Hemichorea-Hemiballismus As Presentation of Toxoplasma gondii Encephalitis in an Immunocompromised Host
Chu Keat Lim, Xiong Khee Cheong, Juen Kiem Tan, Ummu Afeera Zainulabid, Hui Jan Tan, Najma Kori, Petrick Ramesh Periyasamy

TL;DR
A man with advanced HIV developed a rare movement disorder caused by Toxoplasma gondii encephalitis, which improved with timely treatment.
Contribution
This case highlights hemichorea-hemiballismus as a rare but important presentation of Toxoplasma gondii encephalitis in immunocompromised individuals.
Findings
The patient showed clinical and radiological improvement after one month of anti-toxoplasmosis treatment.
Brain imaging revealed a basal ganglia lesion consistent with cerebral toxoplasmosis.
Positive Toxoplasma IgG serology supported the diagnosis in this immunocompromised patient.
Abstract
Toxoplasma gondii encephalitis is a common but serious opportunistic infection in people living with human immunodeficiency virus (PLHIV), particularly those with advanced disease and low CD4 counts. Its classical manifestations include fever, altered mental status, seizures and focal neurological signs. Movement disorders are a less common consequence, with hemichorea-hemiballismus (HCHB) representing a rare but striking manifestation. We describe a 36-year-old man with advanced HIV disease who had defaulted on treatment. He presented with bizarre, involuntary movements of his left upper and lower limbs. His serum Toxoplasma IgG was positive, and brain imaging revealed a basal ganglia lesion leading to the presumptive diagnosis of cerebral toxoplasmosis. He was treated with anti-toxoplasmosis and anti-dyskinetic medications, achieving both clinical and radiological resolution after one…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
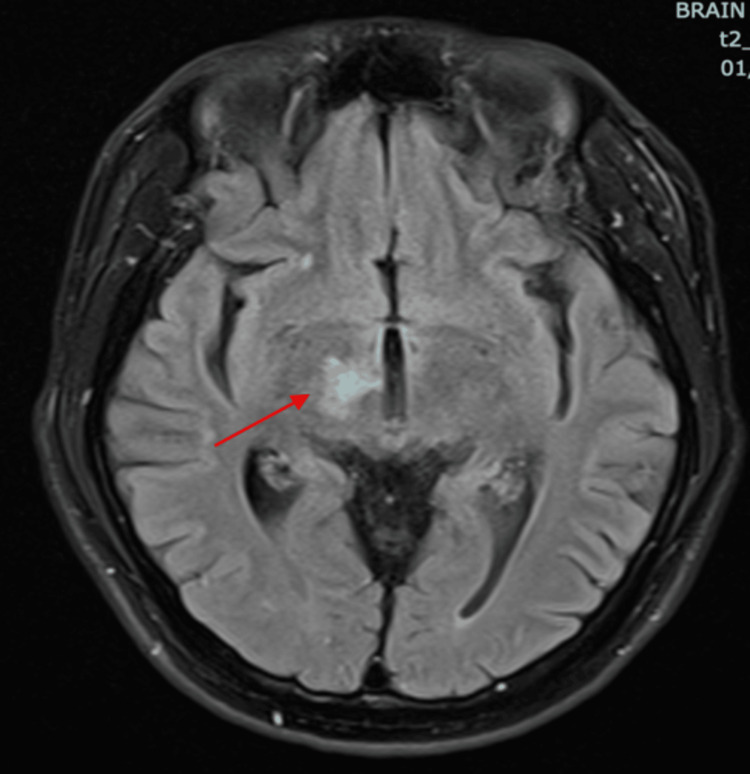 Figure 1
Figure 1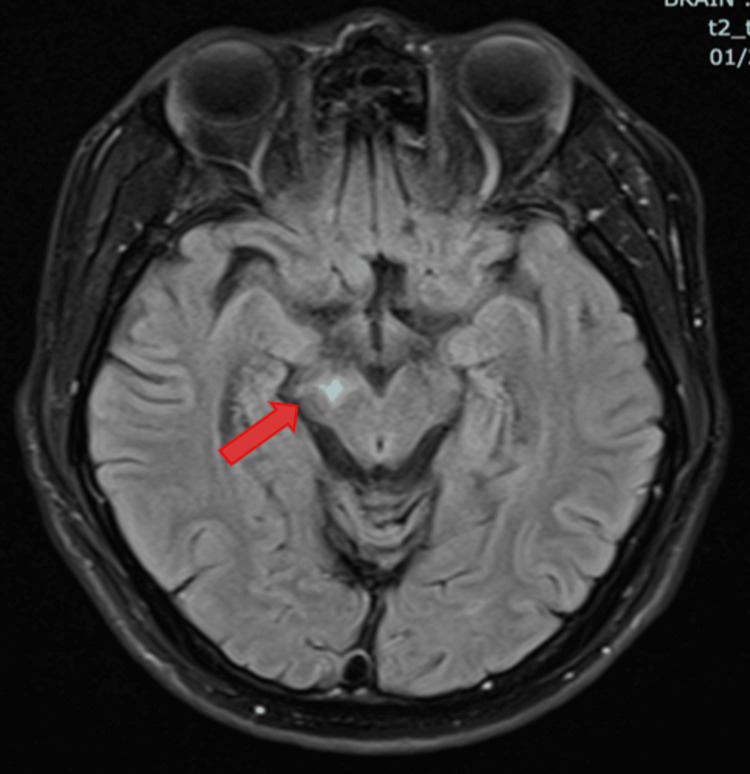 Figure 2
Figure 2| Investigations | Results | Normal Range |
| Blood | ||
| White cell count | 4.5 x109/L | 4.5-11.0 x109/L |
| CD4 count | 4* cell/uL | 500 -1500 cell/uL |
| HIV Viral load PCR | 398,000* copies/mL | Not detected copies/mL |
| Toxoplasma IgG | Reactive* | Non-reactive |
| Cryptococcal Antigen | Non-reactive | Non-reactive |
| Rapid Plasma Reagin (RPR) | Non-reactive | Non-reactive |
| Cerebrospinal Fluid (CSF) | ||
| Opening Pressure | 5 cmH20 | 10 – 20 cmH2O |
| White blood cells | No cell seen | 0 – 5 cell/µL |
| Protein | 0.59* g/L | 0.15 – 0.45 g/L |
| Glucose | 4.1 mmol/L | 2.8 – 4.2 mmol/L |
| Meningitis panel PCR for virus & bacteria | Not detected | Not detected |
| MTB PCR | Not detected | Not detected |
| MTB Culture | No growth | No growth |
| Case, year | Age, gender | Movement disorder | Causative agent (s) | Affected central nervous system site (s) | Treatment | Time interval to Complete Resolution of Symptoms |
| Samira Rabhi et al. (2011) [ | 59, female | HCHB | Cerebral toxoplasmosis | Right capsule thalamic focal lesion | Trimethoprim-sulfamethoxazole, steroid | 2 weeks |
| Reyes et al. (2016) [ | 22, male | Unilateral choreoathetosis, cognitive decline (MMSE 5) on presentation | Cerebral toxoplasmosis, secondary syphilis | Right parietal-temporal lobes, bilateral frontal, basal ganglia, thalamus region | Trimethoprim-sulfamethoxazole, intravenous penicillin for 10 days, antiretroviral therapy, carbamazepine for 6 days, phenytoin | 4 months |
| Magano et al. (2016) [ | 26, male | Hemiballismus | Cerebral toxoplasmosis | Lower left and right cerebellar hemisphere, thalamus- mesencephalic, extension to internal capsule | Pyrimethamine, clindamycin, antituberculosis (isoniazid, rifampicin, ethambutol, pyrazinamide) surgery, stereotactic right pallidotomy on day 46, therapy due to refractory movement. An antiepileptic drug was not illustrated. | 12 weeks |
| Dimal et al. (2021) [ | 24, male | HCHB | Cerebral toxoplasmosis, cerebral tuberculosis | Right subthalamic nucleus, cerebral peduncle | Trimethoprim/ sulfamethoxazole, anti tuberculosis (isoniazid, rifampicin, ethambutol, pyrazinamide), risperidone | 9 months |
| Our case | 36, male | HCHB | Cerebral toxoplasmosis | Right thalamus, right centrum semiovale, right cerebral peduncle | Clindamycin, pyrimethamine, folinic acid, tetrabenazine, clonazepam | 1 month |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurological and metabolic disorders · Infectious Encephalopathies and Encephalitis · Autoimmune Neurological Disorders and Treatments
Introduction
Toxoplasma gondii encephalitis is a severe opportunistic cerebral infection caused by reactivation of the intracellular protozoan Toxoplasma gondii. In immunocompromised individuals, latent tissue cysts acquired from consuming undercooked meat, unwashed vegetables, or contact with cat feces can reactivate, leading to necrotising encephalitis. This opportunistic infection occurs most commonly among people living with HIV (PLHIV), with the greatest risk occurring in those with a CD4 count of <50 cells/µL [1]. The classic manifestations of cerebral toxoplasmosis are those of a focal encephalitis, including headache, fever, confusion, seizures, focal motor weakness, and potentially coma. However, movement disorders, while less common, represent a significant and diagnostically crucial clinical presentation. Reported rates of movement disorders in HIV-associated cerebral toxoplasmosis vary from 2% in contemporary antiretroviral therapy (ART)-treated cohorts to as high as 40% in pre-ART populations [2-5]. Hemichorea-hemiballismus (HCHB) in PLHIV is a rare presentation compared to other movement disorders [3,4]. Involvement of subcortical brain structures, particularly the basal ganglia, is often related to opportunistic infections like toxoplasmosis, especially in patients with advanced HIV disease [2]. Despite advancements in ART and the decline in severe opportunistic infections, this case contributes to the essential educational repository for clinicians in recognising HCHB as a neurological manifestation in individuals with AIDS. It also reinforces the need for early initiation of appropriate therapy to improve outcomes.
Case presentation
A 36-year-old man with a known history of HIV and hepatitis B co-infection presented to the emergency department with an acute neurological syndrome in December 2023. He had been lost to follow-up for two years after initially starting ART. He presented with a two-day history of involuntary movements affecting his left arm and leg. The symptom was accompanied by slurred speech and involuntary grimacing. He noticed the hyperkinetic symptoms completely resolved during sleep. There was no history of diabetes, substance use or family history of movement disorders. On examination, he was alert and oriented. Neurological examination revealed left-sided hemichorea-hemiballismus (HCHB), with left upper limb hypertonia and hyperreflexia but preserved muscle power of 5/5. An urgent ophthalmology review ruled out ocular toxoplasmosis.
Initial blood investigations (Table 1) showed mild anemia with hemoglobin of 11.2 g/dL and white cell count of 4.5 x109/L. Subsequent CD4 count of 4 cells/µL and an HIV viral load of 398,000 copies/mL, confirming AIDS. A presumptive diagnosis of Toxoplasma gondii encephalitis was made following Magnetic Resonance Imaging (MRI) of the brain (Figures 1, 2) revealed T2W/FLAIR hyperintense signals in the right thalamus (with T1 hyperintense rim enhancement), extending into the right cerebral peduncle, and the right centrum semiovale with perilesional edema. In addition, serology was positive for Toxoplasma gondii IgG. A lumbar puncture was performed to rule out other mimics like meningitis or CNS lymphoma. Opening pressure was not raised, mildly elevated protein (0.59g/L), and a normal glucose ratio. CSF cytology showed no pleocytosis and was negative for malignancy on cytology. Crucially, CSF PCR tests for tuberculosis, viruses, and bacteria were negative. However, CSF testing for Toxoplasma PCR and EBV PCR was not available in our centre.
MRI of the brain T2 FLAIR showed hyperintensity at the right thalamus with perilesional edema (thin red arrow).T2-FLAIR: T2-weighted-Fluid-Attenuated Inversion Recovery
MRI of the brain with T2 FLAIR showed hyperintensity at the right cerebral peduncle (thick red arrow) T2-FLAIR: T2-weighted-Fluid-Attenuated Inversion Recovery
Due to the unavailability of sulfadiazine, anti-toxoplasma therapy was initiated with trimethoprim-sulfamethoxazole (TMP-SMX) at a dose of 1920 mg twice daily (approximately equivalent to 10 mg/kg/day of TMP). For the movement disorder, tetrabenazine (12.5 mg twice daily) and clonazepam (1 mg twice daily) were prescribed. During the second week of anti-toxoplasma therapy, TMP-SMX was switched to pyrimethamine (75 mg daily) and clindamycin (600 mg every 6 hours) due to kidney impairment and transaminitis. On day 11 of anti-toxoplasma therapy, the patient was started on ART consisting of tenofovir disoproxil fumarate (300 mg daily), emtricitabine (200 mg daily), and dolutegravir (50 mg daily). The patient demonstrated remarkable clinical recovery prior to discharge. After one month of therapy, his involuntary movements had resolved completely, and he had regained the ability to walk independently. Following completion of the 8-week induction phase for toxoplasma therapy, maintenance therapy was initiated with clindamycin (600 mg every 8 hours) and pyrimethamine (75 mg daily).
Discussion
Toxoplasma gondii is an intracellular protozoan that is typically acquired via the ingestion of tissue cysts from either uncooked meat or soil contaminated by cat faeces. Infection is often asymptomatic in immunocompetent hosts. The risk of cerebral toxoplasmosis is higher in individuals who are seropositive for the parasite than in those who are seronegative. The reactivation of latent toxoplasmosis depends on the degree of host immunosuppression. The clinical presentation varies depending on the location of brain involvement [2]. Common manifestations of Toxoplasma gondii encephalitis include headache, cranial nerve palsy, and altered sensorium, fever, focal motor deficits and seizures.
According to a systematic review on movement disorders in PLHIV, opportunistic cerebral toxoplasmosis is the most common cause of hemichorea-hemiballismus in patients with AIDS, accounting for up to 60% of hemichorea cases [6]. Cerebral toxoplasmosis frequently affects the juxta-cortical regions and basal ganglia. This specific neuroanatomical localisation is why movement disorders are a more prominent feature in toxoplasmosis than in other opportunistic infections [7]. On imaging, it typically presents as ring-enhancing lesions on contrast-enhanced CT or MRI of the brain. It can be challenging to distinguish from other conditions like cerebral tuberculoma or lymphoma radiologically [8].
The definitive diagnosis of cerebral toxoplasmosis requires a brain tissue biopsy to identify the trophozoite. However, this invasive procedure carries a high risk of bleeding and neurological complications and is therefore rarely performed. CSF Toxoplasma PCR is another diagnostic tool with good sensitivity of 83% and specificity up to 95%, but lumbar puncture is limited due to cerebral oedema, and the test is not widely available in resource-limited settings [9]. In this case, a presumptive diagnosis of Toxoplasma gondii encephalitis was made based on the clinical history of advanced HIV, the presence of a basal ganglia lesion on brain imaging, and supportive positive Toxoplasma serology, even though the classic ring-enhancing lesion was not seen.
The recommended therapy for Toxoplasma gondii encephalitis is a combination of pyrimethamine, sulfadiazine, and leucovorin [1]. However, due to the unavailability of sulfadiazine in our country, initial therapy was commenced with trimethoprim/sulfamethoxazole (TMP-SMX), which serves as an effective alternative. The regimen was then switched to pyrimethamine and clindamycin, alongside leucovorin, due to TMP-SMX-related kidney and liver impairment. Tetrabenazine and clonazepam were initiated to manage the disabling HCHB symptomatically. Tetrabenazine works by depleting monoamines in the central nervous system, helping to control hyperkinetic movements, while clonazepam acts as a muscle relaxant. Our patient demonstrated significant clinical improvement within a few weeks of therapy. This positive response further supported the presumptive diagnosis of cerebral toxoplasmosis. A good clinical outcome can be expected with an early diagnosis and prompt initiation of anti-toxoplasma therapy.
Table 2 illustrates a summary of HCHB cases associated with cerebral toxoplasmosis and their clinical outcomes. The most commonly affected sites were the thalamus and basal ganglia. Some cases involved co-infections, particularly with tuberculosis or syphilis, which required dual therapy. The time to complete symptom resolution was highly variable, ranging from two weeks to nine months. The presence of a dual pathology often contributes to a longer recovery period than a mono-infection. In our case, the patient's symptoms resolved with treatment, which indicates that HCHB due to an active infection can be reversible [10]. This contrasts with movement disorders due to other causes, such as HIV-associated neurodegeneration or Huntington's disease (HD), which may have progressive or persistent symptoms. Therefore, a lack of clinical response to toxoplasma treatment within two weeks of therapy should raise suspicion for alternative or additional diagnoses, such as persistent gliosis [11] or an undiagnosed neurodegenerative condition like Huntington's disease.
Conclusions
HCHB is one of the rare but reversible symptoms in cerebral toxoplasmosis, owing to the predilection of the infection for the basal ganglia and thalamic nuclei. The diagnosis is frequently presumptive, relying on neurological presentation, imaging, and positive toxoplasma serology. Therefore, early initiation of therapy is crucial to optimise patient outcomes. The failure of symptoms to improve with anti-toxoplasma therapy may warrant further investigation, including stereotactic brain biopsy or CSF toxoplasma PCR, to establish a definitive diagnosis. This case also highlights the importance of ART adherence to maintain virological suppression and potentially reduce the development of opportunistic infections. Medications to control the movement disorders may be beneficial as symptomatic treatment, particularly in the acute phase of the disease. The recovery time varies from weeks to months, depending on the severity of the disease and the affected sites.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Guidelines for prevention and treatment of opportunistic infections in HIV-infected adults and adolescents: recommendations from CDC, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America MMWR Recomm Rep Kaplan JE Benson C Holmes KK Brooks JT Pau A Masur H 120758 2009 https://pubmed.ncbi.nlm.nih.gov/19357635/19357635 · pubmed ↗
- 2HIV-related movement disorders: Epidemiology, pathogenesis and management CNS Drugs Cardoso F 66366816(10)2002 https://pubmed.ncbi.nlm.nih.gov/19357635/1226986010.2165/00023210-200216100-00002 · doi ↗ · pubmed ↗
- 3Hemichorea-hemiballismus as a presentation of cerebritis from intracranial toxoplasmosis and tuberculosis Tremor Other Hyperkinet Mov (N Y) Dimal NPM Santos NJC Reyes NGD Astejada MN Jamora RDG 66366811:22021;11:2https://pubmed.ncbi.nlm.nih.gov/19357635/10.5334/tohm.576PMC 782497733552670 · doi ↗ · pubmed ↗
- 4Hemichorea-hemiballismus as an initial manifestation in a Moroccan patient with acquired immunodeficiency syndrome and toxoplasma infection: A case report and review of the literature Pan Afr Med J Rabhi S Amrani K Maaroufi M 910201110.4314/pamj.v 10i 0.72216 PMC 328293422187591 · doi ↗ · pubmed ↗
- 5Movement disorders and AIDS: A review Parkinsonism Relat Disord Tse W Cersosimo MG Gracies JM Morgello S Olanow CW Koller W 3233341020041526187410.1016/j.parkreldis.2004.03.001 · doi ↗ · pubmed ↗
- 6A review of movement disorders in persons living with HIV Parkinsonism Relat Disord Amod F Holla VV Ojha R Pandey S Yadav R Pal PK 10577411420233753262110.1016/j.parkreldis.2023.105774 · doi ↗ · pubmed ↗
- 7Movement disorders in 28 HIV-infected patients Arq Neuropsiquiatr Mattos JP Rosso AL Correa RB Novis SA 525530602002 https://pubmed.ncbi.nlm.nih.gov/12244384/12244384 · pubmed ↗
- 8HIV-associated opportunistic CNS infections: Pathophysiology, diagnosis and treatment Nat Rev Neurol Bowen LN Smith B Reich D Quezado M Nath A 6626741220162778624610.1038/nrneurol.2016.149 · doi ↗ · pubmed ↗