Serologic Evidence of Exposure to Burkholderia pseudomallei, Nigeria
Jelmer Savelkoel, Gabriel E. Wagner, Chiedozie K. Ojide, Katrin Frankenfeld, Anne Rudloff, Susanna J. Dunachie, Michaela Lipp, W. Joost Wiersinga, Ivo Steinmetz, Emma Birnie, Rita O. Oladele

TL;DR
The study found that 30% of healthy Nigerians showed signs of past exposure to the bacteria that causes melioidosis.
Contribution
This is the first study in Nigeria to use a protein microarray to detect exposure to Burkholderia pseudomallei.
Findings
30% of participants showed serologic evidence of exposure to Burkholderia pseudomallei.
The study used a protein microarray to detect exposure in healthy individuals.
Melioidosis may be more prevalent in Nigeria than previously reported.
Abstract
Melioidosis is an underreported cause of community-acquired pneumonia and sepsis in Nigeria. We conducted a cross-sectional study using a Burkholderia pseudomallei protein microarray in 500 healthy participants from Nigeria. We observed a serologic response supportive of past exposure to the causative agent of melioidosis in 30% of study participants.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
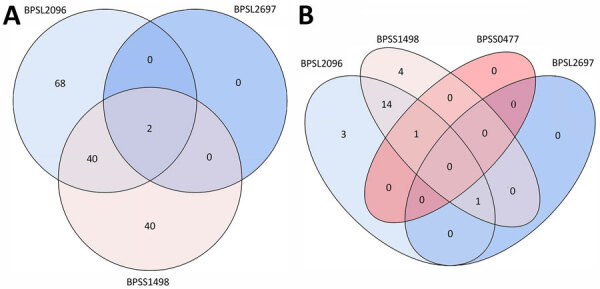 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBurkholderia infections and melioidosis · Brucella: diagnosis, epidemiology, treatment · Amyloidosis: Diagnosis, Treatment, Outcomes
Melioidosis is a severely neglected tropical disease that is prevalent yet highly underreported in Africa (1,2). Burkholderia pseudomallei, as its causative agent, is a gram-negative environmental bacterium, and exposure can lead to pneumonia, sepsis, and abscess formation; mortality rates sometimes exceed 40% (1). Nigeria is a high-priority country for melioidosis surveillance efforts in Africa because the disease burden is thought to the highest on the continent (2–4). However, current epidemiologic estimates in Nigeria are derived solely from modeling (3,4). Environmental distribution of B. pseudomallei has been established in Nigeria; the highest soil positivity rate has been demonstrated in the southeastern state Ebonyi (5). We hypothesized that environmental exposure to B. pseudomallei would result in a serologic response among inhabitants of Ebonyi state. Thus, we performed a cross-sectional study to assess the extent of a serologic response to B. pseudomallei in this state.
We recruited healthy participants using a convenience sampling approach in communities and the blood bank of the Alex Ekwueme Federal University Teaching Hospital Abakaliki. Adult participants were only able to take part if they could provide consent and were without suspicion of acute disease or febrile illness. Every consecutive participant meeting those criteria was recruited using a 1:1 ratio between communities and the blood bank. We obtained serum samples, and participants completed a short survey with questions on demographics and risk factors related to B. pseudomallei exposure.
We tested serum at a 1:2,000 dilution for the presence of IgG against a panel of 4 B. pseudomallei antigens (BPSL2096, BPSL2697, BPSS0477, and BPSS1498) spotted at a concentration of 1 mg/mL on the INTER-ARRAY platform (fzmb GmbH, https://www.inter-array.com), and we applied a signal intensity threshold of 0.3 on the basis of previous studies (6,7) (Appendix). We verified array performance with buffer control and nonpooled positive (melioidosis, culture-confirmed) and negative (healthy, nonendemic) control samples in every run. We screened serum of healthy participants from the hyperendemic region of Ubon Ratchathani, Thailand, collected as part of a previous study, in parallel with the same assay and used it as a comparator (n = 50) (6,8).
Ethical approval for use of the Nigeria samples was obtained from the Research and Ethics Committee of Alex Ekwueme Federal University Teaching Hospital Abakaliki (ref. no. 10/06-2022-02/08/2022). Ethical approval for the use of the Thailand samples was obtained from the Faculty of Tropical Medicine, Mahidol University (ref. no. TMEC 12-014), Sappasitthiprasong Hospital, Ubon Ratchathani (ref. no. 018/2555), and the Oxford Tropical Research Ethics Committee (ref. no. 64-11); study details can be found elsewhere (6,8).
We recruited 500 participants in Nigeria, 60.6% men and 39.4% women, with a median age of 30 (interquartile range 23–38) years; most reported farming activities and soil exposure as risk factors for exposure to B. pseudomallei (Table). We observed 150 (30%) participants with a positive serologic response to *>*1 antigen of our panel, compared to 23 (46%) participants for the Thailand cohort (Figure). We observed positivity to BPSS1498, also known as hemolysin coregulated protein and considered to be the prime serodiagnostic target for B. pseudomallei and B. mallei (7), in 82 (16.4%) participants from Nigeria (Table; Figure, panel A). In Thailand, 20 (40%) participants had a positive response to BPSS1498 (Figure, panel B). No participants from Nigeria had a positive response to >3 antigens. We included the variables age, sex, smoking and alcohol use, soil exposure and farming activity, and sampling location (community vs. blood bank) in a logistic regression model. However, we excluded diabetes from this model because of the limited number of events, despite it being a known risk factor for melioidosis (1). Using the previously mentioned model, we found no significant predictors of a positive serologic response in participants from Nigeria when taking into account all pooled antigens.
Strengths of our study include the use of a multiplex assay that includes BPSS1498, which alone proves more sensitive as a serodiagnostic target than the indirect hemagglutination assay, the standard for melioidosis serodiagnosis (9,10). Of note, BPSL2096 showed a higher positivity in participants from Nigeria than BPSS1498 did, which might reflect differences in bacterial strains, host factors, or both. However, further studies are needed to elucidate this observation. Our positive results are strengthened by the fact that we tested serum from participants from regions in Nigeria in which the pathogen has been detected in the environment. Also, we compared our results to a selection of healthy serum samples from an endemic area in northeastern Thailand to contextualize our results. Limitations include possible underestimation of the seropositivity rate because of the use of a serodiagnostic cutoff value for signal intensity established in culture-confirmed melioidosis patients (6) or overestimation because of possible but considered limited cross-reactivity after exposure to other species (9,10).
Our seroepidemiologic panel should be further refined relating to cutoffs in ongoing surveillance efforts in Nigeria and other sub-Saharan countries to map the epidemiology of melioidosis. Our seropositivity estimates of exposure to B. pseudomallei among persons in Nigeria can be used to inform future serosurveillance and validation work.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Meumann EM, Limmathurotsakul D, Dunachie SJ, Wiersinga WJ, Currie BJ. Burkholderia pseudomallei and melioidosis. Nat Rev Microbiol. 2024;22:155–69. 10.1038/s 41579-023-00972-537794173 · doi ↗ · pubmed ↗
- 2Birnie E, James A, Peters F, Olajumoke M, Traore T, Bertherat E, et al. Melioidosis in Africa: time to raise awareness and build capacity for its detection, diagnosis, and treatment. Am J Trop Med Hyg. 2022;106:394–7. 10.4269/ajtmh.21-067335008053 PMC 8832903 · doi ↗ · pubmed ↗
- 3Birnie E, Virk HS, Savelkoel J, Spijker R, Bertherat E, Dance DAB, et al. Global burden of melioidosis in 2015: a systematic review and data synthesis. Lancet Infect Dis. 2019;19:892–902. 10.1016/S 1473-3099(19)30157-431285144 PMC 6867904 · doi ↗ · pubmed ↗
- 4Limmathurotsakul D, Golding N, Dance DA, Messina JP, Pigott DM, Moyes CL, et al. Predicted global distribution of Burkholderia pseudomallei and burden of melioidosis. Nat Microbiol. 2016;1:15008. 10.1038/nmicrobiol.2015.827571754 · doi ↗ · pubmed ↗
- 5Savelkoel J, Oladele RO, Ojide CK, Peters RF, Notermans DW, Makinwa JO, et al. Presence of Burkholderia pseudomallei in soil, Nigeria, 2019. Emerg Infect Dis. 2023;29:1073–5. 10.3201/eid 2905.22113837081606 PMC 10124662 · doi ↗ · pubmed ↗
- 6Kohler C, Dunachie SJ, Müller E, Kohler A, Jenjaroen K, Teparrukkul P, et al. Rapid and sensitive multiplex detection of Burkholderia pseudomallei–specific antibodies in melioidosis patients based on a protein microarray approach. P Lo S Negl Trop Dis. 2016;10:e 0004847. 10.1371/journal.pntd.000484727427979 PMC 4948818 · doi ↗ · pubmed ↗
- 7Wagner GE, Berner A, Lipp M, Kohler C, Assig K, Lichtenegger S, et al. Protein microarray-guided development of a highly sensitive and specific dipstick assay for glanders serodiagnostics. J Clin Microbiol. 2023;61:e 0123422. 10.1128/jcm.01234-2236541753 PMC 9879090 · doi ↗ · pubmed ↗
- 8Jenjaroen K, Chumseng S, Sumonwiriya M, Ariyaprasert P, Chantratita N, Sunyakumthorn P, et al. T-cell responses are associated with survival in acute melioidosis patients. P Lo S Negl Trop Dis. 2015;9:e 0004152. 10.1371/journal.pntd.000415226495852 PMC 4619742 · doi ↗ · pubmed ↗