Methodological quality of systematic intervention reviews on vaccination
Antonia Pilic, Louise Henaff, Christoph A. Steffen, Madeleine Batke, Hanna Helene Linß, Iksha Thebe, Nina Rehr, Catalina Hamon Pinilla, Amrita John, Ole Wichmann, Vanessa Piechotta, Thomas Harder

TL;DR
This study finds that most systematic reviews on vaccination are of low methodological quality, with issues like poor protocol registration and lack of conflict of interest management.
Contribution
The study evaluates methodological quality of vaccination-related systematic reviews and identifies factors influencing their reliability.
Findings
110 out of 120 systematic reviews were rated as critically low-quality.
Reviews published after 2017 and Cochrane reviews showed higher methodological quality.
Only a quarter of reviews with conflicts of interest described how they managed them.
Abstract
Systematic reviews (SRs) are pivotal in vaccination recommendation development. However, the reliability of their findings relies on methodological rigor. This study examines the methodological quality of vaccination-related SRs and aims to identify influencing factors. We used the SYSVAC registry to draw 120 SRs on the efficacy or effectiveness of vaccination using a randomized block design. SRs published from 2011 to 2023 were considered. SR characteristics were extracted, and methodological quality was assessed by two reviewers using AMSTAR 2 (A Measurement Tool to Assess Systematic Reviews 2). SRs were scored between 0 and 16 and categorized as high, moderate, low, or critically low quality. Mann–Whitney U test, chi-squared test, Fisher’s exact test, and multivariable linear regression analysis were used to assess the influence of SR characteristics on AMSTAR 2 score. Secondary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
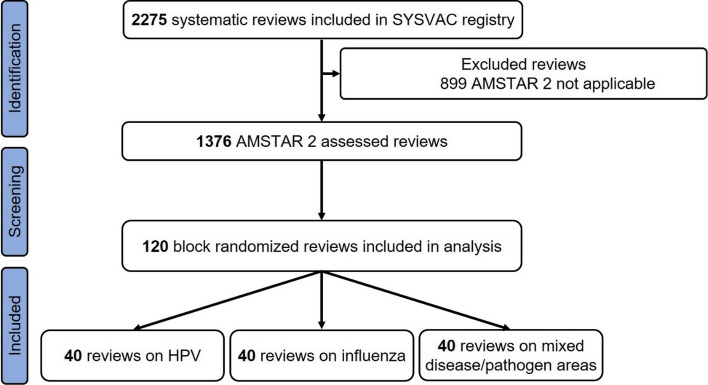 Figure 1
Figure 1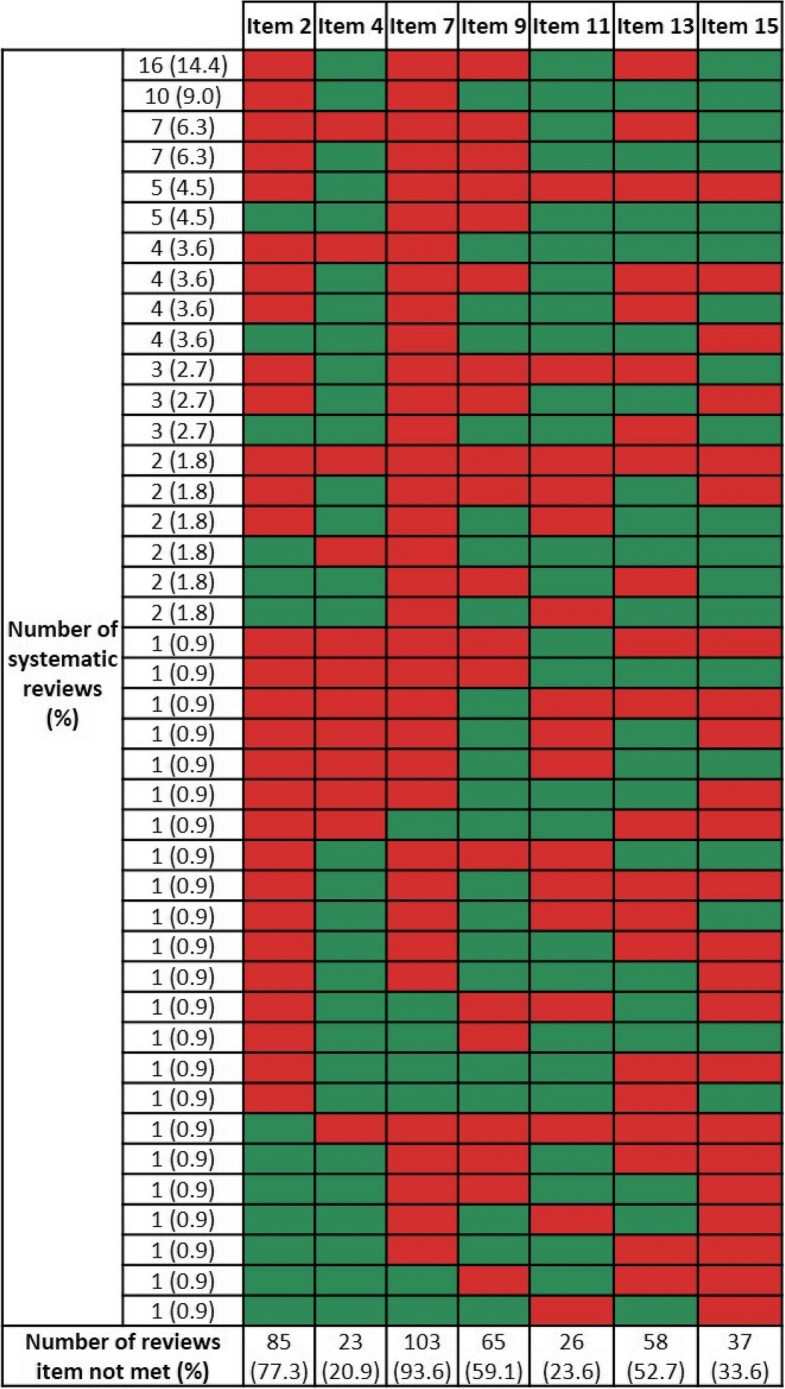 Figure 2
Figure 2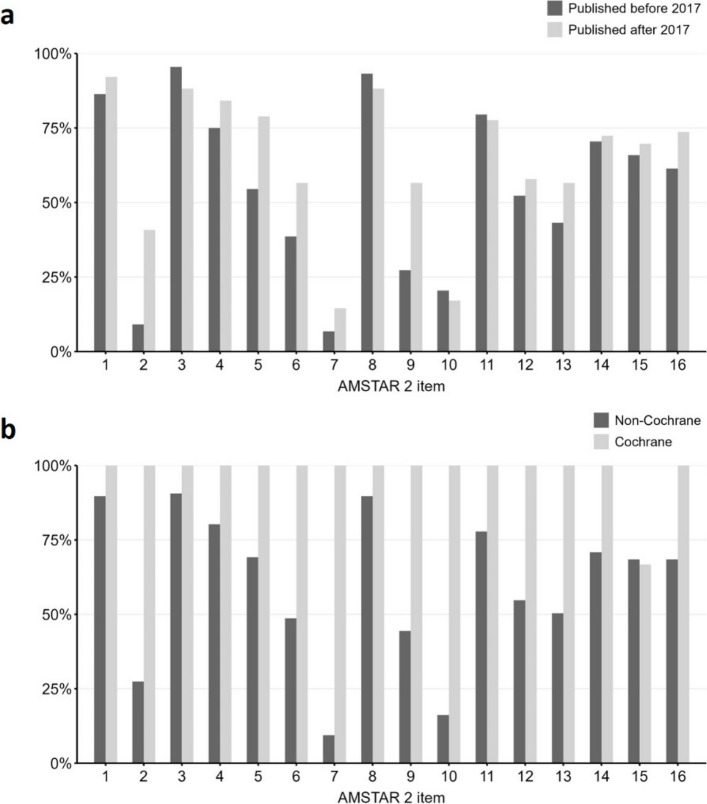 Figure 3
Figure 3- —Robert Koch-Institut (4255)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMeta-analysis and systematic reviews · Respiratory viral infections research · Vaccine Coverage and Hesitancy
Background
Critical assessment of the methodological quality of systematic reviews (SRs) is crucial. Among several tools available to assess the quality of SRs [1–3], AMSTAR 2 (A Measurement Tool to Assess Systematic Reviews 2) is one of the most often used [2, 4]. AMSTAR 2 was developed in 2017 for SRs of randomized and non-randomized controlled trials of healthcare interventions [2]. The tool consists of 16 items which have to be answered using four response categories (yes/partial yes/no/no meta-analysis conducted) [2]. A higher number of fulfilled items (i.e., answered by “yes”) corresponds to a higher methodological quality, ranging from a score of 0 to 16. Seven items are defined as being of critical importance. Based on identified flaws in items, AMSTAR 2 classifies the overall confidence of a SR into four categories: high, moderate, low, and critically low.
National Immunization Technical Advisory Groups (NITAGs) are independent expert groups which develop vaccination recommendations for national immunization programs [5]. Regarding efficacy, effectiveness, and safety of vaccines, NITAGs are requested to base their recommendations on best-available evidence, ideally the results of SRs. A recent bibliometric analysis showed a substantial increase in the number of vaccination-related SRs over the past decade, with a major proportion of them being rated as critically low in overall methodological quality [6]. However, no detailed analysis on the individual AMSTAR 2 items has been conducted in this study [6]. Using reliable and transparently reported SRs without methodological flaws is crucial for NITAGs to develop evidence-based vaccination recommendations, reducing the risk of false conclusions that could negatively impact decision-making and trust in the recommendation.
Therefore, the aim of this study was (i) to assess the methodological quality of SRs on the efficacy and effectiveness of vaccines and (ii) to investigate the characteristics influencing the methodological quality of these SRs.
Methods
We performed a cross-sectional study following a protocol developed a priori (see Additional file 1).
Database and review selection
We used the SYSVAC registry to draw a sample of SRs on the efficacy or effectiveness of vaccination. SYSVAC is a freely accessible database hosted by the NITAG Resource Center [7], which has its secretariat based at the World Health Organization (see www.nitag-resource.org/sysvac-systematic-reviews) [8]. As of 15 August 2024, SYSVAC comprised a total of 2275 SRs (including umbrella reviews) on vaccination-related topics. SRs included in SYSVAC are identified by monthly systematic literature searches conducted in MEDLINE on the OVID platform, Embase, the Cochrane Library of Systematic Reviews, and the Living Overview of Evidence repository [9] (for details, see Additional file 2 and [8, 10]). Outcomes considered in SYSVAC include microbiological, biological, or immunological markers (e.g., antibodies, immune cells), along with epidemiological factors (e.g., infection) and the impact on disease epidemiology (including indirect effects and impact on serotype distribution). We used block randomization to draw a sample of 120 SRs from SYSVAC. Blocks were defined according to a single vaccine-preventable disease being the topic of the respective SR, as follows: block 1: human papillomavirus (HPV), block 2: influenza, and block 3: other vaccine-preventable diseases. Thereby, each block included 40 SRs. Only SRs published between 2011 and 2023 were considered to focus on current trends and standards. The SYSVAC registry was initiated in 2011 and only SRs published from this time onwards are incorporated in the registry. The incorporation of SRs published in 2024 had not been completed at the time point of the analysis. All targeted populations and settings were eligible. Umbrella reviews were not considered.
Data extraction and methodological quality assessment
Two reviewers (AP, HL, MB, IT, NR, CP, AJ) extracted the following SR characteristics from the SRs into an Excel extraction form: year of publication; disease/pathogen focus of SR; number of authors; institution and country of corresponding author; Cochrane review; type of included studies in SR; funding information of SR; and declaration of conflicts of interest (CoI). The methodological quality was assessed by pairs of experienced SR methodologists (AP, HL, MB, IT, NR, CP) using AMSTAR 2 (published first in 2017 [2]), with minor adjustments of some items against the original tool for facilitated analysis (see Table 1 for further details). All 16 items were assessed, and judgments were justified by quotes. Each item was answered with either “yes”, “partial yes”, “no” or “no meta-analysis conducted” (if appropriate). Any disagreements where no guidance was available from the AMSTAR 2 tool guidance (e.g., item 16 on dealing with conflicts of interests) were solved through discussion until consensus was achieved. A summary score was calculated by summing the number of items fulfilled (i.e., answered by “yes”, “partial yes”, and “no meta-analysis conducted”). According to AMSTAR 2, high-quality denotes no or one non-critical weakness identified; moderate-quality denotes more than one non-critical weakness identified; low-quality denotes one critical flaw with or without non-critical weaknesses identified; and critically low-quality denotes more than one critical flaw with or without non-critical weaknesses identified (see Table 1 for critical items) [2]. Table 1. Description of original AMSTAR 2 items and adjustmentsItemDescription of original AMSTAR 2 item [2]Adjustment1Did the research question and inclusion criteria for the review include the components of PICO?-**2Was there “a priori” protocol designed and any significant deviations from the protocol justified?Only “yes” or “no” option as generally binary outcome3Was the selection of the study designs for inclusion in the review explained?Any information on study type sufficient to meet this item4Was a comprehensive literature search strategy used? (subitem: justified publication restrictions)**Any information on restrictions sufficient to meet subitem5Was study selection performed in duplicate?-6Was data extraction performed in duplicate?-**7Did the review authors provide a list of excluded studies and justify the exclusions?Only “yes” or “no” option as generally binary outcome8Were the included studies described in adequate detail?Only “yes” or “no” option as generally binary outcome9Was a satisfactory technique used for assessing the RoB in individual studies included in the review?**Only “yes” or “no” option as generally binary outcome10Were sources of funding for the studies included in the review reported?-**11**Were appropriate methods for statistical combination of results used?-12Was the potential impact of RoB in individual studies on the results assessed?-13****Did the review authors account for RoB in individual studies when interpreting/discussing the results of the review?-14Was a satisfactory explanation for, and discussion of any heterogeneity observed in the results provided?-**15**Was an adequate investigation on publication bias conducted and its likely impact on the results discussed?-16Were potential conflicts of interest declared and how were they dealt with?-Items in bold are critical items^^if meta-analysis conducted (term “meta-analysis” needs to be mentioned)PICO Population, Intervention, Comparator, Outcome, RoB Risk of bias
Statistical analysis
Descriptive statistics are displayed as median and range or frequencies and percentages, as appropriate. Differences in AMSTAR 2 score according to SR characteristics were compared using Mann–Whitney U test. Chi-squared test or Fisher’s exact test was used to compare individual AMSTAR 2 items. Multivariable linear regression was applied for influence analysis of SR characteristics on AMSTAR 2 score. Secondary analysis was conducted for SRs rated as critically low to identify limiting patterns of critical items (items 2, 4, 7, 9, 11, 13, and 15) that contributed to their AMSTAR 2 rating. For all analyses, the responses “yes”, “partial yes” and “no meta-analysis conducted” were combined into one response, and the item was considered to be fulfilled. P-values below 0.05 were considered statistically significant. All statistical analyses were carried out using R (version 4.4.1).
Results
The search in the SYSVAC registry identified 2275 SRs, of which 1376 SRs addressed interventions (i.e., efficacy or effectiveness of vaccines) and were therefore eligible for AMSTAR 2. According to study design, 120 SRs were included in the analysis (see Fig. 1 for flow chart). A list of the SRs not considered in this analysis is available upon request.Fig. 1. Flow chart of block-randomized selection process for systematic reviews on vaccination efficacy/effectiveness included in SYSVAC registry [8] AMSTAR 2 A Measurement Tool to Assess Systematic Reviews 2, HPV Human papillomavirus
About half of the included SRs were published in or after 2019 and had a median of five authors. Most SRs had a corresponding author with an academic background (n = 64; 53.3%), followed by a background in policy/government (n = 20; 16.7%). Three SRs were Cochrane reviews. The majority of SRs included randomized-controlled trials (RCTs; n = 87, 72.5%). Out of the 87 SRs with reporting on funding, 18 SRs (15.0%) were funded by pharmaceutical companies. Forty-three SRs (35.8%) reported that at least one author had a CoI. Table 2 summarizes further characteristics of the included SRs. Details on individual SRs are shown in Additional file 3. Table 2. Characteristics of included vaccination-related systematic reviews. N = 120Characteristics of systematic reviewsMedian (range) or n (%)Year of publication2019 (2011–2023)Disease/pathogen (intervention) HPV, Influenza (each)40 (33.3) Tuberculosis5 (4.2) Herpes zoster4 (3.3) Cholera, Dengue, HIB, Poliomyelitis, TBE, Varicella (each)3 (2.5) Hepatitis A, Yellow fever (each)2 (1.7) Diphtheria, Ebola, Herpes simplex, Meningococcal disease, Mpox, Mumps, Rabies, Streptococcus group B, Zika virus (each)1 (0.8)Number of authors5 (1–18)Institution of corresponding author Academia64 (53.3) Policy/government20 (16.7) Industry18 (15.0) Cross-sector18 (15.0)Country of corresponding author United States of America21 (17.5) China, United Kingdom (each)11 (9.2) Australia, Italy (each)10 (8.3) Canada9 (7.5) Switzerland5 (4.2) Brazil, Germany, Netherlands (each)4 (3.3) France3 (2.5) Bangladesh, Belgium, Denmark, Ireland, Republic of Korea, Peru, Portugal, South Africa, Spain, Taiwan (each)2 (1.7) Argentina, Guinea-Bissau, Hungary, India, Islamic Republic of Iran, Japan, Norway, Poland, Singapore, Sweden, Tanzania, Zambia (each)1 (0.8)Cochrane review3 (2.5)Study design included (multiple possible) RCTs87 (72.5) NRSIs65 (54.2) Single-arm studies15 (12.5)Funding by pharmaceutical company No69 (57.5) Not reported33 (27.5) Yes18 (15.0)Conflicts of interests declared No74 (61.7) Yes43 (35.8) Not reported3 (2.5)HIB Haemophilus influenzae type b, HPV Human papillomavirus, NRSIs Non-randomized studies of interventions, RCTs Randomized-controlled trials, TBE Tick-borne encephalitis
The methodological quality of most SRs was critically low, with flaws in more than one critical item (n = 110, 91.7%). Six SRs were of high quality (5.0%), of which four had flaws in one non-critical item (item 6, 10, 12, or 14). The median of the AMSTAR 2 score, including meta-analysis considering items, was 10 (range 2–16). Table 3 summarizes the methodological quality of the included SRs. Table 3. Methodological quality of included vaccination-related systematic reviews. N = 120Methodological quality of systematic reviewsMedian (range) or n (%)AMSTAR 2 overall confidence Critically low110 (91.7) High6 (5.0) Low4 (3.3) Moderate0 (0.0)AMSTAR 2 score10 (2–16)AMSTAR 2 score (excl. meta-analysis considering items 11, 12, and 15)9 (0–16)AMSTAR 2 A Measurement Tool to Assess systematic Reviews 2
Secondary analysis of critically low-rated SRs (n = 110) showed that the majority of them failed to meet two to four out of seven critical items (see Table 4 for number of critical items not met). Almost all critically low-rated SRs lacked the justification for excluding individual studies (item 7; n = 103, 93.6%) and did not report a protocol registration (item 2; n = 85, 77.3%). Only some SRs did not report an adequate literature search strategy (item 4; n = 23, 20.9%) or applied appropriate meta-analytical methods (item 11; n = 26, 23.6%). Most frequent combinations of unmet critical items were lack of protocol registration (item 2) plus lack of justification for excluding individual studies (item 7) plus no or inadequate risk of bias (RoB) assessment (item 9) and interpretation (item 13) (n = 16, 14.4%); or the lack of protocol registration (item 2) plus justification for excluding individual studies (item 7) (n = 10, 9.0%) (Fig. 2). All AMSTAR 2 ratings can be found in Additional file 4. Table 4. Limitations in AMSTAR 2’ critical items of critically low-rated systematic reviewsNumber of limitations in critical itemsNumber of SRs (n)%Two2926.4Three2522.7Four2825.5Five1816.4Six87.3All seven21.8Item 2 Protocol registration, Item 4 Adequacy of literature search strategy, Item 7 Justification for excluding individual studies, Item 9 Risk of bias assessment, Item 11 Appropriateness of meta-analytical methods, Item 13 Risk of bias interpretation, Item 15 Publication bias. Further information on AMSTAR 2 critical items can be found in Table 1 . *N *= 110Fig. 2Patterns of AMSTAR 2’s limitations in critical items of systematic reviews. Red indicates limitations and green fulfillment of an item. Item 2 Protocol registration, Item 4 Adequacy of literature search strategy, Item 7 Justification for excluding individual studies, Item 9 Risk of bias assessment, Item 11 Appropriateness of meta-analytical methods, Item 13 Risk of bias interpretation, Item 15 Publication bias. Further information on AMSTAR 2 critical items can be found in Table 1. N = 110
Bivariate analyses showed that SRs published after 2017 (AMSTAR 2 was published first in 2017 [2]) and Cochrane reviews had a significantly higher methodological quality than SRs published before 2017 (mean AMSTAR 2 score difference: 2; p = 0.004) and non-Cochrane reviews (mean AMSTAR 2 score difference: 6; p = 0.003). Furthermore, SRs with declared conflicts of interests were of significantly lower methodological quality than SRs with no conflicts of interests (mean AMSTAR 2 score difference: 2; p = 0.004). None of the other characteristics had an impact on the methodological quality (see Table 5 for bivariate analyses). Table 5AMSTAR 2 scores according to characteristics of vaccination-related systematic reviewsCharacteristics of systematic reviewsYes^a^No^a^p-value^b^Publication year after 2017^c^11 (3–16)9 (2–16)0.004Number of authors involved in systematic review ≥ 5^d^10 (3–16)9 (2–15)0.28Cochrane review16 (15–16)10 (2–15)0.003Type of included studies RCTs included10 (5–16)9 (4–15)0.24 NRSIs included10 (4–15)10 (5–16)0.46 Single-arm studies included11 (8–15)10 (4–16)0.08Funding by pharmaceutical company8 (3–15)10 (2–16)0.05Conflicts of interest8 (3–15)10 (2–16)0.004NRSIs Non-randomized studies of interventions, RCTs Randomized-controlled trials^a^Median (range)^b^Mann-Whitney U-test^c^AMSTAR 2 was published first in 2017 [2]^d^Median of included authors in review
To further investigate which individual AMSTAR 2 items contributed to these differences, we compared SRs published before and after 2017, Cochrane reviews and non-Cochrane reviews, and SRs from authors with and without CoI. SRs published after 2017 had significantly higher methodological quality than SRs published before 2017 because of protocol registration (40.8% vs. 9.1%, critical item 2), study selection in duplicate (78.9% vs. 54.5%, non-critical item 5), and adequate RoB assessment (56.6% vs. 27.3%, critical item 9) (all p < 0.05, see Fig. 3a). Cochrane reviews had significantly higher methodological quality than non-Cochrane reviews because of protocol registration (100.0% vs. 27.4%, critical item 2), justification for excluding individual studies (100.0% vs. 9.4%, critical item 7), reporting of funding sources of studies (100.0% vs. 16.2%, non-critical item 10), and reporting the impact of RoB assessment of individual studies (100.0% vs. 54.7%, non-critical item 12) (all p < 0.05, see Fig. 3b). Interestingly, only a quarter of SRs with declared CoI described their approach for managing these conflicts (n = 9/43, 20.9%, non-critical item 16).Fig. 3AMSTAR 2 scores at item level (1-16) given as a percentage of systematic reviews receiving a “yes”, “partial yes”, or “no meta-analysis conducted” in a Reviews published before (n = 44) vs. after 2017 (n = 76). Groups are significantly different for critical items 2 and 9 and non-critical item 5 (p < 0.05; chi-squared test); and b Cochrane reviews (n = 3) vs. non-Cochrane reviews (n = 117). Groups are significantly different for critical items 2 and 7 and non-critical items 10 and 12 (p < 0.05; Fisher’s exact test). Item 1 PICO, Item 2 Protocol registration, Item 3 Study design, Item 4 Adequacy of literature search strategy, Item 5 Study selection in duplicate, Item 6 Study extraction in duplicate, Item 7 Justification for excluding individual studies, Item 8 Study characteristics, Item 9 Risk of bias assessment, Item 10 Funding sources of the included studies, Item 11 Appropriateness of meta-analytical methods, Item 12 Impact of the risk of bias assessment of individual studies, Item 13 Risk of bias interpretation, Item 14 Discussion of heterogeneity, Item 15 Publication bias, Item 16 Management of conflicts of interest. Further information on AMSTAR 2 items 1–16 can be found in Table 1
The multivariable linear regression analysis showed that 26% of the variability of the methodological quality of the SRs was explained by the eight factors in the model (R^2^ = 0.26; adjusted R^2^ = 0.17; see Table 6 for analysis). However, only the publication year after 2017 (yes/no) and Cochrane review status (yes/no) had a significant independent influence on AMSTAR 2 score. Table 6. Multivariable linear regression analysis: AMSTAR 2 score according to characteristics of vaccination-related systematic reviews (R^2^ = 0.26; adjusted R^2^ = 0.19)Characteristics in the modelBetaT**p-valuePublication year after 2017^a^−1.730−2.7490.008Number of authors involved in systematic review ≥ 5^b^−0.121−0.2130.832Cochrane review−5.690−3.2170.002Type of included studies RCTs included0.0100.0120.990 NRSIs included−0.335−0.4690.641 Single-arm studies included−0.424−0.4170.678Funding by pharmaceutical company0.8621.0340.305Conflicts of interest0.5480.7680.445RCTs Randomized-controlled trials, NRSIs Non-randomized studies of interventions^a^AMSTAR 2 was published first in 2017 [2]^b^Median of included authors in review
Discussion
This methodological study used the AMSTAR 2 tool to assess the methodological quality of vaccination-related SRs and to identify sources and determining factors of critically low quality. We found only a minority of SRs of high quality, particularly those published in the Cochrane Library. The predominance of critically low-quality SRs in our random sample of vaccination-related SRs is concerning, considering their relevance in guiding global and national vaccination policies. Recent overviews of SRs on COVID-19 or influenza vaccination showed similar results regarding the proportion of critically low-rated SRs [11–14].
Our results showed that the most often unmet critical items of AMSTAR 2 were related to the justification for excluding individual studies and the protocol registration (items 7 and 2), leading to a critically low rating. This observation was also made in overviews of SRs in other areas of medicine, such as non-operative treatments for proximal humerus fractures [15]. Justifying the exclusion of individual studies in a SR increases transparency and reproducibility and supports the understanding of the eligibility criteria of the review. Protocol registration not only informs researchers about ongoing SRs, thereby helping to avoid redundancy, but also increases transparency and minimizes the potential for bias [16].
A recent bibliometric analysis of vaccination-related SRs showed that the proportion of SRs with high quality increased from 9% in 2017 to 22% in 2018 [6], which coincides with the release of AMSTAR 2 and the Cochrane Collaboration Handbook for review authors [2]. This might indicate an increasing awareness in the research community regarding methodological standards for the conduct of SRs. Making protocol registration in platforms like PROSPERO mandatory by publishers might further enhance transparency and minimize reporting bias [17, 18]. Other strategies may be enforcement of compliance with reporting guidelines such as PRISMA, or incentives for rigorously conducted SRs with greater recognition and support through funding agencies and academic institutions [19, 20].
So far, two studies have assessed the methodological quality of SRs on influenza vaccination [21, 22]. Using the first version of the AMSTAR tool, Remschmidt et al. also found that the Cochrane review status (Cochrane review vs. non-Cochrane review) had an impact on the methodological quality of SRs on influenza vaccination [21]. However, in their sample of SRs, major flaws were observed with regard to study selection in duplicate, inclusion of grey literature, and justification for excluding individual studies [21]. These results differ from those of our study, where Cochrane reviews differed from non-Cochrane reviews regarding protocol registration, justification for excluding individual studies, funding sources of the included studies, and the impact of the RoB assessment of individual studies (item 2, 7, 10, and 12). Additionally, our results showed that SRs published after 2017 (i.e., after publication of AMSTAR 2) were of higher methodological quality. Differences in the quality between SRs published after and before 2017 were due to protocol registration, study selection in duplicate, and RoB assessment (item 2, 5, and 9). However, direct comparison between both studies is limited due to differences between the two versions of the AMSTAR tool. In contrast to another study on vaccination-related SRs published from 2016 to 2019 [22], we did not observe an impact of industry sponsorship on the methodological quality of SRs. However, similar to that study [22], the same proportion of industry-funded SRs (15%) was found. Even if funding by the pharmaceutical industry did not influence the methodological quality of vaccination-related SRs, the management of CoI (item 16) was poorly described and remains crucial for interpreting SRs and drawing reliable conclusions. Nevertheless, multivariable analysis showed no significant independent relation between CoI and AMSTAR 2 score. Cochrane review status or publication date could be accountable for the observed effect.
Given the high proportion of SRs on vaccination with critically low methodological quality in our sample, the question remains how to deal with these SRs in daily practice, in particular in situations when resources or time constraints limit the ability to conduct a new, more rigorous SR. The median AMSTAR 2 score of the included SRs in this study was 10, indicating that 62.5% of the 16 items were met. NITAGs, as recommendation-making bodies for immunization policies, can consider using these SRs despite their limitations. Available guidance can support NITAGs in the stepwise selection of SRs based on their methodological quality [23, 24]. Future research could explore the development of a guidance for the critical appraisal of SRs based on their individual AMSTAR 2 items in the decision-making process.
This study has two main limitations. First, due to limited resources, only a proportion of SRs selected by block-randomization could be analyzed. Since not all vaccination topics are represented in this sample (e.g., we do not have SRs on pneumococcal disease or rotavirus in the sample), the generalizability of our results might be questioned. Second, we acknowledge that calculating a summary score is not the recommended method for assessing methodological quality; however, this intuitive approach has already been adopted by others [22, 25] and we deemed it appropriate to use to facilitate descriptive analysis. Overall, this study provides an up-to-date overview on the methodological quality of vaccination-related SRs and provides a starting point for improving SR methodological standards.
Conclusions
Our study found critical methodological shortcomings in vaccination-related SRs. By addressing limitations, authors of newly developed SRs can improve the quality and reliability of evidence synthesis, thereby supporting robust decision-making in vaccination policy and practice. SRs provide the evidence base for public health decisions; therefore, ensuring their high methodological quality is essential. Future efforts should prioritize adherence to established methodological standards to enhance the impact of SRs and to inform evidence-based decision-making.
Supplementary Information
Additional file 1: Study protocol.Additional file 2: Search strategy.Additional file 3: Characteristics of included systematic reviews; n = 120. Additional file 4: Methodological quality assessment of included systematic reviews using AMSTAR 2; n = 120.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1SYSVAC. https://www.nitag-resource.org/sysvac-systematic-reviews. Accessed 18 Dec 2024.
- 2Epistemonikos. Living Overview of Evidence repository https://app.iloveevidence.com/loves/5e 6fdb 9669 c 00e 4ac 072701 d. Accessed 01 June 2024.
- 3Jo CL, Burchett H, Bastías M, Campbell P, Gamage D, Henaff L, et al. Using existing systematic reviews for developing vaccination recommendations: Results of an international expert workshop. Vaccine. 2021;39(23):3103–10. 10.1016/j.vaccine.2021.04.045. Pub Med PMID: WOS:000652613400001.10.1016/j.vaccine.2021.04.04533965256 · doi ↗ · pubmed ↗
- 4Yang D, Tian J, Shen C, Li Q. An overview and single-arm meta-analysis of immune-mediated adverse events following COVID-19 vaccination. Front Pharmacol. 2024;15. 10.3389/fphar.2024.1308768. Pub Med PMID: 2030346077.10.3389/fphar.2024.1308768 PMC 1120008038933672 · doi ↗ · pubmed ↗
- 5Angeletti PM, Marchi S, Trombetta CM, Altobelli E. Flu vaccine administration in the period before SARS-Co V-2 infection and its outcomes: an umbrella review. Prev Med Rep. 2024;38. 10.1016/j.pmedr.2023.102575. Pub Med PMID: 2029625204.10.1016/j.pmedr.2023.102575 PMC 1082025438283956 · doi ↗ · pubmed ↗
- 6Carregaro RL, Roscani ANCP, Raimundo ACS, Ferreira L, Vanni T, da Graca Salomao M, et al. Immunogenicity and safety of inactivated quadrivalent influenza vaccine compared with the trivalent vaccine for influenza infection: an overview of systematic reviews. BMC Infect Dis. 2023;23(1). 10.1186/s 12879-023-08541-0. Pub Med PMID: 2025175980.10.1186/s 12879-023-08541-0PMC 1046361037644401 · doi ↗ · pubmed ↗
- 7Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane handbook for systematic reviews of interventions version 6.5 (updated August 2024). The cochrane collaboration, 2024;2024. www.training.cochrane.org/handbook.
- 8Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane handbook for systematic reviews of interventions version 5.2.0 (updated June 2017). The cochrane collaboration, 2017;2017. www.handbook.cochrane.org.