Expanding the boundaries of PTE: successful integration with multiple major cardiac procedures
Emily Hay-Arthur, Elizabeth J Bashian, Sarah Y Park, Jordan R H Hoffman, Michael T Cain

TL;DR
This paper presents a successful case of combining PTE with multiple major cardiac procedures, showing it can be done safely with proper planning.
Contribution
The paper demonstrates the first successful integration of PTE with multiple major cardiac surgeries in a single operation.
Findings
The patient recovered uneventfully after the combined procedures.
There was marked functional and hemodynamic improvement at 6 months.
The case highlights the importance of multidisciplinary preoperative planning.
Abstract
Pulmonary thromboendarterectomy (PTE) is the only curative treatment for chronic thromboembolic pulmonary hypertension. While combining PTE with a single cardiac procedure is well established, evidence for performing it with multiple major procedures is limited. We report a successful bilateral PTE with coronary artery bypass grafting, ascending aortic and hemiarch repair, patent foramen ovale closure, and left atrial appendage ligation. The patient recovered uneventfully, with marked functional and hemodynamic improvement at 6 months. This case demonstrates the safety and feasibility of complex cardiac surgery with PTE, underscoring the value of thorough, multidisciplinary preoperative planning.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
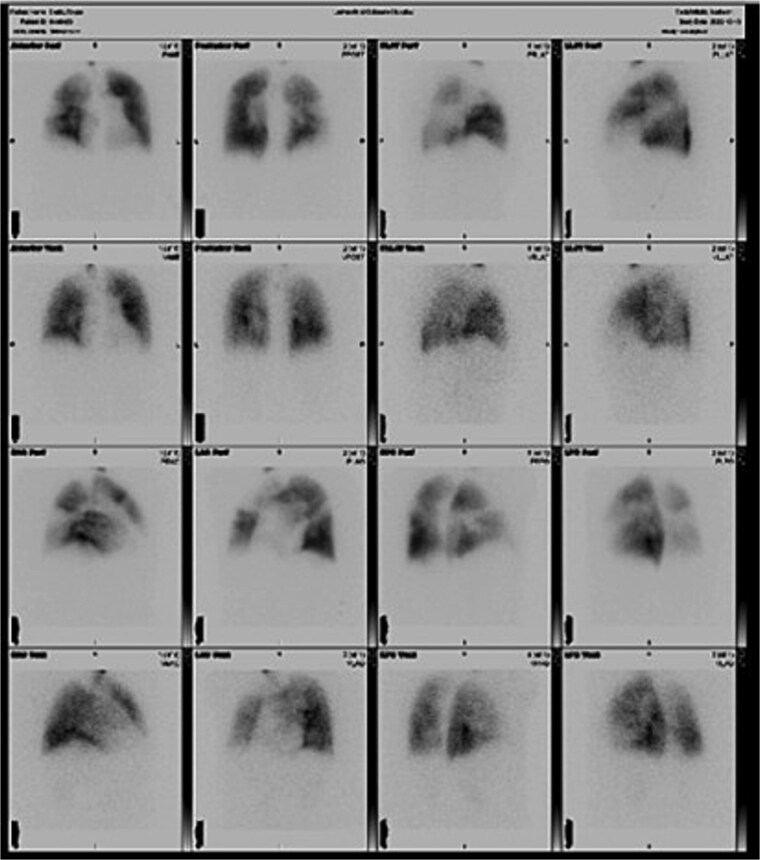 Figure 1
Figure 1 Figure 2
Figure 2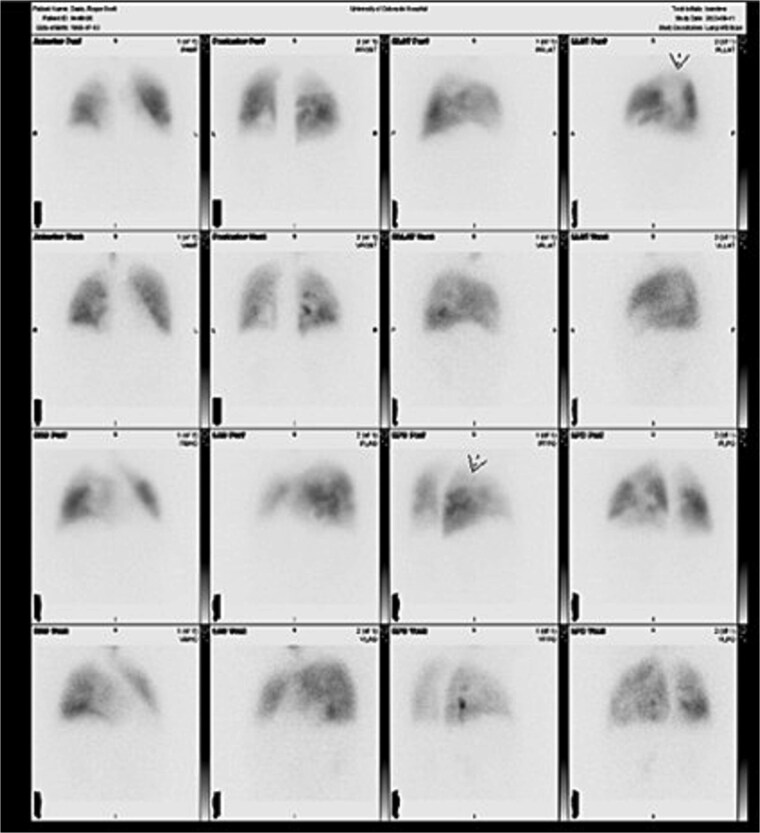 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPulmonary Hypertension Research and Treatments · Cardiac Valve Diseases and Treatments · Venous Thromboembolism Diagnosis and Management
Introduction
Chronic thromboembolic pulmonary hypertension (CTEPH) is an obstructive, fibrotic transformation of the pulmonary vasculature occurring in about 4% of patients after pulmonary embolism. It is defined as pulmonary artery pressure >20 mmHg, pulmonary vascular resistance >3 Woods units, and pulmonary capillary wedge pressure <15 mmHg. Untreated, CTEPH causes pulmonary vascular remodeling and the chronically elevated vascular pulmonary vascular resistance predisposes patients to right heart failure, and death [1, 2].
Pulmonary thromboendarterectomy (PTE), the only curative treatment for CTEPH, offering significant survival benefit [3, 4]. Previous reports show PTE can be performed with single additional procedures such as coronary artery bypass grafting (CABG) or valve interventions and literature supports combining multiple cardiac operations [3, 5, 6]. However, no prior reports describe bilateral PTE along with several major cardiac procedures in a single index operation. We describe a patient presenting with CTEPH also in need of aortic valve replacement, CABG, aortic aneurysm repair, patent foramen ovale (PFO) closure, and left atrial appendage ligation (LAAL).
Case report
Informed written consent was obtained. A 68-year-old male with history of CTEPH, chronic obstructive pulmonary disease, coronary artery disease, chronic osteomyelitis, Type II diabetes, and persistent atrial fibrillation presented with worsening dyspnea requiring home oxygen. Preoperative evaluation showed mean pulmonary artery pressure 42 mmHg, PCWP 11 mmHg, PVR 8.66 Wood units, and bilateral mismatches on ventilation–perfusion (V/Q) scan (Fig. 1). Coronary angiogram revealed multivessel disease. Echocardiogram showed severe eccentric aortic insufficiency, ascending aortic aneurysm, PFO, and enlarged right ventricle (RVSP 77 mmHg). Multidisciplinary review deemed the patient suitable for PTE with concomitant procedures.
Preoperative ventilation-perfusion (V/Q) scan demonstrating bilateral segmental and subsegmental perfusion defects consistent with chronic thromboembolic pulmonary hypertension.
Under general anesthesia, a pulmonary artery catheter and transesophageal echocardiography confirmed preoperative findings. CABG was performed with left internal mammary artery to the left anterior descending artery and saphenous vein graft to the right coronary artery. Bilateral pulmonary endarterectomy with right pulmonary artery patch angioplasty was completed. Disease was Jameson class I on the right and class II on the left (Fig. 2). The patient then underwent aortic valve replacement with an Edwards Inspiris tissue valve, ascending aorta repair, PFO closure, and LAAL. No intraoperative complications occurred. He was extubated on postoperative day 1. Echocardiogram showed a mildly enlarged right ventricle with normal pressures. Mean PA pressures were 24, 18, 24, and 15 mmHg on postoperative days 1–4. He was discharged on day 8 requiring 3 L oxygen at rest and 8 L with exertion. At 6 months, he required no supplemental oxygen and reported improved exercise tolerance. Follow-up V/Q scan showed markedly improved bilateral perfusion (Fig. 3).
Intraoperative specimen showing large clot burden removed during bilateral pulmonary thromboendartectomy, with both subacute and chronic organized thromboembolic material evident.
Six-month postoperative V/Q scan demonstrating interval improvement in bilateral pulmonary perfusion, with homogenous distribution of radiotracer and normalization of hilar and vascular markings.
Discussion
PTE remains the gold standard for CTEPH, offering long-term survival benefits not matched by medical therapy [1–3]. Preoperative workup includes echocardiogram, right heart catheterization with pulmonary angiography, V/Q scan, and CTA chest to confirm diagnosis and exclude alternative causes of pulmonary hypertension. Evaluation for concurrent cardiac disease is essential; coronary angiography is indicated in patients with coronary risk factors [7]. Risk models such as STS and EuroSCORE may underestimate complexity in combined PTE cases.
Previous reports support combining PTE with one additional cardiac procedure [5, 6]. Thistlewaite et al. reported similar mortality between isolated PTE and PTE with concomitant CABG, PFO closure, or valve surgery [5]. Erdem et al. likewise reported good outcomes with combined procedures, most often CABG [6].
Our case extends these findings, showing safe performance of bilateral PTE with CABG, aortic valve replacement, aortic aneurysm repair, PFO closure, and LAAL in a single operation. Success relied on meticulous preoperative planning to minimize ischemic and bypass times. The hemiarch was resected during the first circulatory arrest before addressing the pulmonary arteries, improving exposure. CABG was performed during cooling, and valve/aortic work during rewarming, reducing idle time. This strategy resulted in cross-clamp and bypass times only slightly longer than for PTE alone [8].
Combining multiple procedures avoids staged operations, reducing the risk of repeat sternotomy and ongoing exposure to untreated pulmonary hypertension. Published data suggest no increased risk when adding general cardiac procedures to an aortic case, and concomitant procedures may confer a survival benefit.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pengo V, Lensing AWA, Prins MH, et al. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism. N Engl J Med 2004;350:2257–64. 10.1056/NEJ Moa 03227415163775 · doi ↗ · pubmed ↗
- 2Riedel M, Stanek V, Widimsky J, et al. Longterm follow-up of patients with pulmonary thromboembolism: late prognosis and evolution of hemodynamic and respiratory data. Chest 1982;81:151–8. 10.1378/chest.81.2.1517056079 · doi ↗ · pubmed ↗
- 3Al Abri Q, Lu AJ, Ramchandani MK. Chronic thromboembolic pulmonary hypertension: a comprehensive review and multidisciplinary approach to surgical treatment. Methodist Debakey Cardiovasc J 17:e 18–28. 10.14797/IQTU 6714 PMC 833120634377353 · doi ↗ · pubmed ↗
- 4Madani MM, Wiedenroth CB, Jenkins DP, et al. Pulmonary thromboendarterectomy: the potentially curative treatment of choice for chronic thromboembolic pulmonary hypertension. Ann Thorac Surg 2024;119:756–67. 10.1016/j.athoracsur.2024.07.05239265713 · doi ↗ · pubmed ↗
- 5Thistlethwaite PA, Auger WR, Madani MM, et al. Pulmonary thromboendarterectomy combined with other cardiac operations: indications, surgical approach, and outcome. Ann Thorac Surg 2001;72:13–8. 10.1016/S 0003-4975(01)02686-811465167 · doi ↗ · pubmed ↗
- 6Erdem H, Korun O, Yanartaş M, et al. Outcomes of pulmonary endarterectomy operation concomitant with cardiac procedures. Thorac Cardiovasc Surg 2020;69:279–83. 10.1055/s-0040-171058032738809 · doi ↗ · pubmed ↗
- 7Pandey AK, Lee NS, Marsal J, et al. Evaluation of routine coronary angiography before pulmonary thromboendarterectomy. Ann Thorac Surg 2021;111:1703–9. 10.1016/j.athoracsur.2020.06.10732896544 · doi ↗ · pubmed ↗
- 8Thalji NM, Suri RM, Daly RC, et al. The prognostic impact of concomitant coronary artery bypass grafting during aortic valve surgery: implications for revascularization in the transcatheter era. J Thorac Cardiovasc Surg 2015;149:451–460.e 2. 10.1016/j.jtcvs.2014.08.07325308117 · doi ↗ · pubmed ↗