Surgical Management of Pleomorphic Lung Carcinoma With Left Atrial Invasion: Two Cases Including One With Cerebral Artery Metastasis
Eitetsu Koh, Yasuo Sekine, Hiroyuki Saitou, Kenzo Hiroshima

TL;DR
Two rare cases of aggressive lung cancer invading the heart and spreading to the brain are reported, showing the challenges and outcomes of surgical treatment.
Contribution
Demonstrates the feasibility of CPB-assisted surgery for rare PLC with left atrial invasion and highlights unusual cerebral metastasis.
Findings
CPB-assisted resection is technically feasible for PLC with left atrial invasion.
PLC can metastasize to cerebral arteries, causing ruptured aneurysms and subarachnoid hemorrhage.
Multidisciplinary planning is essential for managing PLC with atypical vascular metastasis.
Abstract
Pleomorphic carcinoma is a rare, aggressive subtype of non‐small cell lung cancer (NSCLC). Invasion into the left atrium and dissemination to cerebral arteries are exceptionally uncommon, and the role of cardiopulmonary bypass (CPB)–assisted resection remains debated. We report two surgically treated cases with left atrial invasion. Case 1: A 57‐year‐old man underwent left lower lobectomy with partial atrial resection under CPB. One month later, he developed subarachnoid hemorrhage caused by rupture of a cerebral aneurysm secondary to metastasis; histology of the aneurysmal wall confirmed carcinoma. He remains recurrence‐free at 21 months. Case 2: A 62‐year‐old woman underwent extended left upper lobectomy with partial atrial resection under CPB. Although adrenal metastasis was suspected radiologically, pathological confirmation was lacking preoperatively; surgery was pursued because of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
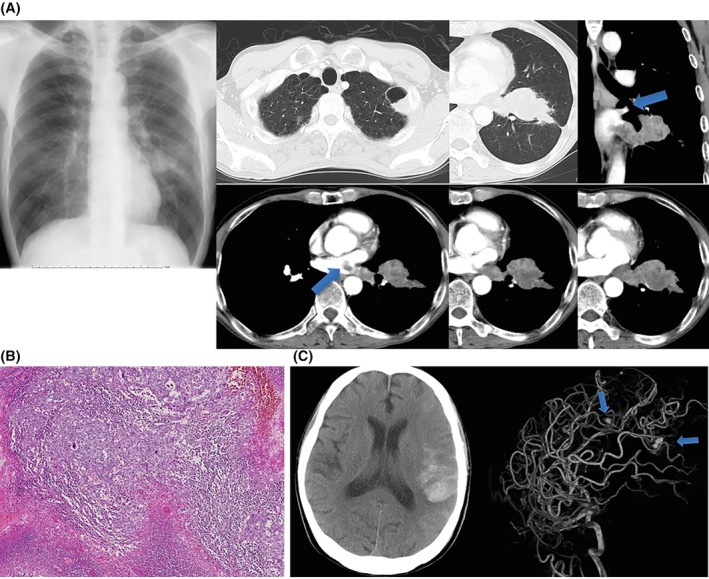 FIGURE 1
FIGURE 1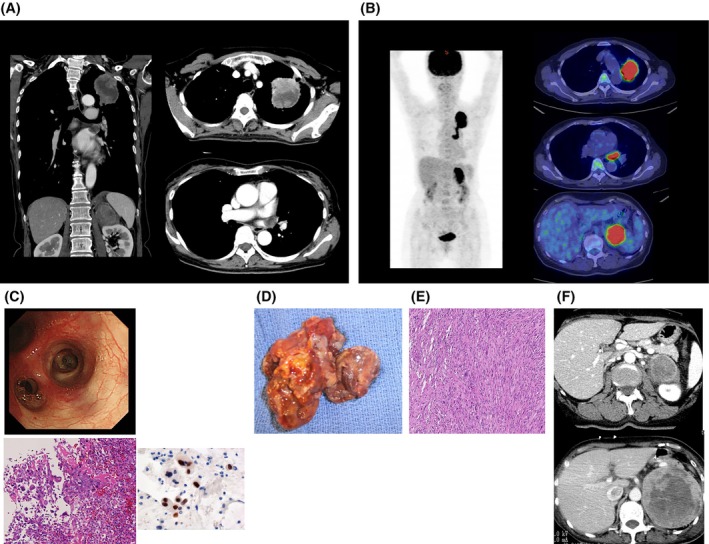 FIGURE 2
FIGURE 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMetastasis and carcinoma case studies · Cardiac tumors and thrombi · Lung Cancer Diagnosis and Treatment
Introduction
1
Pleomorphic carcinoma accounts for < 1% of NSCLC and is characterized by spindle and/or giant cells with high metastatic potential and chemoresistance. When tumors extend into the left atrium, CPB‐assisted resection is occasionally attempted, but long‐term oncologic benefit is uncertain. Metastatic involvement of cerebral arterial walls leading to aneurysmal rupture is exceedingly rare. We present two pleomorphic carcinoma cases with atrial invasion—one complicated by histology‐proven metastatic cerebral aneurysm—to discuss surgical feasibility, selection, and surveillance.
Case Presentations
2
Case 1
2.1
A 57‐year‐old man presented with hemoptysis and frequent atrial arrhythmias. CT showed a left lower‐lobe mass invading the left atrium. Endobronchial ultrasound–guided nodal assessment showed no mediastinal metastasis. Due to urgent symptoms (recurrent hemoptysis/arrhythmias), surgery proceeded without cranial MRI. Left lower lobectomy with partial atrial resection under CPB was performed. Pathology: pleomorphic carcinoma (pT4N0M0, pl0, pm2, and stage IIIA). One month later, subarachnoid hemorrhage occurred; angiography revealed multiple aneurysms. Aneurysm clipping confirmed metastatic carcinoma in the aneurysmal wall. At 21 months postoperatively, he remains recurrence‐free (Figure 1A–C).
Case 1. (A) Preoperative chest radiograph/CT showing a left lower‐lobe mass invading the left atrium (arrows); EBUS‐TBNA supported surgery by excluding mediastinal nodal disease. Clinical stage cT4N0/1 M0, stage IIIA. (B) Histology (H&E): Pleomorphic carcinoma with marked atypia and spindle cells; pT4N0M0, pl0, pm2. (C) Postoperative CT/MRA revealing multiple cerebral aneurysms (arrows); enlargement despite antibiotics prompted clipping. Aneurysmal wall contained metastatic carcinoma.
Case 2
2.2
A 62‐year‐old woman had a 6‐cm left upper‐lobe mass extending into the left superior pulmonary vein and left atrium. PET‐CT suggested adrenal uptake; preoperative pathology confirmed pleomorphic carcinoma while adrenal metastasis was unproven histologically. Extended left upper lobectomy with partial atrial resection under CPB was performed. She developed postoperative cerebral infarction and rapid adrenal progression despite carboplatin–paclitaxel chemotherapy, and died 4 months postoperatively (Figure 2A–F).
Case 2. (A) Preoperative CT: 6‐cm left upper‐lobe mass with pulmonary vein/atrial invasion. (B) PET‐CT: High uptake in the lung tumor and left adrenal gland (SUVmax 24.5 → 27.5). (C) Bronchoscopy/biopsy: Poorly differentiated NSCLC with pleomorphism; IHC TTF‐1+, p40−, Napsin A−, p63−; EGFR mutation negative. (D) Intraoperative gross: ~4.5‐cm mass protruding into the atrial cavity. (E) Histology (H&E): Pleomorphic carcinoma; pT4N0. (F) Abdominal CT: Adrenal lesion grew from ~4 cm preop to > 10 cm at 3 months.
Discussion
3
Our experience underscores dual challenges: the technical demands of atrial resection and the intrinsically aggressive biology of pleomorphic carcinoma. Small series have reported acceptable perioperative outcomes with atrial resection under CPB in selected T4 NSCLC, but durable control is limited in histologies with early dissemination. In Case 1, metastatic infiltration of a cerebral arterial wall caused aneurysmal rupture—an extremely rare pattern previously described only sporadically. From a biological perspective, pleomorphic carcinoma frequently shows epithelial–mesenchymal transition features, aligning with early hematogenous spread and atypical vascular tropism. Clinically, we recommend comprehensive preoperative staging (including brain imaging when feasible), explicit documentation of nodal assessment, early involvement of cardiac surgery, and vigilant neuro‐oncologic surveillance. In suspected stage IV disease, the threshold for induction or systemic therapy should be low; surgery must rest on multidisciplinary consensus and patient‐centered goals [1, 2, 3, 4].
Conclusions
4
CPB‐assisted resection can be feasible for left‐atrial invasion; however, pleomorphic histology often dictates outcome. Multimodal strategies and close surveillance are essential, and unusual vascular metastases should be anticipated.
Author Contributions
Conceptualization: Eitetsu Koh, Yasuo Sekine. Methodology: Eitetsu Koh, Hiroyuki Saito. Surgery/clinical management: Eitetsu Koh, Yasuo Sekine, Hiroyuki Saito. Pathology Investigation: Kenzo Hiroshima. Data curation: Eitetsu Koh. Writing – original draft: Eitetsu Koh. Writing – review and editing: All authors. Supervision: Yasuo Sekine.
Funding
The authors have nothing to report.
Ethics Statement
This retrospective case report complied with institutional and national ethical standards. Institutional review board approval was waived.
Consent
Written informed consent for participation and publication (clinical details and images) was obtained from both patients.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M. Chida , M. Minowa , S. Miyoshi , A. Hattori , and M. Sato , “Surgical Outcomes of Lung Cancer Involving the Left Atrium,” European Journal of Cardio‐Thoracic Surgery 30, no. 2 (2006): 280–284.
- 2Y. Yu , J. Zhang , M. Bao , et al., “Surgical Treatment for Non‐Small Cell Lung Cancer With Left Atrial Invasion,” Journal of Cardiothoracic Surgery 9 (2014): 6.24393470
- 3N. F. Fishback , W. D. Travis , C. A. Moran , D. G. Guinee, Jr. , W. F. Mc Carthy , and M. N. Koss , “Pleomorphic (Spindle/Giant Cell) Carcinoma of the Lung: Clinicopathologic Correlation of 78 Cases,” American Journal of Surgical Pathology 18, no. 6 (1994): 582–593.
- 4K. Sato , Y. Yoshimoto , N. Sadamasa , O. Narumi , H. Kajiwara , and J. Hamada , “Pulmonary Carcinoma Metastasizing to the Cerebral Arterial Wall Causing Subarachnoid Hemorrhage,” Surgical Neurology International 7 (2016): 28.27114852