Pain and high-impact pain in community-dwelling older adults in Australia and relation to sociodemographic and health-related factors, including physical disability, psychological distress, and quality of life
Grace Joshy, Saman Khalatbari-Soltani, Kay Soga, Melonie Martin, Sinan Brown, Fiona M. Blyth, Emily Banks

TL;DR
This study finds that high-impact pain is common in older adults in Australia and is strongly linked to lower socioeconomic status, health issues, and reduced quality of life.
Contribution
The study provides population-based evidence on the prevalence and correlates of general and high-impact pain in older adults.
Findings
High-impact pain affects 13% of older adults and is more common in women, older age groups, and those with lower income or education.
People with high-impact pain are significantly more likely to experience severe physical limitations and psychological distress.
High-impact pain is strongly associated with poor quality of life and self-rated health.
Abstract
Chronic pain is common and debilitating and significantly impacts quality of life (QoL). However, large-scale population-based evidence on general bodily pain, pain sufficient to impact daily life (high-impact pain), and their relation to sociodemographic and health-related outcomes is limited. Self-administered questionnaire data from the 45 and Up Study (Wave-2, 2012–2015), an Australian population-based cohort study, were used to estimate the prevalence of general and high-impact pain. Modified Poisson regression estimated age- and sex-adjusted prevalence ratios (PRs) quantified their relation to sociodemographic, behavioural, and health characteristics, as well as physical functioning, psychological distress, QoL, and self-rated health. Overall, the study included n = 142,313 participants. Among them, 31% reported moderate-to-severe bodily pain, and 13% reported high-impact pain.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
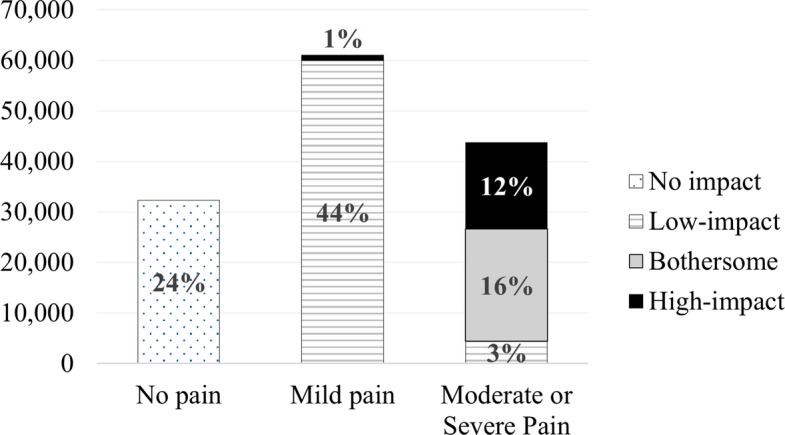 Figure 1
Figure 1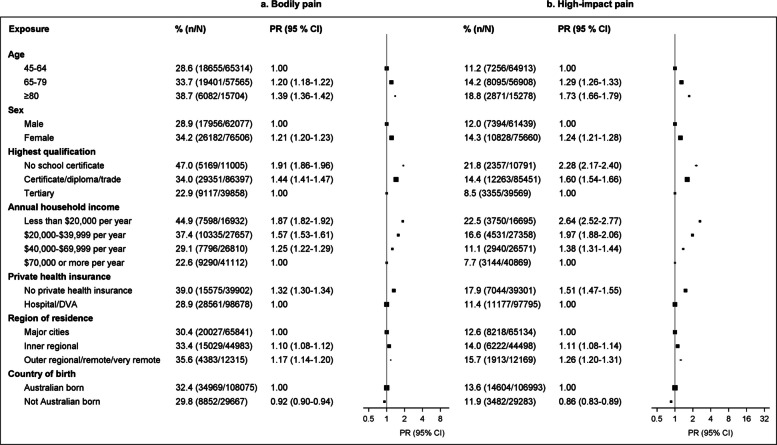 Figure 2
Figure 2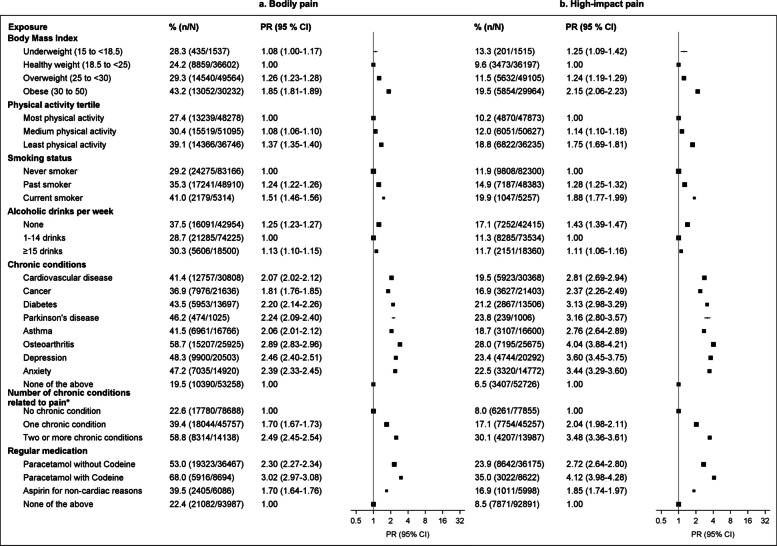 Figure 3
Figure 3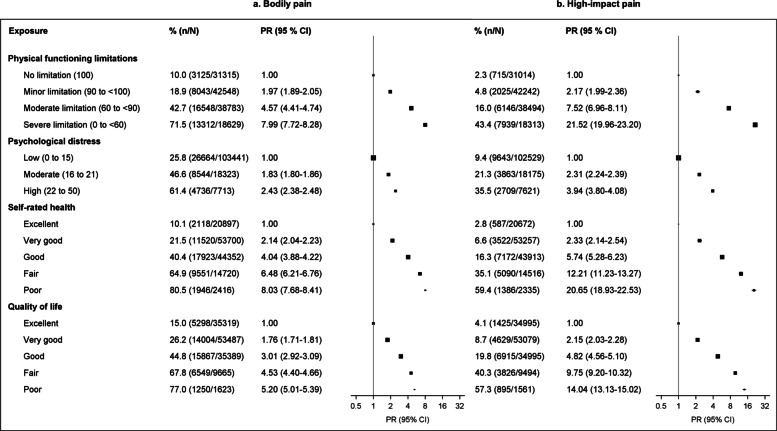 Figure 4
Figure 4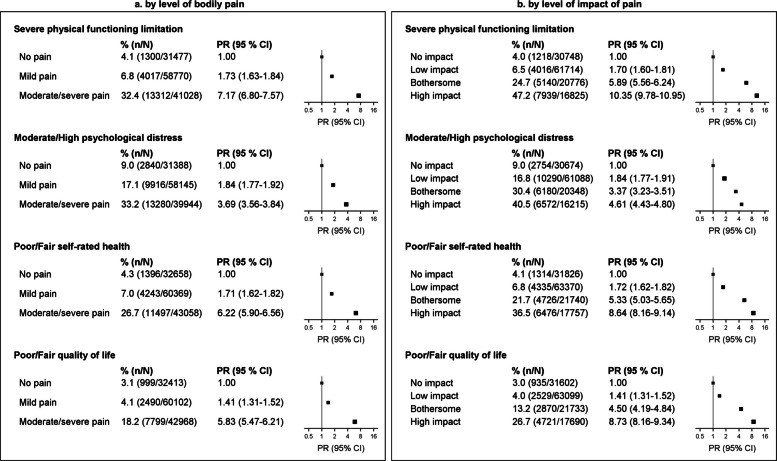 Figure 5
Figure 5- —Australian Research Council, Australia
- —https://doi.org/10.13039/501100000925National Health and Medical Research Council
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMusculoskeletal pain and rehabilitation · Pediatric Pain Management Techniques · Fibromyalgia and Chronic Fatigue Syndrome Research
Background
Chronic pain is common, affecting more than 30% of people worldwide [1, 2]; it is closely associated with reduced quality of life (QoL) and imposes a significant socioeconomic burden on individuals and society [1, 2]. Pain and related conditions, including low back pain, headaches, neck pain, and osteoarthritis, are leading causes of years lost to disability globally [3]. In 2018, 3.24 million Australians were estimated to be living with chronic pain, with the majority (56%) experiencing restrictions on the activities they are able to undertake in their daily lives [4].
The prevalence of pain varies across countries and communities, ranging from 10 to 50% [5]. Studies vary in terms of the type of pain investigated, assessment of severity and/or impact of pain, and the study population, with the majority being from the USA, UK, and Europe [5]. In general, pain is more common among females, middle-aged and older people, those with chronic disease, and those of low socioeconomic position, as indicated by lower levels of education, and smoking [5]. The prevalence of chronic pain is high in older age groups, driven by aging itself, disability, higher incidence of diseases, slower healing, and poorer recovery from acute injury [6]. Older adults are particularly vulnerable due to an increased risk for suffering from bothersome pain and reduced ability to cope or manage pain.
For people living with pain, the extent to which it interferes with daily life is of central importance. However, evidence on this is limited—especially in the general population. Most studies to date have focused on the nature of pain (e.g., chronic widespread pain [7]; transition from regional to widespread chronic pain [8, 9]), on single indicators of socioeconomic position [10, 11], demographic [12], or health-related factors [13, 14] as exposures, on specific population groups [15, 16], and many are limited by small sample sizes. Although pain has been shown to be associated with mental health conditions, disability, and QoL [17–19], evidence is particularly limited on pain that impacts daily life and how it relates to person-centred outcomes – outcomes that matter to individuals and are key determinants of the ability to live rich and meaningful lives [20]. Since debilitating pain has important social, economic, and health consequences, multidisciplinary approaches to pain management, enabling meaningful contributions from individuals to family, work, and social life, are a public health priority.
This study aimed to quantify the prevalence of bodily pain and pain sufficient to impact daily activities (high-impact pain) in a population-based cohort study of older adults, according to sociodemographic, behavioural, and health characteristics. A further aim was to examine the relationship of pain to adverse person-centred outcomes, including physical functioning limitations, psychological distress, self-rated health, and self-rated QoL.
Methods
Study participants
The Sax Institute’s 45 and Up Study is a cohort study of 267,357 men and women aged 45 years or over, randomly sampled from the general population of New South Wales (NSW), Australia, using the Services Australia Medicare enrolment database. People from regional and remote areas based on the Accessibility and Remoteness Index of Australia and those aged 80 years or over were oversampled. Individuals joined the study by completing postal questionnaires between 2005 and 2009 and consenting to long-term follow-up through repeated surveys and linkage of their data to other population health databases [21]. Details of the 45 and Up Study are described elsewhere [21].
The follow-up to the 45 and Up Study (Wave 2) was undertaken from 2012 to 2015, where eligible participants completed a questionnaire gathering data on health and lifestyle changes, as well as additional specific data on physical health and wellbeing. Participants who had requested not to be contacted further or were deceased (ascertained through linkages to death registries) were not included. A total of 142,548 participants completed the follow-up survey. Questionnaire data included comprehensive self-reported information including demographic factors, doctor-diagnosed health conditions, pain, functional capacity, mental health and self-rated health, QoL, height, weight, smoking, alcohol intake, and physical activity (Additional file 1: Tables S1–S2) [22, 23].
Following the exclusion of participants with study withdrawal requests, the original follow-up survey data from the Sax Institute consisted of 142,412 participants. We excluded participants with invalid baseline or follow-up questionnaire dates (n = 95, 0.07%) or baseline age under 45 (n = 4, 0.003%). The analysis dataset consisted of 142,313 individuals.
Outcomes
Main outcomes were bodily pain and its impact on daily life, based on two questions: (1) “How much bodily pain have you had during the past 4 weeks?”, followed by response options of none, very mild, mild, moderate, severe, and very severe; (2) “During the past 4 weeks, how much did pain interfere with your normal work (including both work outside the home and housework)?”, followed by response options of not at all, a little bit, quite a bit, moderately, and extremely. In binary classification, participants were considered to have bodily pain if they answered ‘moderate’, ‘severe’ or ‘very severe’. Participants were classified as having high-impact pain (at least ‘mild’ pain and ‘moderate’ or ‘extreme’ pain interference), bothersome pain (‘moderate’ or ‘severe’ pain and ‘a little’ pain interference), low-impact pain (‘moderate’ or ‘severe’ pain without any pain interference (‘not at all’) or ‘mild’ pain with ‘a little’ pain interference) or no impact of pain (no pain or pain interference) (Additional File 1: Tables S1, S3). From this, we also created a binary classification for high-impact pain (yes/no).
Adverse person-centred outcomes included severe physical functioning limitations, moderate or high psychological distress, poor or fair self-rated health, and poor or fair QoL (Additional File 1: Table S2). Physical functioning limitations were assessed using the Medical Outcomes Study Physical Functioning (MOS-PF) score [24] eliciting self-reported data on limitations in the ability to perform moderate and vigorous physical activities and tasks such as lifting or carrying shopping; climbing stairs; walking; bending, kneeling, or stooping; and bathing or dressing. The MOS-PF is a valid and reliable measure of physical functioning [25], with a lower score indicating more severe functional limitation. Scores ranged from 0 to 100 and were categorised as severe (0 to < 60), moderate (60 to < 90), minor (90 to < 100), or no (100) limitations. Psychological distress was assessed using the Kessler-10 (K10), a validated measure of non-specific symptoms of psychological distress [26]. Respondents indicated the frequency of symptoms experienced in the past 4 weeks, from 1 ‘none of the time’ to 5 ‘all of the time’. Scores ranged from 10 (no distress) to 50 (severe distress) [27] and were categorised as low (≤ 15), moderate (16 to 21), or high (22 to 50) distress. Self-rated health and QoL were based on the question, “In general, how would you rate your overall health/quality of life?”, followed by response options of excellent, very good, good, fair, and poor.
Sociodemographic, behavioural, and health-related factors
Sociodemographic characteristics included age, sex, education (no school certificate, certificate/diploma/trade, university degree), annual household income (< 20 K, 20–40 K, 40–70 K, ≥ 70 K), private health insurance, region of residence, and country of birth (Australian-born, not Australian-born) (Additional File 1: Table S2). Age at follow-up survey was categorised as 45–64 years; 65–79 years; and ≥ 80 years. The region of residence (derived from the address) was categorised as major city, inner regional, outer regional, and remote/very remote.
Health and behavioural characteristics included body mass index (BMI (kg/m^2^), 15 to < 18.5, 18.5 to < 25, 25 to < 30, and 30–50), physical activity (tertiles of physical activity sessions per week weighted for intensity), smoking status (never/past/current smoker), and number of alcoholic drinks per week (0, 1–14, ≥ 15 drinks per week), and chronic health conditions (based on responses to the question “has a doctor ever told you that you have…”), followed by a tick list of conditions (Additional File 1: Table S2); we considered cardiovascular disease (high blood pressure, stroke or blood clot), cancer, diabetes, Parkinson’s disease, asthma, osteoarthritis, depression, and anxiety. Individual chronic conditions (yes/no), as well as the number of chronic conditions with a known relationship to pain (cancer, diabetes, osteoarthritis, anxiety, and depression) grouped as none, one, or two or more, were considered [28]. Sensitivity analysis considered the number of chronic conditions, grouping three conditions with no specific relationship to pain (cardiovascular disease (CVD), Parkinson’s disease, and asthma), as well as grouping all eight conditions irrespective of the relation with pain. Regular medications were based on responses to the question, “Have you taken any medications for most of the last 4 weeks?”, followed by a tick list of medications, which included ‘paracetamol without codeine’, ‘paracetamol with codeine’, and ‘aspirin for other reasons’. Indicators of physical and mental health included physical functioning limitations, psychological distress, self-rated health, and self-rated QoL. Lower back pain (yes/no) was assessed using responses to “In the past 4 weeks, have you had pain in your lower back?”.
Statistical methods
We excluded participants with missing data on bodily pain (n = 3730; 2.6%) and high-impact pain (n = 3711; 2.6%) from the corresponding analyses. After logical imputation and backfilling for K10 and MOS-PF scores, we excluded those with missing data on each adverse person-centred outcome from the corresponding analyses.
Descriptive statistics summarised levels of bodily pain and high-impact pain in the study population, overall and according to sociodemographic and health-related characteristics. We quantified variations in levels of pain across these characteristics; modified Poisson regression models estimated prevalence ratios (PRs) and 95% confidence intervals (CIs) adjusted for age and sex (where applicable). Further statistical adjustments were not done as the objective was to compare prevalences rather than establish causality.
To quantify variation in adverse person-centred outcomes according to the level of pain experienced by the individual, adjusted PRs for severe physical functioning limitations, high psychological distress, poor/fair QoL, and poor/fair self-rated health were estimated by levels of bodily pain (no pain, very mild or mild pain, and moderate, severe or very severe pain) and impact of pain (no impact, low-impact, bothersome, high-impact).
Results
The study sample included 142,313 participants; 54% of participants were aged > 65 years, 55% were women, and 78% were Australian-born (Table 1). Table 1. Characteristics of the study populationN**%Total participants142,313****100%**Age group (years) 45–6466,58047% 65–7959,23642% ≥ 8016,49712%Male63,81645%University degree40,59029%Annual household income $70,000 or more41,72029%Private health insurance (hospital/DVA)100,82771%Residing in major city67,56247%Australian-born110,84678%Body mass index, kg/m^2^ Underweight (15 to < 18.5)15991% Obese (30 to 50)31,08422%Highest physical activity tertile37,98827%Current smoker85,21160% ≥ 15 alcoholic drinks per week18,89813%Self-reported chronic condition Cardiovascular disease31,85222% Cancer22,26416% Diabetes14,20310% Parkinson’s disease10761% Asthma17,23112% Osteoarthritis26,77919% Depression21,12315% Anxiety15,38011% None of the above54,55738%Medications Paracetamol without codeine37,44526% Paracetamol with codeine90326% Aspirin for non-cardiac reasons62874% None of the above96,46368%Severe physical functioning limitations (MOS-PF score < 60)19,50314%Moderate/high psychological distress (K10 score 16–50)26,80319%Poor/fair self-rated health17,87413%Poor/fair quality of life11,8078%Received cancer treatment in last month45183%
Overall, nearly a quarter of the study population (24%) reported no pain, 45% reported mild pain, and nearly one-third (31%) reported moderate/severe bodily pain (Fig. 1). The impact of pain on day-to-day activities was low for 47%, bothersome for 16%, and high for 13% of participants. While there is no additional information on the location of pain, at least 50% of those reporting any bodily pain or its impact also reported lower back pain, while 14% of those not reporting bodily pain in general reported lower back pain (Additional File 1: Fig. S1).Fig. 1. The distribution of pain and its impact in the study population
Variations in pain and its impact according to sociodemographic and health-related factors
High-impact pain, and to a lesser extent bodily pain, was more common among older adults, women, those with low education, low household income, no private health insurance, and those living in outer regional/remote/very remote areas (Fig. 2; Additional File 1: Fig. S2; Additional File 1: Table S4), compared to other cohort members. Prevalence of high-impact pain increased steadily with increasing BMI and was higher among the least physically active (versus most active), and those currently smoking (versus never smoking) (Fig. 3). High-impact pain was more common in those reporting alcohol consumption of ≥ 15 drinks per week (17.1%) and was slightly elevated in those reporting no alcohol consumption (11.7%) versus moderate consumption (11.3%). Those diagnosed with any of the eight chronic conditions considered were around three to four times more likely to report high-impact pain, with prevalence ranging from 16 to 28% for specific conditions versus 6.5% for those with none of those conditions (Fig. 2; Additional File 1: Table S5). Considering various combinations of chronic conditions, high-impact pain varied by specific conditions individuals were diagnosed with but was much more common among those with multimorbidity (Additional File 1: Table S6). Prevalence of bodily pain and high-impact pain increased with the number of chronic conditions (Fig. 3; Additional File 1: Table S7); among people with two or more conditions with a known relationship to pain (osteoarthritis, diabetes, anxiety, depression, cancer), 58.8% reported bodily pain and 30.1% reported high-impact pain. Reported use of paracetamol with and without codeine was associated with a higher prevalence of pain outcomes. Similar patterns across population groups were observed for both high-impact pain and bodily pain, although stronger socioeconomic gradients, as well as stronger associations with adverse physical and mental health outcomes were observed for high-impact pain.Fig. 2. Prevalence of bodily pain and high-impact pain by sociodemographic characteristics. a Bodily pain. b High-impact pain. A total of 138,583 participants with valid data on bodily pain and 137,099 participants with valid data on the level of impact of pain contributed to the corresponding analyses. Models are adjusted for age (continuous variable) and sex, where applicable. Missing data in educational qualification, region of residence, and country of birth (0.95%, 11%, and 0.61%, respectively) were included as separate categories in the corresponding models; there were no missing data on age or sex. CI: confidence interval; PR: prevalence ratio adjusted for age and sex (where applicable)Fig. 3. Prevalence of bodily pain and high-impact pain by health and behavioural factors. a Bodily pain. b High-impact pain. ^*^Chronic conditions with a known relationship to pain—cancer, diabetes, osteoarthritis, anxiety, and depression. Models are adjusted for age (continuous variable) and sex. Missing data in risk factors were included as separate categories in the corresponding models. The proportion of missing data in risk factors was less than 2%, except for BMI (14.9%); there were no missing data in chronic diseases and regular medications, as that information was collected using tick boxes. CI: confidence interval; PR: prevalence ratio adjusted for age and sex
Compared to people with no physical functioning limitations, the prevalence of high-impact pain was two-fold in those with minor physical functioning limitations (4.8% versus 2.3%, PR = 2.17 [1.99–2.36]) and 21-fold in those with severe limitations (43.4%, PR = 21.52 [19.96–23.20]) (Fig. 4). Similarly, the prevalence of high-impact pain was 20-fold in those with poor versus excellent self-rated health (59.4% versus 2.8%, PR = 20.65 [18.93–22.53]), 14-fold in those with poor versus excellent QoL (57.3% versus 4.1%, PR = 14.04 [13.13–15.02]), and nearly four-fold in those with high versus low psychological distress (35.5% versus 9.4%, PR = 3.94 [3.80–4.08]). Bodily pain was much more common than high-impact pain in all these groups, with similar patterns but attenuated PRs observed (Fig. 4).Fig. 4. Prevalence of bodily pain and high-impact pain among participants by levels of physical functioning, psychological distress, self-rated health, and quality of life. a Bodily pain. b High-impact pain. Models are adjusted for age (continuous variable) and sex. Missing data in risk factors (1–7%) were included as separate categories in the corresponding models. CI: confidence interval; PR: prevalence ratio adjusted for age and sex
Prevalence of adverse person-centred outcomes according to levels of bodily pain and impact of pain
Levels of adverse person-centred outcomes—severe physical functioning limitations, moderate/high psychological distress, and poor/fair self-rated health and QoL— increased with increasing levels of pain and its impact (Fig. 5). For instance, 47.2% of people with high-impact pain had severe physical limitations, compared to 4.0% of those reporting no impact of pain on their day-to-day activities (PR = 10.35 [9.78–10.95]); 40.5%, 26.7%, and 36.5%, respectively, had moderate/high psychological distress (PR = 4.61 [4.43–4.80]), poor/fair QoL (PR = 8.73 [8.16–9.34]), and poor/fair self-rated health (PR = 8.64 [8.16–9.14]). Prevalence of adverse outcomes was four-to-seven-fold in those with moderate/severe bodily pain compared to those reporting no bodily pain.Fig. 5. Prevalence of severe physical functioning limitation, moderate/high psychological distress, poor/fair self-rated health, and poor/fair QoL according to levels of bodily pain and impact of pain. a By level of bodily pain. b By level of impact of pain. Models are adjusted for age (continuous variable) and sex. CI: confidence interval; PR: prevalence ratio adjusted for age and sex. Of the 138,583 participants with valid data on bodily pain, those with missing data on each additional outcome variable were excluded from the corresponding analyses: 7308 for physical functioning limitations, 9106 for psychological distress, 2498 for self-rated health, and 3100 for quality of life. Of the 137,099 participants with valid data on high-impact pain, those with missing data on each additional outcome variable were excluded from the corresponding analyses: 7036 for physical functioning limitations, 8774 for psychological distress, 2406 for self-rated health, and 2975 for quality of life
Discussion
This large population-based study of over 140,000 middle-aged and older Australians found that pain is common, with around one-third reporting moderate/severe bodily pain and around one-in-eight reporting high-impact pain. Older adults, women, those with lower education and income, and those living in regional or remote areas are more likely than others to experience pain, reflecting a strong socioeconomic gradient. People born outside of Australia reported lower levels of pain than Australian-born participants. Pain was also more common among those with lower levels of physical activity, current smoking, high alcohol consumption or abstinence, chronic conditions, higher BMI, and use of over-the-counter medications for pain relief.
Our findings suggest a close, complex, and potentially bi-directional relationship between pain and adverse person-centred outcomes. Prevalence of bodily pain and high-impact pain increased substantially with increasing levels of adverse person-centred outcomes. At the same time, levels of adverse person-centred outcomes increased markedly with increasing levels of bodily pain and impact of pain. Among those with the most adverse person-centred outcomes (severe physical functioning limitations, high psychological distress, poor self-rated health, and poor QoL), at least 61–81% reported bodily pain and 36–59% reported high-impact pain; PRs were 2-to-22-fold compared with participants not reporting those issues. Among those with the highest levels of pain (moderate/severe bodily pain or high impact of pain), around 27–47% reported severe physical functioning limitations, moderate/high psychological distress, or poor/fair self-rated health, and 18–27% reported poor/fair QoL; PRs were 4-to-10-fold compared with participants not experiencing pain or impactful pain.
Strengths and limitations
To our knowledge, this is the first Australian and largest study to quantify comprehensively the prevalence of bodily pain and the impact of pain, and to investigate high-impact pain in relation to sociodemographic, behavioural, and health-related factors. This study also adds to the evidence base on the relation of adverse person-centred health outcomes to pain and the impact of pain. The use of gradients on the impact of pain enabled a deeper understanding of the relationship between high-impact pain and person-centred outcomes, offering evidence to inform the development of multidisciplinary prevention and treatment strategies. In particular, this study highlights population groups with a higher prevalence of pain, including pain that affects their day-to-day functioning, as well as the broader problems experienced by those in pain.
The cross-sectional design of this study means caution should be applied to any causal interpretations. Temporal information on pain in relation to chronic conditions or person-centred outcomes was not available for this study. Our study population was randomly sampled from a whole-of-population database, representing about 10% of the entire NSW population in the target age group. The response rate was approximately 18%, consistent with similar cohort studies. Participants tend to be healthier than the general population in cohort studies, and attrition usually increases with every wave of follow-up. In general, nonparticipation and loss to follow-up tend to be more pronounced among the less advantaged and less healthy, leading to cohort studies often being an increasingly healthy, wealthy subpopulation [29]. Even when characteristics of follow-up samples are different to the initial sample, estimates on restricted samples can remain internally valid [30]. Hence, while the absolute estimates of pain prevalence may not be directly representative, the prevalence ratios (PRs), which are based on internal comparisons, are likely to be more generalisable [31]. We relied on survey data; most sociodemographic, health-related behaviours, and health-related determinants of pain and high-impact pain were self-reported. Of note, only data on country of birth were available (as a proxy for ethnicity), which warrants further studies on detailed ethnicity variables. Pain is based on self-report; linked clinical or qualitative interview data were not available to further understand issues such as how participants’ pain was addressed and whether they were currently able to access help from primary care providers.
Findings in the context of the literature to date and possible mechanisms and implications
To our knowledge, there are no previous studies that have holistically evaluated a range of sociodemographic, behavioural, and health-related factors in relation to pain and high-impact pain in Australia. Most available evidence, in Australia and globally, focuses on chronic pain and does not consider pain alongside other person-centred outcomes—such as physical disability, psychological distress, and QoL. The experience of pain is dynamic, and measures used to assess pain vary [32], limiting comparability across studies; most measures consider duration, severity, and/or impact. The revised version of the graded pain scale [33] allows differentiation of mild, bothersome, and high-impact chronic pain based on the number of pain days in the past three months and activity limitation days due to pain. Measurement of high-impact pain in large cohort studies is an active area of research [34]. Although the graded pain scale was not available for this study, we were able to identify high-impact pain as recommended [32, 33], using activity limitations. Regardless of differences in study design, pain assessment method, and sample population, the associations we report are broadly consistent with prior studies, indicating that little has changed or improved over time. This highlights a need for strengthened policy attention and adequate resourcing to address modifiable risk factors for pain and a need to implement evidence-based, multidimensional prevention, and treatment strategies, with our larger, more comprehensive study providing greater certainty to support such actions.
Prevalence of pain and high-impact pain increased with increasing age, which agrees with previous findings that mostly report an increase in chronic pain prevalence at late middle age and then either a plateauing of prevalence estimates or continually increasing prevalence [9, 35]. Of note, some studies report no associations between increasing age and pain [17, 36–39] and some report decreasing prevalence among older adults relative to younger adults [15, 40, 41]. These inconsistencies suggest that differences in population characteristics (e.g., sociodemographic factors, coping strategies, and resilience) and methods used to measure pain may influence these associations.
Considering sociodemographic indicators of pain, our results are in agreement with previous literature, including a higher prevalence of pain among women [7–9, 17, 35], those with low educational level and income level [10, 38, 40–47], and those living in regional/rural areas [5, 37, 44]. We found differences in pain and high-impact pain by country of birth (lower prevalence among non-Australian-born compared to Australian-born); previous literature, mainly conducted in the USA, also reports differences in pain outcomes by ethnicity, finding mostly higher prevalence of pain among Native American and multiracial adults and lower prevalence among Asian Americans [48].
Prevalence of both pain and high-impact pain were significantly higher among those with higher BMI, lower levels of physical activity, past and current smokers, and those with no or high levels of alcohol consumption. These health-related and behavioural characteristics, including high BMI [35], low levels of physical activity [49, 50], and smoking [35, 51, 52], have been found to be associated with pain in previous studies. Existing evidence indicates that abstinence from alcohol is a risk factor, and moderate alcohol consumption is an apparent protective factor for pain [35]. Our findings, of higher proportions of participants with high alcohol consumption or abstinence reporting pain, might be due to the sick quitter effect, whereby former drinkers with underlying health conditions are included in the non-drinking group [53]. Additionally, given the cross-sectional nature of this study, these results should be interpreted with caution, and longitudinal studies are needed to establish the direction of these complex associations.
Similar to our findings, previous studies report a higher prevalence of pain among those with comorbid conditions, many of which are known to cause pain, including cancer, gastrointestinal, psychiatric/mood conditions [15, 28] Parkinson’s disease [54], cardiovascular diseases [55–58], and musculoskeletal conditions [15, 41, 45, 59, 60]. In addition, existing evidence indicates that multimorbidity is associated with pain [15, 28, 61]; although we looked at specific patterns of co-occurrence and the number of chronic conditions, we could not examine multimorbidity in detail considering time since diagnosis or severity. For example, 16% of participants reported being ever diagnosed with cancer, but only 3% had received cancer treatment in the past month. Our finding of a higher prevalence of bodily pain and high-impact pain among those using paracetamol with and without codeine likely reflects the common use of analgesic medications available at the time of the survey in pain management.
This paper provides new insights into the relation of pain to physical disability, psychological distress, and QoL, potentially reflecting bidirectional relationships with adverse person-centred outcomes likely contributing to and being consequences of pain. Our findings are generally consistent with the limited integrated evidence from previous studies. For instance, significant associations have been found between anxiety, depression, or poor mental health and pain [40, 52, 62–65]. Poor vitality and physical function have been shown to be associated with pain progression [66]. Poor self-rated health [52, 60] and low QoL [18, 67] have been reported as risk factors for pain, while poor mental health has been shown to be a predictor [66]. Our study found markedly greater adverse person-centred health outcomes in participants reporting moderate/severe bodily pain and bothersome or high levels of impact of pain. While pain has been reported as a key factor limiting activity/functioning [68, 69], there is limited evidence on how adverse person-centred outcomes vary according to increasing levels of pain. For example, we could identify only one study (n = 17,543, Australian population) reporting marked gradients in psychological distress and self-rated health by levels of chronic pain and interference with daily activities [40]. No previous studies have reported on adverse person-centred outcomes according to the level of impact of pain.
The study was not designed to determine the causal mechanisms through which sociodemographic, health-related, or behavioural factors contribute to the development of pain or its progression. The factors considered in this study were found to be associated with both pain and high-impact pain, which the biopsychosocial model of pain supports [70]. These factors are interconnected and the fact that the strongest relationships observed in this study were between physical ill health/disability and pain suggests this as a potential underlying mechanism. For instance, demographic factors (e.g., age, sex, ethnicity, geographical context) and socioeconomic position (e.g., low education and income levels) are major factors that influence health, the pain experience, and pain-related outcomes. Further research with more detailed analyses considering temporality is needed to evaluate causal relationships.
Conclusions
Bodily pain that has a high impact on an individual’s ability to carry on with daily life affects around one in eight older community-dwelling participants. People of lower socioeconomic position and those with health problems, particularly physical disability, are more likely than others to experience high-impact pain. Among those experiencing high-impact pain, around half have severely reduced physical functioning and high psychological distress, and a quarter report poor/fair QoL. Findings inform prevention and management of pain and indicate that access to high-quality pain management would substantially improve outcomes.
Supplementary Information
Additional file 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Deloitte Access Economics. The cost of pain in Australia. Canberra, Australia: Deloitte Australia; 2019. Available from: https://www 2.deloitte.com/au/en/pages/economics/articles/cost-pain-australia.html.
- 2Schofield P, Ruskin A, Gibson S. Pain in Older Adults. International Association for the Study of Pain. 2021. Availale from: https://www.iasp-pain.org/resources/fact-sheets/pain-in-older-adults/. Accessed 1 Nov 2025.
- 3Sax Institute. The 45 and Up Study. Wave 2 Data Book: First Follow-Up, 2012–2015. Sydney, Australia: Sax Institute; 2021. Available from: https://www.saxinstitute.org.au/wp-content/uploads/W 2-databook-May 2021.pdf.
- 4Sax Institute. Data and technical information. Sydney, Australia: Sax Institute. Available from https://www.saxinstitute.org.au/solutions/45-and-up-study/use-the-45-and-up-study/data-and-technical-information/.
- 5Santos MC da Silva, Gabani FL, Dias DF, de Andrade SM, González AD, Loch MR, et al. Longitudinal associations of changes in physical activity and TV viewing with chronic musculoskeletal pain in Brazilian schoolteachers. P Lo S One. 2020;15:e 0234609.10.1371/journal.pone.0234609 PMC 729936732555745 · doi ↗ · pubmed ↗
- 6Bruehl S, Olsen RB, Tronstad C, Sevre K, Burns JW, Schirmer H, et al. Chronic pain-related changes in cardiovascular regulation and impact on comorbid hypertension in a general population: the Tromsø study. PAIN. 2018;159(1):119–27. 10.1097/j.pain.0000000000001070.10.1097/j.pain.000000000000107028953193 · doi ↗ · pubmed ↗