352 · doi ↗ · pubmed ↗
- 3O'Connor KM Williams P Pergam SA. An unusual case of knee pain: Pseudogout and Abiotrophia defectiva infection. South Med J 2008; 101:961–2. 10.1097/smj.0b 013e 31817 fe 04c.18708985 PMC 2735253 · doi ↗ · pubmed ↗
- 4Taylor CE Fang MA. Septic arthritis caused by Abiotrophia defectiva. Arthritis Rheum 2006; 55:976–7. https://doi.org/10.1002/art.22348.10.1002/art.2234817139646 · doi ↗ · pubmed ↗
- 5Wilawer M Elikowski W Greberski K Ratajska PA Welc NA Lisiecka ME. Abiotrophia defectiva endocarditis – Diagnostic and therapeutic challenge: Case report. ID Cases 2023; 34:e 01906. https://doi.org/10.1016/j.idcr.2023.e 01906.10.1016/j.idcr.2023.e 0190637867569 PMC 10585279 · doi ↗ · pubmed ↗
- 6Young JN York J. Abiotrophia causing prosthetic joint septic arthritis. Cureus 2022; 14:e 22801. 10.7759/cureus.22801.35399397 PMC 8980255 · doi ↗ · pubmed ↗
- 7Cassir N Grillo J Argenson J Drancourt M Levy P. Abiotrophia defectiva knee prosthesis infection: A case report. J Med Case Rep 2011; 5:438. https://doi.org/10.1186/1752-1947-5-438.10.1186/1752-1947-5-43821896178 PMC 3177934 · doi ↗ · pubmed ↗
- 8Woo PC Fung AM Lau SK Chan BY Chiu S Teng JL Granulicatella adiacens and Abiotrophia defectiva bacteraemia characterized by 16S r RNA gene sequencing. J Med Microbiol 2003; 52:137–40. https://doi.org/10.1099/jmm.0.04950-0.10.1099/jmm.0.04950-012543919 · doi ↗ · pubmed ↗