Real-world evidence indicates romosozumab use is associated with a greater reduction in osteoporotic fractures than PTH (1–34) analogs in women
Ko-Hsiu Lu, Shiow-Ing Wang, Shun-Fa Yang

TL;DR
A study found that romosozumab reduces osteoporotic fractures more effectively than PTH drugs in women and older adults.
Contribution
This study provides real-world evidence that romosozumab is more effective than PTH analogs in reducing fracture risk in specific patient subgroups.
Findings
Romosozumab users had a 28.9% lower fracture risk compared to PTH users (HR: 0.711).
Benefits were strongest in women, older adults, and those with prior fractures.
Romosozumab also reduced hypercalcemia risk compared to PTH drugs.
Abstract
To compare the effectiveness of romosozumab (ROMO) with parathyroid hormone (PTH) receptor agonists [teriparatide (TPTD)/abaloparatide (APTD)] in reducing fracture risk following osteoporosis treatment. A TriNetX cohort study assessed fracture and mortality risks using Kaplan–Meier analysis with hazard ratios (HRs) and 95% confidence intervals (CIs). After propensity score matching (n = 2,258 pairs), ROMO users had lower risks of osteoporotic fractures (HR: 0.711, 95% CI: 0.542–0.931) and hypercalcemia (HR = 0.707, 95% CI: 0.511–0.977) compared with PTH receptor agonists. Five subgroup analyses demonstrated a reduced fracture risk in the ROMO cohort among women (HR: 0.738), patients aged ≥ 65 years (HR: 0.652), individuals with a history of prior fractures (HR: 0.659), and those without chronic kidney disease (CKD) (HR: 0.731). Sensitivity analyses confirmed the robustness of the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
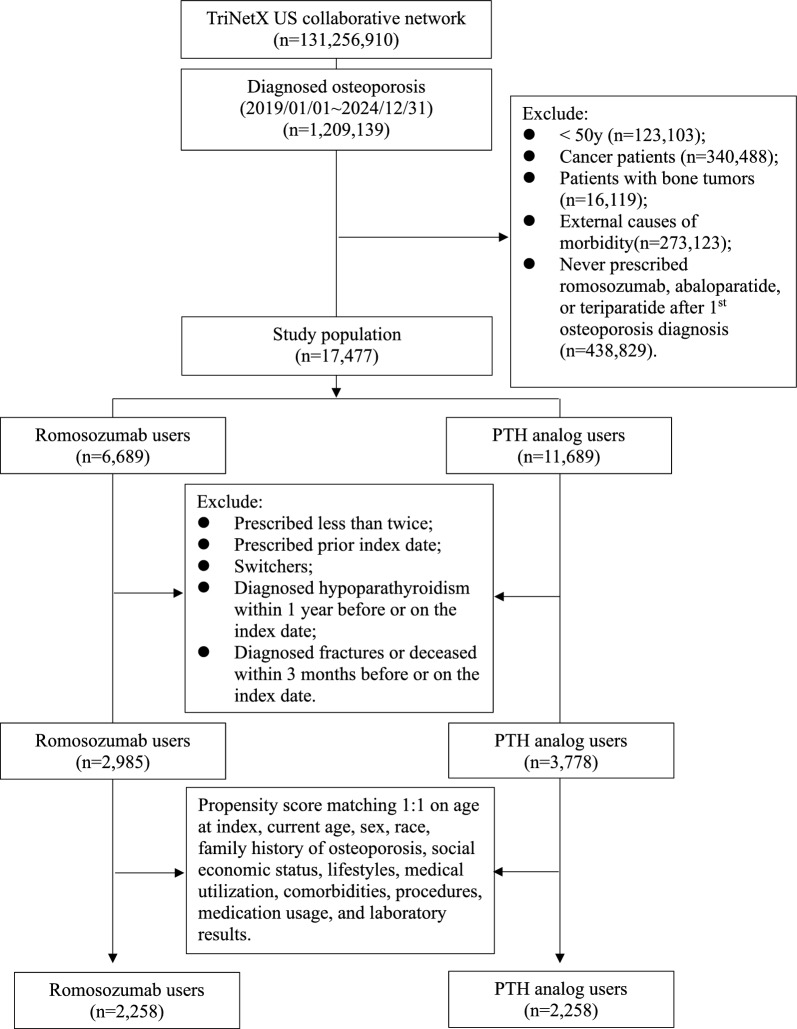 Figure 1
Figure 1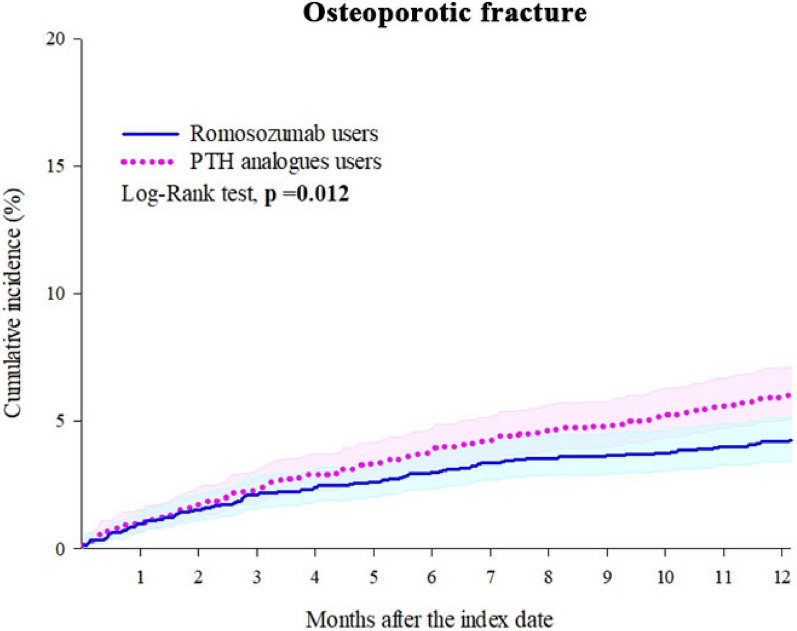 Figure 2
Figure 2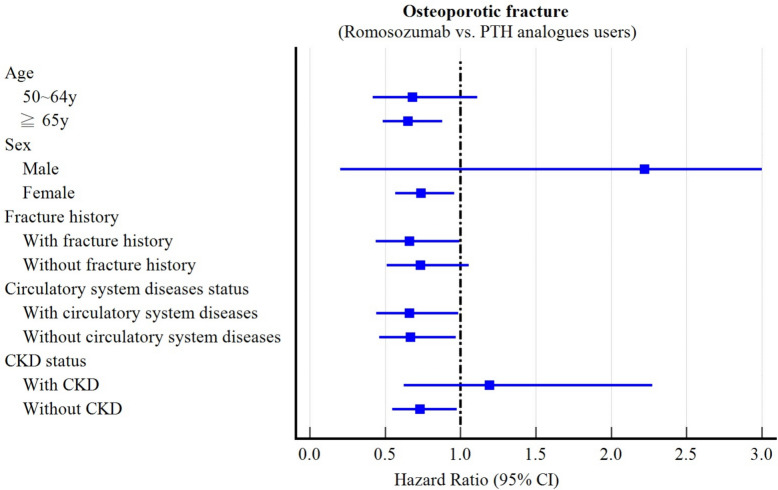 Figure 3
Figure 3- —https://doi.org/10.13039/501100004699Chung Shan Medical University Hospital
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone health and osteoporosis research · Parathyroid Disorders and Treatments · Bone health and treatments
Background
Severe osteoporosis with high fracture risk requires uninterrupted, long-term therapy [1]. Antiresorptive agents, including bisphosphonates (BPs), remain first-line due to proven efficacy, clinical experience, convenient dosing, and cost-effectiveness [1, 2]. However, osteoporotic fractures, particularly vertebral and hip fractures, substantially impact on morbidity, quality of life, mortality, and healthcare burdens, ultimately shortening life expectancy [3]. Patients with very high fracture risk, such as severe bone loss, prior vertebral fracture or hip fracture, antiresorptive-related adverse events, or poor bone health requiring surgery, may benefit from rapid gains in bone mass, microarchitecture, and biomechanics through osteoanabolic agents [4, 5]. These include teriparatide (TPTD, Forteo®), abaloparatide (APTD, Tymlos®), and romosozumab (ROMO, Evenity®), which provide greater bone mineral density (BMD) gains and fracture risk reduction than BPs [1, 6, 7].
TPTD, 1–34 parathyroid hormone (PTH) receptor 1 agonist, predominantly stimulates remodeling-based bone formation [1, 8]. Approved by the U.S. Food and Drug Administration (FDA) in 2002, TPTD was originally limited to a 24-month lifetime treatment duration [3, 9], but this restriction was removed in 2020 [10, 11]. Although it increases bone formation, coupled resorption constrains the net anabolic benefit [12]. In pivotal trials, 24 months of daily 20 µg TPTD reduced clinical fractures by 52%, vertebral fractures by 56%, and non-vertebral fractures by 34% compared with risedronate [13] with significant benefit seen as early as seven months [14]. Versus placebo, TPTD decreased vertebral fracture risk by 65% and non-vertebral fracture risk by 53% at 21 months [15].
APTD, a 1–34 PTH-related peptide analog and PTH receptor 1 agonist, was U.S. FDA-approved in 2017 with a 24-month lifetime limit. In an 18-month trial, daily 80 µg subcutaneous APTD increased BMD by 10.4% at the lumbar spine, 4.3% at the total hip, and 4.0% at the femoral neck versus placebo [16]. Both APTD and TPTD significantly reduced vertebral fracture risk by 86% and 80%, respectively. While APTD showed lower major osteoporotic fracture incidence than TPTD (1.5% vs. 3.1%), non-vertebral fracture reduction did not differ significantly (43% vs. 28%) from placebo.
ROMO, a humanized IgG2 monoclonal antibody against sclerostin, stimulates bone formation and inhibits resorption, primarily via modeling-based formation, producing rapid, substantial BMD gains [1, 8]. Approved by the U.S. FDA in 2019 for postmenopausal women, ROMO treatment is limited to 12 months [17]. Monthly 210 mg ROMO reduced clinical fractures by 27% versus alendronate, vertebral fractures by 48%, non-vertebral fractures by 19%, and hip fractures by 38%. Compared with placebo, ROMO reduced clinical fractures by 36% and vertebral fractures by 73%, with the strongest effect at the spine [18, 19]. After 12 months, ROMO increases femoral neck BMD by 4.8–5.9% versus placebo and 2.5–3.2% versus alendronate, total hip BMD by 4.8–6.8% versus placebo and 2.2–3.4% versus alendronate, and lumbar spine BMD by 11.4–13.3% versus placebo and 7.2–8.7% versus alendronate [8, 18, 19].
TPTD is often reserved for patients at very high fracture risk (e.g., ≥ 2 prevalent fractures) or prior BP exposure [4]. However, prior antiresorptive therapy may blunt TPTD’s anabolic response, particularly at the hip, sometimes causing early BMD decline in the first year [20, 21]. Similarly, early ROMO responses are attenuated by prior BPs or denosumab [21, 22], predictable by early changes in bone turnover markers [23, 24]. Head-to-head trials in treatment-naïve postmenopausal women with osteopenia show greater BMD and bone strength gains at the femoral neck, total hip, and lumbar spine after 12 months of ROMO versus TPTD, especially at the lumbar spine [21, 25, 26]. The STRUCTURE trial confirmed superior BMD improvements in women transitioning from BPs to ROMO versus TPTD [27].
Because on-treatment BMD gains strongly correlate with fracture risk reduction [28], attenuation after prior antiresorptive therapy may compromise both agents’ effectiveness. Given the lack of real-world data directly comparing fracture outcomes between ROMO and PTH receptor 1 agonists, we analyzed the TriNetX U.S. network in osteoporosis patients without recent fractures (within three months), evaluating osteoporotic, vertebral, non-vertebral, and hip fractures, all-cause mortality, and calcium abnormalities.
Materials and methods
Study design
We conducted a retrospective cohort study using the TriNetX U.S. collaborative network, which includes 72 healthcare organizations (HCOs) and over 100 million patients across the United States. This network captures both insured and uninsured patients from hospitals, as well as primary care and specialty services. Detailed information on TriNetX is available on its official website (https://trinetx.com/?mc_cid=7e2ecd5bc5&mc_eid=%5BUNIQID%5D). Data quality is ensured through standardized metrics assessing conformance, completeness, and plausibility. Using the TriNetX platform, we created matched comparison cohorts with a built-in propensity score matching (PSM) algorithm according to predefined inclusion and exclusion criteria [29, 30]. Analyses covered the period from January 1, 2019, to December 31, 2024.
Ethics statement
The TriNetX database contains only de-identified data. Protected health information, including exact age for patients over 90 years, was removed. De-identification has been validated by a qualified expert in accordance with the HIPAA Privacy Rule (§164.514(b)(1)), most recently in December 2020. Therefore, analyses using TriNetX are generally not considered “human subjects research” and are exempt from IRB review. This study was additionally approved by the Institutional Review Board of Chung Shan Medical University Hospital (approval no. CS2-23,208) and was reported in accordance with the RECORD (Reporting of Studies Conducted Using Observational Routinely Collected Health Data) guidelines.
Participants
Patients diagnosed with osteoporosis were identified on at least two separate occasions using the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) codes M80 and M81. Eligible patients were aged ≥ 50 years and received either ROMO (defined by the normalized name for clinical drugs, RxNorm 2,123,126), TPTD (RxNorm 32,915), or APTD (RxNorm 1,921,069) following their initial recorded diagnosis of osteoporosis (Fig. 1).Fig. 1. Flowchart of the selection process
The index date was defined as the first prescription date of ROMO, TPTD, or APTD during the study period. Exclusion criteria included: prevalent users who received prescriptions for ROMO, TPTD, or APTD before January 1, 2019, or prior to initial osteoporosis diagnosis; history of cancer (C00–C96), bone tumors (D16, D48.0, and D49.2), or external causes of morbidity (V00–Y99); prior exposure to comparator drugs before the index date; age < 50 years at the index date, fewer than two prescriptions of the study drugs, hypoparathyroidism (E20) within one year before the index date, or diagnosed fractures or deceased within three months before or on the index date; and patients who switched between ROMO and TPTD/APTD after the index date [e.g., patients in the ROMO cohort must not have received TPTD or APTD, and vice versa].
Covariates
Baseline covariates associated with fracture risk, including demographics, comorbidities, and medication use, were assessed during the year preceding the index date. To minimize confounding, differences between ROMO users and the TPTD/APTD users were adjusted. Detailed covariates and their corresponding codes are provided in Supplementary Table 1.
Outcomes
Patients were followed from one day after the index date to 12 months thereafter. The primary outcome was osteoporotic fractures, categorized as vertebral fractures and non-vertebral fractures. vertebral fractures included cervical vertebra and neck fractures (S12), thoracic vertebral fractures (S22.0), lumbar vertebral fractures (S32.0), fatigue fractures of vertebra (M48.4), and collapsed vertebra not classified elsewhere (M48.5). Non-vertebral fractures included pelvic fractures (ilium [S32.3], acetabulum [S32.4], pubis [S32.5], ischium [S32.6], other pelvic fractures [S32.8]), hip fractures (head/neck of femur [S72.0], pertrochanteric [S72.1]), other femur fractures (S72), lower leg fractures including ankle (S82), shoulder/upper arm fractures (S42), and forearm fractures (S52). Secondary outcomes included all-cause mortality, hypocalcemia (E83.51), and hypercalcemia (E83.52) as positive control outcomes**.**
Subgroup analyses
We examined whether fracture, mortality, and calcium abnormality risks varied according to age, sex, prior fracture history, circulatory system disease, and chronic kidney disease (CKD). Age was stratified into 50–64 years and ≥ 65 years; sex as male or female; fracture history as presence or absence of fractures occurring three months to three years before the index date; and circulatory disease and CKD as present or absent.
Sensitivity analysis
To assess the robustness of the results, four sensitivity analyses were performed: (1) propensity score matching was performed using an alternative set of covariates, (2) addressing geographic variation by using global collaborative network, which includes more than 120 HCOs across 19 countries (the United Kingdom, Italy, Spain, Germany, Poland, Bulgaria, Lithuania, Brazil, India, Australia, Singapore, Malaysia, Taiwan, Japan, and the United States), thereby enhancing external validity in a more diverse population, (3) modified control cohort restricted to TPTD users only, and (4) given that romosozumab is typically limited to 12 months of use according to regulatory labeling and clinical guidelines, whereas TPTD may be administered for up to 24 months, we conducted a sensitivity analysis to address potential bias arising from the different approved treatment durations.
Statistical analysis
PSM was used to create cohorts with similar baseline characteristics, controlling for confounders. Matching was performed using a 1:1 greedy nearest-neighbor approach (TriNetX support documentation: https://support.trinetx.com/hc/en-us/articles/360011978033-In-compare-outcomes-how-are-patients-matched-when-balancing-cohorts/). Baseline balance was assessed using standardized mean differences (SMDs), with SMD < 0.1 considered well matched [31]. Kaplan–Meier survival analysis estimated outcome probabilities, with hazard ratios (HRs) and 95% confidence intervals (CIs) calculated using the survival package v.3.2–3 in R (R Foundation, Vienna, Austria), following TriNetX methodology (https://support.trinetx.com/hc/en-us/articles/360053133594-How-does-TriNetX-test-for-proportionality-on-a-hazard-ratio-). Log-rank tests determined differences between survival curves. Two-tailed p-values < 0.05 were considered statistically significant, and the proportional hazards assumption was verified using scaled Schoenfeld residuals.
Results
Baseline characteristics
A total of 17,477 patients were included in the present study. After applying propensity score matching, 2,258 users of ROMO and an equal number of PTH analog users were selected for analysis. The selection process is illustrated in Fig. 1. Table 1 summarizes the demographics, comorbidities, procedures, medications, and laboratory data of ROMO and PTH analog users before and after propensity score matching. Compared with TPTD/APTD users, ROMO users were generally older and more likely to be female at baseline. Additionally, fewer patients with cardiovascular disease were identified in the ROMO group. Most baseline characteristics were well balanced between the two groups (all standardized mean differences [SMDs] < 0.1), except for the use of antidepressants, antiepileptics, and alendronate.Table 1. Baseline characteristics of study subjects before and after PSM matching (PSM)VariablesBefore PSM^a^After PSM^a^Romosozumab users(n = 2985)PTH analogs users(n = 3778)SMDRomosozumab users(n = 2258)PTH analogs users(n = 2258)SMDCurrent age, mean ± SD70.9 ± 7.569.3 ± 7.70.20770.1 ± 7.470.1 ± 7.70.007Age at index, mean ± SD68.7 ± 7.566.2 ± 7.70.32667.6 ± 7.367.6 ± 7.60.002Sex, n (%) Female2867 (96.0)3381 (89.5)0.2552173 (96.2)2169 (96.1)0.009 Male30 (1.0)324 (8.6)0.36030 (1.3)33 (1.5)0.011 Unknown gender88 (2.9)73 (1.9)0.06655 (2.4)56 (2.5)0.003Race, n (%) White2339 (78.4)3020 (79.9)0.0391809 (80.1)1826 (80.9)0.019 Unknown race211 (7.1)346 (9.2)0.077173 (7.7)168 (7.4)0.008 Asian292 (9.8)169 (4.5)0.207154 (6.8)144 (6.4)0.018 Other race60 (2.0)137 (3.6)0.09858 (2.6)60 (2.7)0.006 Black or African American63 (2.1)90 (2.4)0.01854 (2.4)51 (2.3)0.009 Native Hawaiian or other Pacific islander13 (0.4)10 (0.3)0.02910 (0.4)10 (0.4)0.000 American Indian or Alaska native10 (0.3)11 (0.3)0.00810 (0.4)10 (0.4)0.000Family history of osteoporosis, n (%)46 (1.5)53 (1.4)0.01142 (1.9)39 (1.7)0.010Social economic status, n (%) Persons with potential health hazards related to socioeconomic and psychosocial circumstances14 (0.5)12 (0.3)0.02410 (0.4)10 (0.4)0.000Lifestyles, n (%) Personal history of nicotine dependence140 (4.7)200 (5.3)0.028108 (4.8)115 (5.1)0.014 Nicotine dependence62 (2.1)135 (3.6)0.09053 (2.3)53 (2.3)0.000 Tobacco use25 (0.8)39 (1.0)0.02019 (0.8)24 (1.1)0.023 Alcohol related disorders12 (0.4)17 (0.5)0.00710 (0.4)10 (0.4)0.000 Reduced mobility18 (0.6)20 (0.5)0.01011 (0.5)13 (0.6)0.012 Difficulty in walking, not elsewhere classified12 (0.4)10 (0.3)0.02410 (0.4)10 (0.4)0.000 Dependence on wheelchair10 (0.3)10 (0.3)0.01310 (0.4)10 (0.4)0.000Medical utilization/procedures, n (%) Office or other outpatient services1893 (63.4)2043 (54.1)0.1911369 (60.6)1339 (59.3)0.027 Preventive medicine services188 (6.3)308 (8.2)0.072167 (7.4)160 (7.1)0.012 Emergency department services98 (3.3)101 (2.7)0.03663 (2.8)63 (2.8)0.000 Hospital inpatient and observation care services40 (1.3)98 (2.6)0.09035 (1.6)39 (1.7)0.014 Surgical procedures on the femur and knee joint13 (0.4)16 (0.4)0.00211 (0.5)10 (0.4)0.007 Surgical procedures on the pelvis and hip joint15 (0.5)26 (0.7)0.02411 (0.5)14 (0.6)0.018 Surgical procedures on the spine12 (0.4)43 (1.1)0.08411 (0.5)10 (0.4)0.007Comorbidities, n (%) Disorders of lipoprotein metabolism and other lipidemias802 (26.9)1014 (26.8)0.001593 (26.3)617 (27.3)0.024 Vitamin D deficiency684 (22.9)956 (25.3)0.056550 (24.4)545 (24.1)0.005 Hypertensive diseases612 (20.5)823 (21.8)0.031457 (20.2)454 (20.1)0.003 Chronic lower respiratory diseases230 (7.7)365 (9.7)0.070177 (7.8)181 (8.0)0.007 Other forms of heart disease198 (6.6)366 (9.7)0.112163 (7.2)180 (8.0)0.028 Diabetes mellitus176 (5.9)284 (7.5)0.065141 (6.2)134 (5.9)0.013 Diseases of arteries, arterioles and capillaries115 (3.9)213 (5.6)0.08499 (4.4)94 (4.2)0.011 Ischemic heart diseases91 (3.0)192 (5.1)0.10376 (3.4)79 (3.5)0.007 Overweight and obesity90 (3.0)145 (3.8)0.04575 (3.3)66 (2.9)0.023 Other rheumatoid arthritis90 (3.0)163 (4.3)0.06975 (3.3)80 (3.5)0.012 Anemia, unspecified85 (2.8)179 (4.7)0.09975 (3.3)73 (3.2)0.005 Chronic kidney disease106 (3.6)133 (3.5)0.00274 (3.3)79 (3.5)0.012 Rheumatoid arthritis with rheumatoid factor71 (2.4)82 (2.2)0.01456 (2.5)59 (2.6)0.008 Diseases of liver67 (2.2)94 (2.5)0.01643 (1.9)47 (2.1)0.013 Cerebrovascular diseases47 (1.6)101 (2.7)0.07640 (1.8)47 (2.1)0.023 Heart failure34 (1.1)75 (2.0)0.06828 (1.2)33 (1.5)0.019 Malnutrition27 (0.9)46 (1.2)0.03123 (1.0)21 (0.9)0.009 Systemic lupus erythematosus22 (0.7)34 (0.9)0.01818 (0.8)18 (0.8)0.000 Unspecified dementia10 (0.3)10 (0.3)0.01310 (0.4)10 (0.4)0.000 Ankylosing spondylitis10 (0.3)11 (0.3)0.00810 (0.4)10 (0.4)0.000Medications, n (%) Corticosteroids for systemic use658 (22.0)920 (24.4)0.055501 (22.2)501 (22.2)0.000 HMG CoA reductase inhibitors471 (15.8)724 (19.2)0.089350 (15.5)435 (19.3)0.099 Antidepressants388 (13.0)749 (19.8)0.185310 (13.7)396 (17.5)0.105 NSAIDs356 (11.9)662 (17.5)0.158294 (13.0)347 (15.4)0.067 Opioids324 (10.9)598 (15.8)0.147280 (12.4)273 (12.1)0.009 Antiepileptics304 (10.2)625 (16.5)0.188241 (10.7)320 (14.2)0.106 Diuretics243 (8.1)399 (10.6)0.083198 (8.8)209 (9.3)0.017 Sex hormones and modulators of the genital system191 (6.4)373 (9.9)0.127166 (7.4)180 (8.0)0.023 Alendronate179 (6.0)300 (7.9)0.076128 (5.7)187 (8.3)0.103 Aspirin113 (3.8)235 (6.2)0.11293 (4.1)109 (4.8)0.034 Antipsychotics97 (3.3)132 (3.5)0.01485 (3.8)59 (2.6)0.066 Calcium84 (2.8)89 (2.4)0.02963 (2.8)50 (2.2)0.037 Zoledronic acid31 (1.0)26 (0.7)0.03827 (1.2)14 (0.6)0.061 Raloxifene27 (0.9)27 (0.7)0.02122 (1.0)14 (0.6)0.040 Risedronate20 (0.7)43 (1.1)0.04918 (0.8)27 (1.2)0.040 Ibandronate19 (0.6)42 (1.1)0.05114 (0.6)23 (1.0)0.044 Calcitonin10 (0.3)10 (0.3)0.01310 (0.4)10 (0.4)0.000Laboratory, n (%) Body mass index (BMI), ≧ 30 kg/m^2^284 (9.5)395 (10.5)0.031221 (9.8)217 (9.6)0.006 Calcium in serum, < 6.5 mg/dL10 (0.3)10 (0.3)0.01310 (0.4)10 (0.4)0.000 eGFR, < 60 mL/min/1.73 m^2^423 (14.2)443 (11.7)0.073294 (13.0)287 (12.7)0.009 Phosphate in serum, < 3.5 mg/dL381 (12.8)515 (13.6)0.026290 (12.8)292 (12.9)0.003 Calcidiol in serum, < 30 ng/mL98 (3.3)196 (5.2)0.09586 (3.8)82 (3.6)0.009PSM: propensity score matching, PTH: Parathyroid hormone, SMD: standardized mean difference, SD: standard deviation, HMG CoA: hydroxy-3-methylglutaryl coenzyme A, NSAIDs: anti-inflammatory and anti-rheumatic products, non-steroids, eGFR: Glomerular filtration rate/1.73 sq M. predicted in serum, plasma or blood by creatinine-based formulaIf the patient is less or equal to 10, results show the count as 10Bold font represents a standardized difference was more than 0.1^a^ Propensity score matching was performed on age, sex, race, family history of osteoporosis, social economic status, lifestyles, medical utilization/procedures, comorbidities, medication usage (corticosteroids, sex hormones, opioids), and laboratory results (calcium, phosphate, calcidiol, BMI, and eGFR)
Fracture, mortality, and calcium abnormalities
After PSM, ROMO cohort was associated with a significantly lower risk of osteoporotic fractures (HR: 0.711, 95% CI: 0.542–0.931) compared with TPTD/APTD users (Table 2). No significant differences were observed for vertebral fractures (HR: 0.704, 95% CI: 0.458–1.080), non-vertebral fractures (HR: 0.697, 95% CI: 0.425–1.141), hip fractures (HR: 0.365, 95% CI: 0.097–1.376), or all-cause mortality (HR: 0.707, 95% CI: 0.284–1.758), though risks were numerically lower with ROMO users. ROMO was also associated with a lower risk of hypercalcemia (HR: 0.707, 95% CI: 0.511–0.977) and a nonsignificant trend toward higher hypocalcemia (HR: 1.655, 95% CI: 0.892–3.071). Kaplan–Meier analysis demonstrated a significant difference in osteoporotic fractures (log-rank p = 0.012; Fig. 2).Table 2. Risk of outcomes from day 1 to 1 yearOutcomesPatients with outcomeHazard ratio (95% CI)^a^Romosozumab users (n = 2258)PTH analogs users (n = 2258)Osteoporotic fractures911250.711 (0.542–0.931)* Vertebral fractures36500.704 (0.458–1.080) Non-vertebral fractures27380.697 (0.425–1.141) Hip fractures10100.365 (0.097–1.376)All-cause mortality10110.707 (0.284–1.758)Hypocalcemia27161.655 (0.892–3.071)Hypercalcemia63870.707 (0.511–0.977)^^ p < 0.05PTH: Parathyroid hormone, CI: Confidence interval. NA: Not availableIf the patient is less or equal to 10, results show the count as 10^a^ Propensity score matching was performed on age, sex, race, family history of osteoporosis, social economic status, lifestyles, medical utilization/procedures, comorbidities, medication usage (corticosteroids, sex hormones, opioids), and laboratory results (calcium, phosphate, calcidiol, BMI, and eGFR)Fig. 2. Kaplan–Meier curves for osteoporotic fracture: individuals receiving ≥ 2 doses of romosozumab (ROMO) compared with those receiving ≥ 2 doses of teriparatide (TPTD) or abaloparatide (APTD) during 1-year follow-up
Subgroup analysis
Sex: Among females (n = 2179 matched pairs), ROMO use was associated with a lower risk of osteoporotic fractures (HR: 0.738, 95% CI: 0.567–0.960) (Supplementary Table 2, Fig. 3). In contrast, no significant difference was observed among males (n = 22 pairs; HR: 2.219, 95% CI: 0.201–24.50), likely reflecting the extremely small size in this subgroup. The formal test for interaction (p interaction = 0.371) was non-significant, suggesting that the treatment effect did not significantly differ between the subgroups. This result, however, should be interpreted with caution, as the small sample size in the male group may have limited the power to detect a true interaction effect. In females, ROMO was also associated with a reduced risk of hypercalcemia (HR: 0.699, 95% CI: 0.501–0.976). No significant differences were observed for vertebral, non-vertebral, or hip fractures, all-cause mortality, or hypocalcemia. Among males, all effect estimates were imprecise due to the extremely small sample size, and no significant associations were detected.Fig. 3. Subgroup analyses: risk of outcomes from day 1 to 1 year stratified by sex, age, fracture history, circulatory system diseases, and chronic renal disease
Age: Among patients aged ≥ 65 years (n = 1582 matched pairs), ROMO use was associated with a reduced risk of osteoporotic fractures (HR: 0.652, 95% CI: 0.484–0.879) (Supplementary Table 3). No significant differences were observed in patients aged 50–64 years (n = 732 pairs; HR: 0.681, 95% CI: 0.417–1.112). The interaction test was non-significant (p = 0.881), indicating no statistically significant heterogeneity of treatment by age. In both age groups, no significant differences were found for vertebral fractures, non-vertebral fractures, hip fractures, all-cause mortality, hypocalcemia, or hypercalcemia.
Fracture history: Among patients with prior fractures (n = 250 matched pairs), ROMO use was associated with reduced risks of osteoporotic fractures (HR: 0.659, 95% CI: 0.439–0.991) and vertebral fractures (HR: 0.544, 95% CI: 0.300–0.987) (Supplementary Table 4). In patients without a fracture history (n = 1,944 pairs), no significant differences were observed for osteoporotic fractures (HR: 0.735, 95% CI: 0.511–1.056) or vertebral fractures (HR: 0.848, 95% CI: 0.459–1.567). ROMO as not associated with hypercalcemia in patients with prior fractures (HR: 1.118, 95% CI: 0.431–2.899), whereas a significant association was observed in those without fracture history (HR 0.579, 95% CI 0.399–0.841). All interaction p values were nonsignificant (osteoporotic fracture: p = 0.694; vertebral fracture: p = 0.308; hypercalcemia: p = 0.207) indicating no statistically significant heterogeneity by fracture history. No significant differences were observed for nonvertebral fractures, hip fractures, all-cause mortality, or hypocalcemia in either subgroup.
Circulatory system diseases: In patients with circulatory disease (n = 762 matched pairs), ROMO use was associated with a reduced risk of osteoporotic fractures (HR: 0.660, 95% CI: 0.442–0.986) (Supplementary Table 5). A similar association was observed in those without circulatory disease (n = 1,419 pairs; HR 0.668, 95% CI 0.461–0.968). ROMO use was associated with a reduced risk of vertebral fractures in patients with circulatory disease (HR: 0.448, 95% CI: 0.226–0.887), whereas no significant difference was observed in those without circulatory disease (HR 0.681, 95% CI 0.373–1.242). ROMO was not associated with hypercalcemia in patients with circulatory disease (HR 0.717, 95% CI 0.448–1.149), while a significant association was detected in those without circulatory disease (HR 0.553, 95% CI 0.342–0.894). All interaction p values were nonsignificant (osteoporotic fracture: p = 0.965; vertebral fracture: p = 0.367; hypercalcemia: p = 0.449) indicating no statistically significant heterogeneity by circulatory disease status. In both subgroups, no significant differences were observed for nonvertebral fractures, hip fractures, all-cause mortality, or hypocalcemia.
CKD: Among patients without CKD (n = 1882 matched pairs), ROMO use was associated with reduced risks of osteoporotic fractures (HR: 0.731, 95% CI: 0.547–0.977), non-vertebral fractures (HR: 0.584, 95% CI: 0.344–0.989), and hypercalcemia (HR: 0.599, 95% CI: 0.406–0.883) (Supplementary Table 6). Conversely, among patients with CKD (n = 347 pairs), ROMO use was not associated with significant differences in osteoporotic fractures (HR: 1.191, 95% CI: 0.624–2.273), nonvertebral fractures (HR: 1.403, 95% CI: 0.445–4.421), or hypercalcemia (HR: 0.775, 95% CI: 0.385–1.558). All interaction p values were nonsignificant (osteoporotic fracture: p = 0.176; nonvertebral fracture: p = 0.173; hypercalcemia: p = 0.527), indicating no statistically significant heterogeneity by CKD status and likely reflecting limited power due to the relatively small CKD sample. No significant differences were found for vertebral fractures, hip fractures, all-cause mortality, or hypocalcemia in either subgroup.
Sensitivity analyses
First, after adjusting for an alternative set of covariates, the results remained consistent (Supplementary Table 7). Second, using the TriNetX Global Network to assess geographic differences, ROMO users showed nonsignificant trends toward lower risks of osteoporotic fractures (HR: 0.823, 95% CI: 0.637–1.064), vertebral fractures (HR: 0.731, 95% CI: 0.472–1.133), non-vertebral fractures (HR: 0.850, 95% CI: 0.548–1.319), hip fractures (HR: 0.489, 95% CI: 0.147–1.624), and all-cause mortality (HR: 0.891, 95% CI: 0.378–2.098) (Supplementary Table 8). A significant reduction in hypercalcemia risk was observed (HR: 0.639, 95% CI: 0.459–0.889), while no significant difference was found in the risk of hypocalcemia (HR: 1.565, 95% CI: 0.853–2.872).
Third, in a head-to-head comparison with TPTD users, ROMO cohort showed a significantly reduced risk of non-vertebral fractures (HR: 0.509, 95% CI: 0.279–0.931) and hypercalcemia (HR: 0.645, 95% CI: 0.439–0.947) (Table 3), while no significant differences were observed for other outcomes. Due to a small sample size (n < 10), hip fracture and mortality analyses were not available. Kaplan–Meier analysis indicated a nonsignificant trend toward a lower risk of osteoporotic fractures in ROMO users compared to TPTD users (log-rank p = 0.105; Supplementary Fig. 1).Table 3. Risk of outcomes from day 1 to 1 year in a modified control cohort restricted to teriparatide users onlyOutcomesPatients with outcomeHazard ratio (95% CI)^a^Romosozumab users (n = 1586)Teriparatide users (n = 1586)Osteoporotic fractures75950.779 (0.576–1.055) Vertebral fractures32420.753 (0.475–1.192) Non-vertebral fractures16310.509 (0.279–0.931)* Hip fractures < 10 < 10NAAll-cause mortality < 10 < 10NAHypocalcemia20121.652 (0.808–3.380)Hypercalcemia43660.645 (0.439–0.947)^^ p < 0.05CI: Confidence interval. NA: Not available^a^ Propensity score matching was performed on age, sex, race, family history of osteoporosis, social economic status, lifestyles, medical utilization/procedures, comorbidities, medication usage (corticosteroids, sex hormones, opioids), and laboratory results (calcium, phosphate, calcidiol, BMI, and eGFR)
Fourth, we extended the observation window to 366–730 days (i.e., the second treatment year) to examine the robustness of our findings beyond the initial 12-month period. Compared with presumed TPTD-continued patients, presumed ROMO-off patients exhibited a lower risk of hypercalcemia (HR: 0.487, 95% CI: 0.304–0.780) and nonsignificant trends toward reduced risks of osteoporotic fractures (HR: 0.739, 95% CI: 0.522–1.046), vertebral fractures (HR: 0.641, 95% CI: 0.348–1.182), and non-vertebral fractures (HR: 0.618, 95% CI: 0.337–1.133) (Supplementary Table 9). Data on hip fractures, mortality, and hypocalcemia were not reported due to small sample sizes.
Discussion
Osteoporosis reflects accelerated but imbalanced remodeling, resulting in cancellous and cortical bone loss with microarchitectural deterioration [1]. Restoring balance is the therapeutic goal, with signaling pathways central to treatment [32, 33]. Antiresorptive agents slow bone loss but cannot fully restore balance and may cause rare long-term complications such as osteonecrosis of the jaw or atypical femoral fracture [34]. For patients requiring potent anabolic effects without suppression-related adverse effects, TPTD is often chosen [4].
Recent studies suggest ROMO provides greater BMD gains, favorable safety, and higher adherence than TPTD [21, 35]. A network meta-analysis found that TPTD, APTD, and ROMO all reduced vertebral, non-vertebral, and hip fractures versus placebo, without significant inter-drug differences [36]. In our TriNetX U.S. analysis, after propensity matching, ROMO offered stronger protection against osteoporotic fractures, particularly in older (≥ 65 years old) women with prior fractures (3 months–3 years), with or without circulatory disease, or without CKD. ROMO reduced vertebral fracture risk in patients with fracture history or circulatory disease and non-vertebral fracture risk in those without CKD. These effects, consistent with rapid and greater BMD gains, were most evident during the first 12 months [21]. However, small sample sizes and missing subgroup data limit generalization, especially to men.
Subgroup analyses suggested hypercalcemia was less frequent with ROMO, especially in women without fracture history, circulatory disease, or CKD. Hypocalcemia occurred more often, particularly in women aged ≥ 65 years, without fracture history, and with benefits consistent across circulatory diseases status and CKD, although not statistically significant, underscoring the need for monitoring. Head-to-head comparison also showed ROMO carried a lower hypercalcemia risk without significantly increasing hypocalcemia versus TPTD.
Both APTD and TPTD increased BMD at the total hip, femoral neck, and lumbar spine at 6–18 months versus placebo [16]. APTD exceeded TPTD at most sites except the lumbar spine at 18 months, with significantly reduced major osteoporotic fracture risk. Bone turnover markers [procollagen type I N-terminal propeptide (PINP) and carboxy-terminal cross-linking telopeptide of type I collagen (CTX)] rose more with TPTD, indicating greater remodeling activity, although differences were nonsignificant [16]. Because efficacy differences were modest [3, 16], APTD was excluded from the main comparison. Compared with TPTD, ROMO demonstrated significant reductions in non-vertebral fractures and hypercalcemia, with residual benefit of hypercalcemia persisting after discontinuation, largely reflecting higher TPTD risk.
All three agents are generally safe but carry agent-specific warnings. The boxed 24-month limit for TPTD related to osteosarcoma risk was removed after 18 years of surveillance [10, 11], although it remains in place for APTD. ROMO is restricted to 12 months and carries an FDA warning against use in patients with recent CV events [18, 37], although the evidence underlying this concern remains debated [38, 39]. CV risk signals for ROMO are inconsistent: CV events were comparable between ROMO and placebo in postmenopausal women, and no excess risk over bisphosphonates has been demonstrated [19, 40]; however, several findings raise caution. In ARCH and a phase III trial in men, adjudicated serious CV events occurred more often with ROMO (2.5% vs. 1.9% vs. alendronate; 4.9% vs. 2.5% vs. placebo) [18, 37]. Pharmacovigilance data from Japan also suggest potential excess risk [41, 42], and multivariate analyses show higher odds of cardiac events in patients with pre-existing cardiac disease (OR = 5.9) or hypertension (OR = 1.6), and higher cerebrovascular risk in those with cerebrovascular disease (OR = 2.7) or hypertension (OR = 2.6) [42]. A meta-analysis of randomized trials further indicated that ROMO may increase composite arterial events compared with placebo, whereas abaloparatide was associated with lower odds of major adverse CV events or death (MACE) (OR = 0.25–0.31); these associations were attenuated when PTH analogues were pooled [43].
In contrast, a recent TriNetX analysis reported lower 1-year 3-point MACE rates with ROMO than with PTH analogues (158 vs. 211; P = 0.003), including fewer myocardial ischemic events (31 vs. 58; P = 0.003) and fewer cerebrovascular events (56 vs. 79; P = 0.037), along with a nonsignificant trend toward lower mortality [35]. These real-world findings suggest ROMO may not confer higher short-term CV risk, but the overall evidence remains conflicting and will require larger, more diverse, and methodologically rigorous studies to clarify.
In treatment-naïve patients or those previously exposed to antiresorptive agents, ROMO appeared more protective, likely reflecting its antiresorptive effect compared with the resorption increase seen with TPTD/APTD and TPTD alone. However, given the modest differences in efficacy, the extent to which ROMO is truly superior for individual patients remains uncertain [38, 39]. Beyond 12-month ROMO treatment window, discontinuation or transition to antiresorptive therapy has shown nonsignificant trends toward fewer osteoporotic, vertebral, and non-vertebral fractures compared with continued TPTD; nevertheless, prolonged antiresorptive therapy without intermittent remodeling raises concerns regarding microdamage accumulation.
Sequential strategies designed to maintain or further enhance prior BMD gains generally outperform prolonged monotherapy, with the important exception of transitions after denosumab, where rebound bone loss complicates subsequent management [30, 44–47]. Prior antiresorptive therapy may attenuate anabolic responses [20, 21], including the otherwise greater BMD gains achieved with ROMO compared with TPTD [27]. Post-anabolic antiresorptive consolidation or cyclic anabolic-antiresorptive regimens, therefore, remain essential in patients at very high fracture risk. Notably, sustained antifracture benefits for up to 30 months have been reported with TPTD followed by antiresorptive therapy [48], suggesting that TPTD may be preferable for patients with lower hypercalcemia risk who are likely require longer-term sequential or cyclic treatment approaches.
Limitations
This study has several limitations. First, reliance on the TriNetX U.S. network may limit generalizability, although findings were consistent in the Global network. Second, TriNetX is not a population-based dataset; its data are derived solely from participating HCOs. Medical encounters occurring outside the network are therefore not captured, which may result in incomplete follow-up and potential misclassification of exposures or outcomes when key clinical events take place elsewhere. Because TriNetX reflects only the population served by contributing HCOs, selection bias is possible, and the findings may not be fully generalizable to broader populations. Third, residual confounding and misclassification are inherent to electronic health records—based studies. Differences between TPTD and APTD may have introduced bias, although this was partially mitigated by a sensitivity analysis comparing ROMO with TPTD. Injection frequency and treatment duration differed across patients, which may have affected adherence. Baseline T-scores, trabecular bone scores, bone turnover markers, and supplementation data (e.g., vitamin D and calcium) were also incomplete. To reduce misclassification, we included patients with ≥ 2 osteoporosis diagnoses and no recent fractures. Finally, the applicability of these findings to non-Western populations remains uncertain.
Conclusions
In this real-world analysis, ROMO provided greater fracture protection than TPTD/APTD during the first year, with consistent trends in vertebral, non-vertebral, and hip fractures. Benefits were most evident in women with prior fractures or without CKD, regardless of circulatory disease status. ROMO showed a lower risk of hypercalcemia but a nonsignificant trend toward hypocalcemia, highlighting the need for monitoring. Despite small, matched samples, dosing differences, and limited follow-up, these findings support ROMO as a valuable option for severe osteoporotic women requiring rapid, short-term protection, especially after BPs. Therapy should remain individualized, considering fracture risk, comorbidities, safety, and long-term management strategies.
Supplementary Information
Supplementary material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tominaga R, Ikenoue T, Ishii R, Niihata K, Aita T, Okuda T, Shimizu S, Taguri M, Kurita N. Comparative cardiovascular safety of romosozumab versus bisphosphonates in Japanese patients with osteoporosis: a new-user, active comparator design with instrumental variable analyses. J Bone Miner Res. 2025.10.1093/jbmr/zjaf 01039823291 · doi ↗ · pubmed ↗