Acute lymphoblastic B‐cell leukemia or CAR‐T cell related skin changes – a relevant diagnostic challenge
Farzan Solimani, Amrei Dilling, Konrad Heisterkamp, Frederik Damm, Olaf Penack, Christian Oberender, Philipp Le‐Coutre, Martina Rudelius, Kamran Ghoreschi, Alexander Nast

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1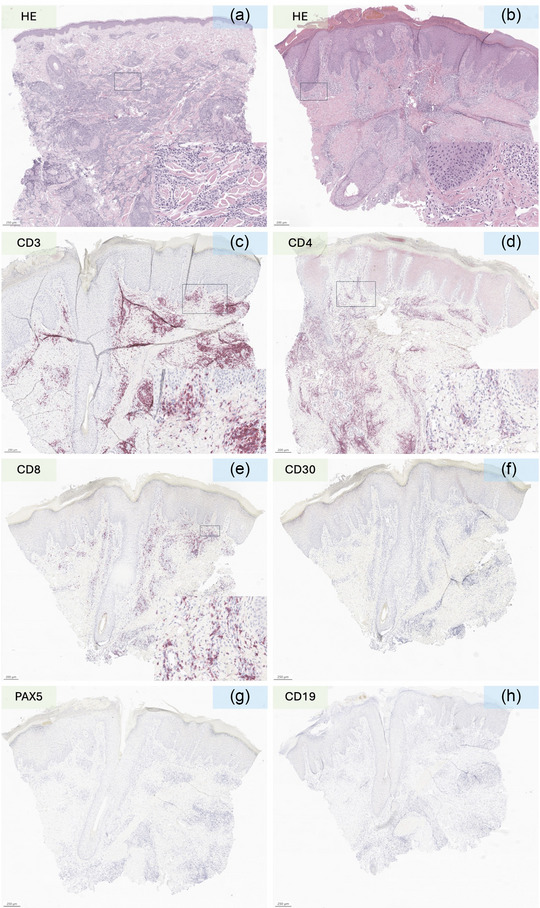 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCAR-T cell therapy research · Cutaneous lymphoproliferative disorders research · Virus-based gene therapy research
Dear Editors,
Chimeric antigen receptor (CAR) therapy is bringing revolutionary therapeutic concepts into clinical practice and enabling physicians to deplete specific cells.1 CAR‐T cells are based on genetically engineered T cells that selectively target specific antigens.1 The increasing numbers of patients receiving CAR‐T therapy is also leading clinicians to encounter rare adverse events more frequently. Cutaneous adverse events of CAR‐T therapy are poorly understood and rarely described and can challenge clinicians to differentiate between recurrence of disease and secondary cutaneous toxicity. A recent case from our department illustrates the clinical and diagnostic challenges of CAR‐T cell induced cutaneous adverse events.
A 50‐year‐old man was diagnosed with a BCR‐ABL and KMT2A negative acute lymphoblastic B‐cell leukemia (B‐ALL) and initially treated with a chemotherapeutic induction regimen (dexamethasone, cyclophosphamide, daunorubicin, peg‐asparaginase, cytarabine) and rituximab. This triggered an antithrombin III deficiency, and, in accordance with the patient's wishes, the treatment was terminated. Eight months later the patient presented to our outpatient dermatological clinic due to the occurrence of infiltrated plaques on the occipital side of head. A histological examination showed nodular partly diffuse blastic infiltrate with CD19^+^, PAX5^+^, CD3^‐^ profile and a high (80%) Ki67 proliferation index (Figure 1a). A recurrence of B‐ALL was diagnosed. Eighteen months later salvage therapy with blinatumomab (a bispecific monoclonal antibody (mAB) T‐cell engager that recognizes and links CD3 and CD19) was started but was dismissed shortly thereafter due to generalized serositis. After a thorough explanation of the available options, the patient declined an allogeneic transplantation and opted for anti‐CD19 CAR‐T treatment, which was started 4 months later. After bridging therapy with inotuzumab ozogamicin (a humanized mAb against the B‐cell marker CD22 linked to a cytotoxic agent) and conditioning (fludarabine and cyclophosphamide) the patient received 1 x 10^6^‐CAR‐T cells/kg (brexucabtagene autoleucel, an autologous CD19 directed CAR). A grade II cytokine release syndrome (CRS) was promptly managed with tocilizumab (an anti‐IL‐6 receptor mAb). Eight months after CAR‐T infusion the patient presented in our department again due to the onset of painless non‐pruriginous macules and slightly infiltrated plaques and nodules on the occipital side of the head, abdominal region and knee (Figure 2). Additionally, the patient reported to have morning stiffness, joint pain and myalgia. There was no evidence of any further organ‐related toxicity. The medical history also ruled out the possibility of a contact allergic reaction, viral exanthema or vaccine‐related reaction. Apart from a slight decrease in circulating neutrophils and an increase in monocytes, the differential blood count showed no pathological changes in the circulating CD4/CD8 T and natural killer (NK) cells. We suspected a recurrence of B‐ALL and performed histological examination of skin biopsy from the abdominal regional and occipital region. Histology revealed a dense lymphocytic and eosinophilic infiltration with perivascular accentuation. The lymphocytic infiltration was made up almost exclusively by a small mixed CD4/CD8 CD30^–^ T cells (Figure 1b–f), whereas B cell‐lineage specific markers (CD20, CD19, Pax5) showed only a few positive cells, thus excluding the presence of a B‐cell malignancy (Figure 1g–h). Ki67 was also not significantly elevated and terminal deoxynucleotidyl transferase (TdT, a marker for lymphoblastic lymphomas and leukemias) was negative (Figure 2). A clonality assessment of the immunoglobulin heavy chain (IgH, framework regions FR1‐4) and of the T‐cell receptor (TCR)γ (Vγ/J, Vγ/Jp) showed a polyclonal IgH repertoire and absence of TCR‐clonality. These results pointed against the presence of B‐ALL or other haemato‐oncological diseases and we made a diagnosis of CAR‐T cell induced T‐cell pseudo lymphomatous skin reaction. The lesions improved rapidly in the first 3 months, after which they showed some symptom‐free residual inflammation that was resistant to treatment. Twelve months after CAR‐T cell treatment, the patient is still in remission at follow‐up examinations with regard to B‐ALL and still shows slight residual erythematous lesions.
While CRS and Immune effector cell‐associated neurotoxicity syndrome (ICANS) are well described adverse events, cutaneous manifestations need to be elucidated and poses a clinical challenge, especially since it might mimic leukemia cutis. Reports described so far different cutaneous manifestation such as maculopapular eruptions, erythematous rashes, purpura, petechiae, and blistering lesions.2, 3 A recent study on CAR‐T clinical trials showed that mild‐to‐moderate skin reactions occur in up to 35% of enrolled patients.2 Lack of dermatological training could conceal higher rates. For physicians, it is crucial to thoroughly exclude a recurrence of disease. We performed immunohistochemistry and clonality assessment to rule out leukemia cutis. Other groups took different approaches. One group applied flow cytometry of blister fluids and skin‐lesional T cells from a patient with bullous eruption, which showed presence of CD3 mixed CAR‐T^+^/CAR‐T^–^ cells.4 In a study involving CD30 CAR‐T cell therapy in Hodgkin lymphoma skin reactions were analyzed by histology and quantitative polymerase chain reaction showing expression of the CD30 CAR transgene.5 The underlying immunopathomechanism for CAR‐T‐induced skin reactions still needs to be clarified. In our patient, the skin reaction interestingly occurred in the occipital region, where the patient originally developed leukemia cutis. This might indicate a possible initial reaction to malignant resident B‐cells as primum movens for skin infiltration. Concordantly to this concept, Hagen et al. recently described a new form of late‐onset CAR‐T‐related organ toxicity (local immune effector cell‐associated toxicity syndrome (LICATS)) in patients with autoimmune diseases who developed inflammatory reactions in the affected organs due to CAR‐T‐mediated B‐cell killing. The reported skin lesions are very similar to those observed in our patient, which also occurred as a result of B‐cell killing in the skin6.
CONFLICT OF INTEREST STATEMENT
None.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Uslu U , Castelli S , June CH . CAR T cell combination therapies to treat cancer. Cancer Cell. 2024;42(8):1319‐1325.39059390 10.1016/j.ccell.2024.07.002 · doi ↗ · pubmed ↗
- 2Nusbaum KB , Dulmage B , Choi JN , et al. Cutaneous manifestations of chimeric antigen receptor T‐cell therapy: An introduction for dermatologists. J Am Acad Dermatol. 2022;87(3):597‐604.34293386 10.1016/j.jaad.2021.07.017 · doi ↗ · pubmed ↗
- 3Rubin CB , Elenitsas R , Taylor L , et al. Evaluating the skin in patients undergoing chimeric antigen receptor modified T‐cell therapy. J Am Acad Dermatol. 2016 Nov;75(5):1054‐1057.27745631 10.1016/j.jaad.2016.06.062 · doi ↗ · pubmed ↗
- 4Hu Y , Zheng W , Qiao J , et al. Bullous and Exanthematous Lesions Associated With Chimeric Antigen Receptor T‐Cell Therapy in a Patient With Diffuse Large B‐Cell Lymphoma. JAMA Dermatol. 2020 S;156(9):1026‐1028.32432646 10.1001/jamadermatol.2020.0636 · doi ↗ · pubmed ↗
- 5Ramos CA , Grover NS , Beaven AW , Lulla PD , et al., Anti‐CD 30 CAR‐T Cell Therapy in Relapsed and Refractory Hodgkin Lymphoma. J Clin Oncol. 2020;38(32):3794‐3804.32701411 10.1200/JCO.20.01342 PMC 7655020 · doi ↗ · pubmed ↗
- 6Hagen M , Müller F , Wirsching A , Kharboutli S , et al., Local immune effector cell‐associated toxicity syndrome in CAR T‐cell treated patients with autoimmune disease: an observational study. Lancet Rheumatol. 2025;7(6):e 424‐e 433.40318690 10.1016/S 2665-9913(25)00091-8 · doi ↗ · pubmed ↗