The mediating effect of triglycerides and related indices on the association between polycyclic aromatic hydrocarbons and oral health in adults aged ≥ 45 years from the national health and nutrition examination survey 2003–2016
Hua Shui, Weiling Liu, Qujie Li, Junhao Zhang, Cifeng Gao, Yong Wu, Chong Zeng, Wuling Chen, Fei Ma, Weiqi Liu

TL;DR
Exposure to certain pollutants called PAHs is linked to poor oral health in older adults, partly through effects on triglyceride levels.
Contribution
This study identifies triglyceride-related indices as mediators of PAHs' impact on oral health in adults aged 45+.
Findings
High exposure to 2-naphthol and 1-hydroxypyrene was associated with increased odds of poor oral health.
Triglyceride-related indices mediated up to 6.10% of the effect of 1-hydroxypyrene on oral health.
A significant interaction between 2-naphthol exposure and race was observed.
Abstract
Environmental pollutants are known determinants of oral health; however, the specific effects of polycyclic aromatic hydrocarbons (PAHs) on the oral health of adults aged ≥ 45 years remain poorly understood. This study investigated the association between PAH exposure and oral health and examined the mediating roles of triglyceride (TG) levels, the Triglyceride–Glucose index (TyG), and the Triglyceride–Glucose–Body Mass Index (TyG-BMI). This study utilized data of 4,442 individuals from the National Health and Nutrition Examination Survey. Logistic regression, weighted quantile sum (WQS) regression, and quantile-based g-computation (QGC) analyses assessed associations of urinary PAH metabolites with self-reported poor oral health. Mediation analysis evaluated the roles of TG, TyG, and TyG-BMI. Exposure in the highest quartile to 2-naphthol (2-NAP) and 1-hydroxypyrene (1-OHP) was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
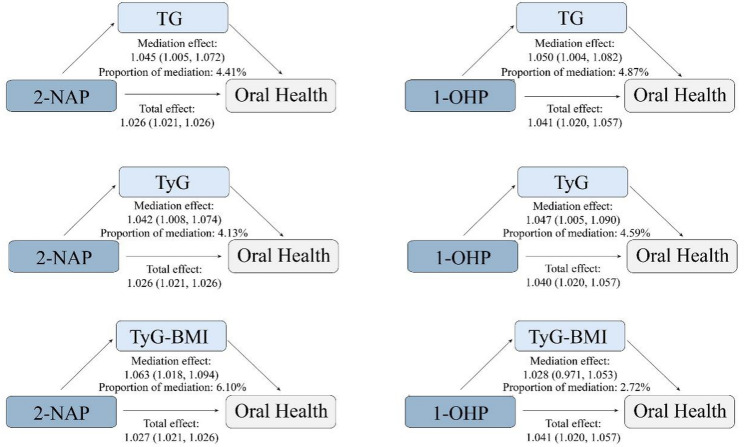 Figure 1
Figure 1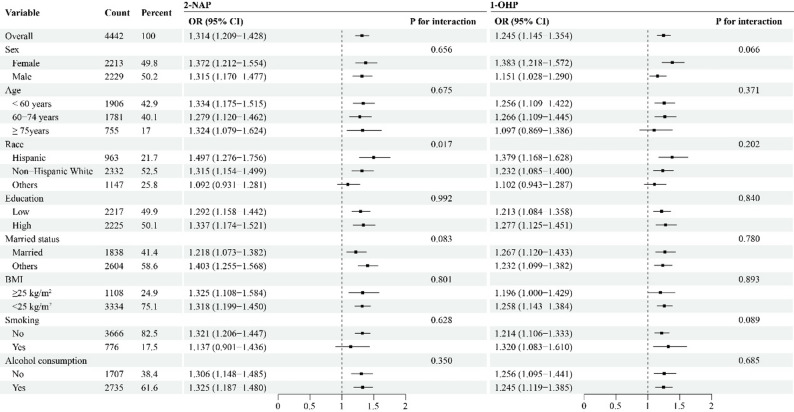 Figure 2
Figure 2- —Huadu District Basic and Applied Basic Research District-Institute Joint Funding Program
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsToxic Organic Pollutants Impact · Effects and risks of endocrine disrupting chemicals · Oral microbiology and periodontitis research
Introduction
Oral health a major global public health challenge, with World Health Organization (WHO) estimates suggesting that around 3.69 billion people worldwide are affected by oral diseases [1]. Studies indicate a higher prevalence of oral diseases among those aged ≥ 45 years. Ageing is accompanied by diminished reparative potential of periodontal apparatus and age-related immunosenescence [2], and immune function weakens, making this population more susceptible to pathogenic factors [3]. The WHO reports indicate that 42% of the population in the Western Pacific Region was affected by oral diseases in 2023, with people aged 45 and older comprising more than 60% of the cases. Additional studies suggest that oral health awareness is generally lower among people in this age group [4], and research conducted in Switzerland among participants aged ≥ 45 years demonstrated a significant link between age and caries and/or periodontal disease [5]. Similarly, a survey of Canadian adults aged 45 to 85 years found that over 30% of participants described multiple oral health concerns over the previous 12 months [6]. Furthermore, oral diseases exhibit strong linkages with several systemic disorders, including cardiovascular ailments, and deficits in nutritional metabolism and immune competence [7–9]. Therefore, further research into the epidemiological characteristics, pathogenic mechanisms, and comprehensive prevention and treatment strategies for oral diseases in people aged 45 and above is urgently needed.
The development of oral diseases is affected by multiple factors, including genetics, behaviour, inflammation, and environmental pollution [10–13]. Among these, the involvement of polycyclic aromatic hydrocarbons (PAHs) as potential risk factors has garnered increasing attention. PAHs belong to a category of environmentally persistent chemical pollutants defined by their condensed aromatic ring systems [14] and are widely present in both the natural environment and environments influenced by anthropogenic activities. Major exposure sources include household cooking, coal combustion, industrial emissions, and vehicular exhaust [15]. Numerous studies have shown that the accumulation of PAHs in the body can contribute to the pathological processes of various diseases, and their potential harm to oral health is being increasingly recognised [16, 17]. Current evidence supporting a link between PAHs and oral conditions is still insufficient. For instance, the underlying mechanisms through which PAHs affect oral health remain unclear, and differences in susceptibility to PAH exposure among various populations, particularly in middle-aged groups such as those aged 45 years, have not been sufficiently studied.
In addition, while triglycerides (TGs) and related indices, such as the Triglyceride–Glucose Index (TyG) and the Triglyceride–Glucose–Body Mass Index (TyG-BMI), have been widely demonstrated to play mediating roles in metabolic diseases [18–20], their capacity to act as mediators in the relationship between PAH exposure and oral diseases remains unclear. Elucidating the role of TG-related indicators in this context is especially critical for understanding health risks in the population aged 45 years, highlighting the importance of further investigation into these mechanisms for developing targeted prevention strategies.
To address this gap, the link between PAH exposure and oral health in adults aged ≥ 45 years and further assessed whether TG, TyG, and TyG-BMI mediate this association. This study hypothesised that exposure to specific PAH correlates with adverse oral health outcomes and that this association is partially mediated through triglyceride-related metabolic pathways. Clarifying these underlying mechanisms is vital to elucidate how pollutant exposure mediates oral diseases in this population, which could inform focused interventions.
Methods
Study cohort
This study analysed data from seven cycles of the NHANES, covering the period from 2003 to 2016. All selected cycles contained complete information on exposure, outcome, and covariate variables, ensuring the data integrity and reliability of the analyses. The study initially included 71,058 participants. After excluding individuals aged under 45 years and those with missing covariate data, the final analytical cohort comprised 4,442 subjects. A detailed participant selection flowchart (Figure S1) illustrates the exclusion criteria and the number of individuals excluded at each stage. A comparison was performed to examine possible selection bias between the included participants (n = 4,442) and eligible individuals aged ≥ 45 years who were excluded owing to missing data on covariates (n = 17,534). A comparison of demographic and socioeconomic characteristics revealed that the groups were broadly similar. Importantly, no significant differences were observed in key health-related variables, including sex, BMI, or smoking status, supporting the representativeness of the final cohort for the analyses (Table S1). The study received ethical approval from the National Center for Health Statistics Ethics Review Board (Protocols #98 − 12, #2005-06, and #2011-17). All participants provided written informed consent.
Assessment of urinary PAH metabolites
In this study, internal PAH exposure was assessed using urinary concentrations of monohydroxy-PAH metabolites from the NHANES database as biomarkers. The study was concentrated on six specific metabolites: 1-naphthol (1-NAP), 2-naphthol (2-NAP), 3-hydroxyfluorene (3-FLU), 2-hydroxyfluorene (2-FLU), 1-hydroxyphenanthrene (1-PHE), and 1-hydroxypyrene (1-OHP). Analyses were conducted via isotope-dilution on an integrated system for online purification, chromatographic separation, and tandem mass spectrometry, following enzymatic deconjugation of urine samples prior to automated extraction and chromatographic separation. The method demonstrated robust sensitivity, with detection limits of 0.008–0.09 ng/mL, as supported by linear calibration curves and stringent quality control measures. This validated methodology provided reliable quantification of exposure biomarkers for investigating associated health outcomes. Urinary concentrations were creatinine (Cr)-adjusted to account for variations in urine dilution, despite the physiological determinants of Cr excretion [21, 22], this correction was applied to align the data with the NHANES methodology. The normalised concentrations (in ng/g Cr) were subsequently natural log-transformed to better meet the assumptions of the parametric statistical models.
Outcome measures
This study principally assessed oral health status as a binary variable (good vs. poor). Given the use of self-reported questionnaire data rather than clinical diagnoses, the construct of “poor oral health” was operationalised as a state characterised by a patient-perceived negative impact on their quality of life or a negative global self-assessment. This approach is methodologically aligned with established public health research, which similarly defined health status groups by collapsing self-reported ratings (e.g., “fair/poor”) to capture meaningful negative perceptions of health [23]. During the 2003–2008 survey cycle, the variable OHQ630 (“How often do you feel bad because of your mouth?“) was used. Participants who reported responses such as “very often”, “fairly often”, or “occasionally” were considered to have experienced a perceptible negative bearing of oral health on their daily living and were thus assigned to the disease group. For the 2009–2016 survey cycle, the variable OHQ845 (“Overall, how would you rate the health of your teeth and gums?“) was used as an alternative measure. Participants who rated their health as “fair” or “poor” were included in the disease group, reflecting a negative perception of their oral health. The control group included participants from their respective survey cycles who gave an affirmative response to either of the following criteria: reporting “hardly ever” or “never” to OHQ630 or rating their oral health as “excellent”, “very good”, or “good” on OHQ845. Individuals with either negative self-perception or impaired quality of life were collectively defined as the disease group (i.e., poor oral health), thereby capturing a population with a clinically meaningful burden of symptoms for analysis.
Covariates
On the basis of previous studies [24–26] and data from this study population, the following covariates were selected: sex, age, race, education, marital status, body mass index (BMI), smoking status, alcohol consumption, poverty status, dietary inflammatory index (DII), and biochemical indicators (TG, uric acid [UA], and glucose [GLU]).
Age was categorised into three groups: <60 years, 60–74 years, and ≥ 75 years. Race was classified as Hispanic, non-Hispanic White, or other (which included non-Hispanic Black, multiracial and other individuals). Socioeconomic variables included education level (low: high school or below; high: college or above), poverty status (low: family income-to-poverty ratio [PIR] < 1.3; high: PIR ≥ 1.3), and marital status, categorised as married or other (including never married, divorced, or widowed). BMI was categorised as < 25 kg/m^2^ or ≥ 25 kg/m^2^. The lifestyle factors assessed included smoking status, categorised as non-smoker (comprising never and former smokers) or current smoker, and alcohol consumption status, classified as nondrinker (including never and former drinkers) or current drinker. The DII is a measure of a diet’s overall inflammatory potential [27], and the score was derived from NHANES dietary data and dichotomised as low (DII ≤ 0) or high (DII > 0). Serum concentrations of TG and UA were measured using the timed endpoint method, and the GLU concentration was determined by the hexokinase method with sample blank correction.
Statistical analysis
In accordance with the complex survey design of NHANES, a weighting methodology was applied in this study. Analytical guidelines for NHANES were followed, which included appropriate adjustment of the individual cycle weights to incorporate the seven cycles of data under examination. Continuous variables are summarised as medians with interquartile ranges, and categorical variables are reported as unweighted counts alongside weighted proportions. To avoid distributional assumptions and to ensure the robustness of statistical inference, nonparametric tests were employed for intergroup comparisons, and differences between the control and disease groups were assessed using chi-square tests. The associations among the PAH metabolites were assessed using Spearman’s rank correlation coefficient. Both univariate and multivariate logistic regression models were subsequently employed to evaluate the associations between these metabolites and the prevalence of oral health conditions. The findings are reported as odds ratios (ORs) alongside their 95% confidence intervals (CIs). The multivariate models were adjusted for potential confounders, including sex, age, race, education, marital status, BMI, smoking status, alcohol consumption, poverty status, DII, and UA. To account for multiple comparisons inherent in the quartile-based analysis of each PAH metabolite, the false discovery rate (FDR) was controlled via the Benjamini–Hochberg procedure, implemented separately for each metabolite.
To address the frequent high correlations among environmental exposures, the analysis utilised two complementary statistical methods: weighted quantile sum (WQS) regression and quantile‑based g‑computation (QGC). In the WQS approach, the six PAH metabolites were quartiles and combined into a weighted index. Stable estimates of component weights and their confidence intervals were derived from 1000 bootstrap samples. The resulting weights reflect the relative contribution of each metabolite to the overall mixture effect. As a complementary method, QGC was used to estimate the combined effect on the outcome following a simultaneous one-quartile increase in all exposures, thereby capturing both positive and negative contributions within the mixture. Both models were adjusted for the following covariates: sex, age, race, education, marital status, BMI, smoking status, alcohol consumption, poverty status, DII, and UA. For each model, the weights of individual PAH metabolites were calculated and visualised using bar plots to illustrate the relative importance of the mixture components. Subsequently, restricted cubic spline (RCS) analysis was performed on PAH metabolites that were significant in logistic regression and consistently identified as predictors in both WQS and QGC models.
To further investigate potential mechanistic pathways, a mediation analysis was performed using key PAH metabolites identified in previous analyses, testing the hypothesis that their effects may be partially mediated by triglycerides and related indices (TyG and TyG-BMI). The natural direct effect (NDE), natural indirect effect (NIE), and total effect were estimated, with 95% confidence intervals for the mediation effects based on 1000 bootstrap resamples. A significant mediation effect was defined as a confidence interval excluding zero. The TyG index was calculated as ln[TG×FBG/2], and the TyG-BMI index was calculated as TyG×BMI. Finally, subgroup analyses were performed: interaction terms between key PAH metabolites and these stratification variables were included in multivariate models to evaluate potential effect modification.
To test the sensitivity of the results to case definitions, a sensitivity analysis was conducted using stricter criteria for both survey cycles. For the 2003–2008 cycle, the case group was redefined to include only participants reporting “very often” or “fairly often” to OHQ630, excluding those reporting “occasionally”. For the 2009–2016 cycle, the case group was redefined to include only those reporting “poor” on OHQ845, excluding those reporting “fair”. All primary multivariate logistic regression analyses of these PAH metabolites were repeated using these more stringent case definitions.
R software was employed for all statistical analyses, using a two-sided P < 0.05 as the criterion for statistical significance.
Results
This study included a total of 4,442 participants, who were categorised into a disease group (n = 1,121) and a control group (n = 3,321) on the basis of oral health status. Between the two groups, significant differences were noted in multiple variables, with the disease group showing different distributions regarding age, race, education, marital status, smoking status, poverty status, DII, TG, GLU, and PAH metabolites—including 1-NAP, 2-NAP, 3-FLU, 2-FLU, and 1-OHP (all P < 0.05). In contrast, there were no significant differences in sex, BMI, alcohol consumption, or Cr, UA, or 1-PHE levels (all P > 0.05) (Table 1). a significant increasing trend in the prevalence of oral diseases (P for trend < 0.001), which was consistent across all sex and race subgroups (Table 2).Table 1. Characteristics by oral health status among participants in NHANES 2003–2016VariableControl group(n = 3321)Disease group(n = 1121)P-valueSex, n (%)0.178 Male1645 (49.5)584 (52.1) Female1676 (50.5)537 (47.9)Age, n (%)0.013 < 60 years1378 (41.5)528 (47.1) 60–74 years1310 (39.4)471 (42.0) ≥ 75 years633 (19.1)122 (10.9)Race, n (%)< 0.001 Hispanic615 (18.5)348 (31.0) Non-Hispanic White1878 (56.5)454 (40.5) Others828 (24.9)319 (28.5)Education, n (%)< 0.001 Low1528 (46.0)689 (61.5) High1793 (54.0)432 (38.5)Marital status, n (%)< 0.001 Married1297 (39.0)541 (48.3) Others2024 (61.0)580 (51.7)BMI, n (%)0.087 ≥ 25 kg/m^2^2468 (74.3)866 (77.3) < 25 kg/m^2^853 (25.7)255 (22.7)Smoking, n (%)< 0.001 No2836 (85.4)830 (74.0) Yes485 (14.6)291 (26.0)Alcohol consumption, n (%)0.016 No1244 (37.5)463 (41.3) Yes2077 (62.5)658 (58.7)Poverty status, n (%)< 0.001 Low721 (21.7)460 (41.0) High2600 (78.3)661 (59.0)DII, n (%)< 0.001 Low425 (14.9)96 (9.5) High2896 (85.1)1025 (90.5)Cr (mg/dL), median (P25, P75)94.00 (50.00, 146.00)96.00 (57.95, 143.00)0.418UA (µmol/L), median (P25, P75)321.20 (267.70, 380.70)321.20 (267.70, 392.60)0.645TG (mmol/L), median (P25, P75)1.41 (0.96, 2.15)1.59 (1.05, 2.47)< 0.001GLU (mmol/L), median (P25, P75)5.27 (4.83, 5.88)5.38 (4.88, 6.11)0.009PAH (ng/mg Cr), median (P25, P75) 1-NAP19.15 (9.22, 59.08)23.59 (8.96, 124.34)0.002 2-NAP32.19 (17.90, 67.46)59.48 (26.95, 128.82)< 0.001 3-FLU0.71 (0.44, 1.66)0.91 (0.46, 5.36)< 0.001 2-FLU1.92 (1.24, 3.98)2.41 (1.26, 9.64)< 0.001 1-PHE1.40 (0.88, 2.23)1.46 (0.84, 2.43)0.687 1-OHP0.95 (0.55, 1.69)1.24 (0.69, 2.58)< 0.001BMI body mass index, DII dietary inflammatory index, Cr creatinine, UA uric acid, TG triglyceride, *GLU *glucose, PAH polycyclic aromatic hydrocarbon, 1-NAP 1-Hydroxynaphthalene, 2-NAP 2-Hydroxynaphthalene, 3-FLU 3-Hydroxyfluorene, 2-FLU 2-Hydroxyfluorene, 1-PHE 1-Hydroxyphenanthrene, 1-OHP 1-Hydroxypyrene, P25 the 25th Percentile, P75 the 75th PercentileTable 2Trends in the weighted annualised prevalence of unhealthy oral conditions among U.S. Adults aged ≥ 45 years, 2003–2016CharacteristicPrevalence. % (95%CI)P for trend2003–20042005–20062007–20082009–20102011–20122013–20142015–2016overall9.8 (8.1–11.5)13.6 (10.0–17.2.0.2)10.5 (8.6–12.5)26.2 (21.4–31.0)28.2 (21.5–34.9)23.7 (20.6–26.7)29.3 (24.4–34.3)< 0.001Sex Male8.7 (5.9–11.6)13.2 (6.4–20.0)8.7 (6.9–10.4)30.7 (25.3–36.1)34.1 (25.8–42.5)23.6 (17.4–29.8)29.0 (20.4–37.5)< 0.001 Female10.7 (7.5–13.9)14.0 (10.0–18.0)12.2 (8.3–16.1)21.3 (15.4–27.1)23.1 (13.7–32.4)23.7 (19.6–27.8)29.6 (22.8–36.4)< 0.001Race Hispanic12.6 (4.0–21.2.0.2)31.4 (16.4–46.3)19.4 (14.2–24.6)46.1 (38.5–53.7)49.9 (39.3–60.5)40.4 (34.1–46.6)45.1 (34.3–55.9)< 0.001 Non-Hispanic White8.7 (6.5–10.9)12.5 (8.2–16.8)7.4 (5.1–9.7)21.6 (16.2–27.1)26.1 (18.1–34.0)20.8 (17.9–23.6)24.5 (19.9–29.2)< 0.001 Others14.1 (8.0–20.1.0.1)14.1 (7.8–20.3)23.8 (12.7–34.9)45.0 (33.6–56.3)28.4 (21.4–35.5)28.8 (20.1–37.4)44.0 (33.0–54.9.0.9)< 0.00195%CI, 95% confidence interval
As shown in Figure S2, the Spearman correlation analysis demonstrated statistically significant positive correlations for a number of urinary PAH metabolites (all P < 0.05), with particularly strong correlations observed between 2-FLU and 3-FLU (ρ = 0.92), between 2-FLU and 1-PHE (ρ = 0.67), and between 3-FLU and 1-PHE (ρ = 0.63). These findings suggest potential coexposure patterns or common sources, which may lead.
to combined effects on oral health. To systematically evaluate the associations, logistic regression models were used to assess the individual effects of each PAH metabolite on oral health status. Subsequently, WQS regression and QGC models were employed to quantify the combined effect of the mixture.
After covariate adjustment, there was a significant increasing trend for both 2-NAP and 1-OHP quartiles and poorer oral health (P for trend < 0.001), with the highest quartiles showing ORs of 1.96 (95% CI: 1.34–2.87) and 2.26 (95% CI: 1.51–3.39), respectively. No significant associations were observed for 1-PHE, 1-NAP, 3-FLU, or 2-FLU (Table 3).Table 3. Odds ratios and 95% confidence intervals for the associations between quartiles of urinary PAH metabolites and oral healthVariableIQRCrudeAdjusted^^P for trendOR (95%CI)P-valueP* _FDR_OR (95%CI)P-valueP _FDR_1-NAP0.989IQR 1Ref (-)IQR 20.76 (0.55–1.06)0.1050.2800.76 (0.55–1.06)0.1110.221IQR 30.74 (0.55–1.01)0.0600.0890.76 (0.55–1.06)0.1110.134IQR 41.09 (0.77–1.55)0.6300.9460.92 (0.65–1.29)0.6240.7492-NAP< 0.001IQR 1Ref (-)IQR 20.92 (0.68–1.22)0.5500.5500.91 (0.67–1.24)0.5620.674IQR 31.64 (1.20–2.25)0.0030.0171.58 (1.13–2.21)0.0090.028IQR 42.19 (1.52–3.15)< 0.001< 0.0011.96 (1.34–2.87)< 0.0010.0033-FLU0.839IQR 1Ref (-)IQR 20.83 (0.61–1.14)0.2630.3151.00 (0.67–1.48)0.9890.989IQR 30.95 (0.71–1.27)0.7190.7191.28 (0.77–2.13)0.3430.343IQR 41.04 (0.69–1.57)0.8480.9601.01 (0.40–2.56)0.9870.9872-FLU0.436IQR 1Ref (-)IQR 20.86 (0.66–1.12)0.2610.3150.83 (0.59–1.16)0.2850.428IQR 30.75 (0.58–0.97)0.0310.0610.62 (0.38–1.02)0.0620.094IQR 40.99 (0.70–1.41)0.9600.9600.68 (0.29–1.58)0.3730.5591-PHE0.430IQR 1Ref (-)IQR 20.79 (0.63–1.00.63.00)0.0560.2800.77 (0.60–0.98)0.0410.144IQR 30.80 (0.61–1.05)0.1100.1320.74 (0.55–1.00.55.00)0.0510.094IQR 40.88 (0.67–1.15)0.3420.6830.67 (0.47–0.95)0.0290.0581-OHP< 0.001IQR 1Ref (-)IQR 21.27 (0.93–1.74)0.1400.2801.38 (1.01–1.89)0.0480.144IQR 31.43 (1.08–1.89)0.0150.0451.65 (1.20–2.26)0.0030.016IQR 41.90 (1.41–2.57)< 0.001< 0.0012.26 (1.51–3.39)< 0.0010.001IQR interquartile range, 1-NAP 1-Hydroxynaphthalene, 2-NAP 2-Hydroxynaphthalene, 3-FLU 3-Hydroxyfluorene, 2-FLU 2-Hydroxyfluorene, *1-PHE 1-Hydroxyphenanthrene, 1-OHP 1-Hydroxypyrene, OR odds ratios 0.95%CI, 95% confidence intervals^^ Adjusted for sex, age, race, education, marital status, BMI, smoking status, alcohol consumption, poverty status, DII, and UA
Both the WQS regression and QGC models, adjusted for covariates, demonstrated that exposure to the PAH mixture was positively linked to an increased risk of poor oral health. 2-NAP and 1-OHP were the most influential drivers of this adverse overall effect in both models (Figure S3). The results of the exposure‒response relationship analysis for 2-NAP and 1-OHP are shown in Figure S4, revealing a nonlinear association for 2-NAP (P for nonlinear = 0.035).
The association between 2-NAP and 1-OHP with oral health was significantly mediated by TG and the TyG, with significant indirect effects and a proportional effect ranging from 4.13% to 4.87%. Furthermore, TyG-BMI served as a significant mediator in the association between 2-NAP and oral health, with a proportion mediated of 6.10%. In contrast, the TyG-BMI did not significantly mediate the link between 1-OHP and oral health (Fig. 1).Fig. 1. Mediation analysis of the association between urinary 2-NAP and 1-OHP and oral health by triglycerides and related indices. 2-NAP, 2-Hydroxynaphthalene. 1-OHP, 1-Hydroxypyrene. TG, triglyceride. TyG, triglyceride-glucose index. TyG-BMI, triglyceride-glucose-body mass index
A significant interaction effect was observed for race on the association between 2-NAP and oral health (P for interaction = 0.017), with the strongest effect observed among Hispanic participants (OR = 1.497, 95% CI: 1.276–1.756). In contrast, no significant interaction effects were detected for any of the other subgroups in the association between 1-OHP and oral health (Fig. 2).Fig. 2. Subgroup analysis of the associations between urinary 2-NAP and 1-OHP concentrations and oral health. 2-NAP, 2-Hydroxynaphthalene. 1-OHP, 1-Hydroxypyrene. OR, odds ratios. 95%CI, 95% confidence intervals
Sensitivity analyses employing stricter case definitions (n = 434 cases) showed largely consistent association patterns linking urinary PAH metabolites to oral health problems, compared with the primary analyses. Specifically, significant positive associations persisted for 1-NAP, 2-NAP, and 1-OHP (OR = 1.128, 95% CI: 1.021–1.246; OR = 1.230, 95% CI: 1.028–1.471; and OR = 1.180, 95% CI: 1.017–1.368, respectively), whereas 3-FLU tended towards significance (OR = 1.185, 95% CI: 1.000–1.405; P = 0.053). The direction of these associations aligned with the exposure‒response relationships observed in the primary analyses (Table S2).
Discussion
This study demonstrated significant associations between PAHs and poor oral health in adults aged ≥ 45 years. Both individual and mixture analyses consistently revealed that increased urinary concentrations of 2-NAP and 1-OHP were significantly linked to increased risk of oral diseases, with an exposure‒response relationship observed for 2-NAP. Mediation analyses indicated that TG and TyG mediated these associations, whereas TyG-BMI partially mediated them. Furthermore, subgroup analyses revealed a significant effect modification by race on the association between 2-NAP and oral health. These findings emphasise the public health relevance of both individual and combined PAH exposure as environmental determinants of the oral disease burden among adults aged 45 years and above.
Exposure to PAHs may negatively affect oral health through multiple mechanisms. Specifically, PAHs can initiate local inflammatory responses by activating aryl hydrocarbon receptors via their metabolites [28]. This activation enhances downstream inflammatory signalling and boosts the production of key pro-inflammatory cytokines [29–31]. These cytokines not only induce inflammation of the oral mucosa but also damage periodontal tissues, resulting in clinical manifestations such as gingival redness, swelling, and bleeding, thereby contributing to the development of periodontitis [32]. Furthermore, PAHs may disrupt intercellular interactions by altering the expression and distribution of key junctional complexes, thereby compromising the barrier function of the oral epithelium [33]. Consequently, PAHs can disrupt the oxidative–antioxidative balance by generating reactive oxygen species, subsequently activating apoptosis-related proteins, inducing apoptosis in oral epithelial cells, and ultimately contributing to the pathogenesis of conditions such as periodontitis, laryngitis, and oral cancer [34–36]. Moreover, PAHs can contribute to oral disease by inducing epigenetic changes in the oral cavity. For instance, dibenzo [def,p] chrysene alters gene expression during the early stages of oral cancer by causing hypomethylation within an intron of fibroblast growth factor 3 and hypermethylation within an intron of vesicle-associated membrane protein 3, thereby participating in the early development of oral cancer [37].
This study revealed that exposure to 2-NAP and 1-OHP is significantly associated with the occurrence of oral diseases. These findings both align and contrast with those of previous research. PAHs have been demonstrated to increase periodontitis risk [17] and to cause oral mucosal injury, with potential utility as oral cancer biomarkers [38]. Furthermore, positive correlations between periodontitis and both 3-OHF and 2-OHF have been reported [39]. These studies indicate that PAH exposure may adversely affect oral health by dysregulating inflammatory pathways and inflicting cellular damage via oxidative stress and DNA impairment.
Methodological variations distinguish this work from earlier reports. Unlike previous studies on the combined effects of heavy metals and PAHs on periodontitis [17], this analysis focused exclusively on PAHs. In contrast to a prior study that assessed PAH-related biological effects via DNA adduct measurement in oral cells using a limited sample size [38], this study utilised NHANES data, quantified urinary PAH metabolites, and included a larger participant cohort. Moreover, whereas earlier work examined only the independent associations of individual PAHs with periodontitis [39], this study is the first to apply WQS and QGC models to systematically quantify the overall oral health risk per quartile increase in a mixture of six PAHs, identifying 2-NAP and 1-OHP as the primary drivers. These discrepancies may stem from differences in sample size, study design, statistical approaches, and the specific PAH metabolites analysed.
The results of the mediation analysis conducted in this study revealed that lipid metabolism markers—specifically, TG and the TyG index (a surrogate indicator of insulin resistance)—significantly mediated the association between two typical PAH metabolites (2-NAP and 1-OHP) and oral health impairment, with mediation proportions ranging from 4.13% to 4.87%. Importantly, this study further revealed that different PAH monomers may influence health through distinct metabolic pathways: obesity-related insulin resistance, represented by TyG-BMI, significantly mediated the relationship between 2-NAP and oral health (proportion of 6.10%), whereas this effect was not observed in the pathway involving 1-OHP. These findings provide important mechanistic insight by suggesting that the impact of 2-NAP on oral health may be more dependent on insulin resistance pathways exacerbated by obesity. These findings align with those of previous research, which revealed that obesity is a key driver of insulin resistance and chronic inflammation [40, 41] and is capable of exacerbating metabolic disturbances and adversely affecting periodontal tissues. In contrast, the effects of 1-OHP are mediated primarily by lipid metabolic dysfunction and insulin resistance (as represented by the baseline TyG index), which appears largely independent of obesity status. This divergence may stem from heterogeneity in pharmacokinetics, receptor-binding affinity, or activation of specific toxic pathways among different PAH monomers. Although numerous studies have separately established independent pathways linking PAH exposure to metabolic dysregulation via oxidative stress and inflammation [42, 43] and connecting metabolic dysregulation to oral diseases [40, 41, 44], the present study integrated these segments by identifying specific serum biomarkers that mediate the relationship between individual PAH metabolites and oral health outcomes, thereby providing novel evidence for a continuous toxicological pathway from exposure to clinical outcome: environmental exposure to PAHs is involved in the pathogenesis of oral diseases partly through mechanistically disrupting host lipid and glucose metabolism. Nevertheless, the temporal sequence inferred from these mediation models warrants further validation in longitudinal studies. Such research should be designed to include biomarkers of oxidative stress and inflammation, with the aim of elucidating the broader mechanistic cascade connecting PAH exposure to oral health.
This study revealed that race was a significant effect modifier in the association between 2-NAPs and oral health, with the strongest effect observed in the Hispanic population; However, the analysis found no evidence of effect modification by any subgroup on the association between 1-OHP and oral health. These findings share both consistencies and differences with those of previous research. First, these results validate and extend prior observations—existing studies have reported that the associations between PAH metabolites and health outcomes may be modified by racial factors [26]. This study similarly identified a significant racial interaction effect for 2-NAP in the context of oral health, further supporting the view that demographic characteristics can amplify the health effects of PAHs. More importantly, these findings reveal that the Hispanic population is particularly vulnerable to the oral health effects of 2-NAP, expanding the understanding of race-specific risk patterns. Second, the results for 1-OHP in this study are consistent with those of previous research: similar to its lack of interaction effects in association with psoriasis [45], this study also found no subgroup interactions between 1-OHP and oral health, collectively suggesting that 1-OHP may have broader rather than specific health effects.
To investigate the relationship between urinary PAH metabolite levels and oral health, a common analytical strategy used in environmental epidemiology was applied for handling complex exposures—converting continuous concentrations into quartiles. This approach was selected for two main reasons: first, to capture potential nonlinear dose–response relationships while avoiding the loss of statistical power that may result from incorrectly assuming a linear model; and second, because quartile-based analysis provides more intuitive and robust risk estimates, which are less sensitive to outliers and easier to interpret. Notably, this methodological choice aligns with several recent studies on PAH-related health effects. For instance, Wu et al. [17], in their investigation of the relationship between PAHs and periodontitis, categorised metabolite concentrations into quartiles and identified 2-NAP and 1-OHP as key drivers using WQS and QGC models. Similarly, Dai et al. [46], in their study on PAHs and immunosuppression, adopted quartile categorisation and applied mixed models such as QGC to confirm the significant immunosuppressive effects of PAH exposure. Thus, this study follows a well-established analytical framework within this field, and the consistency of the results across different models further strengthens the reliability of the conclusions.
The observed link between PAH metabolites and oral health problems remained stable when different diagnostic thresholds were applied. This consistency strengthens confidence in the robustness of the relationship. These findings are consistent with those of earlier reports. A study by Wu et al. [47], utilising data from the NHANES 2009–2014, confirmed a positive association between six hydroxylated polycyclic aromatic hydrocarbons (OH-PAHs) and periodontitis. Notably, the significance of this positive association was maintained even after restricting the analysis to a subsample from 2011 to 2014, confirming the robustness of the link between OH-PAHs and periodontitis. The consistency between the findings of the two studies likely stems from a genuine and robust biological link between PAHs and oral health issues, an effect sufficiently strong to remain detectable across varying analytical conditions. Consequently, the present findings not only reinforce the reliability of the conclusions but also extend the scientific understanding of PAHs as significant environmental risk factors for periodontal disease.
Strength and limitations
This study is the first to elucidate the partial mediating role of triglyceride-related metabolic pathways in the link between exposure to specific PAH and poorer oral health among individuals aged 45 years and older, who have a high burden of oral diseases, thereby providing important clues for targeted prevention in high-risk populations. However, this study has several limitations. First, the categorisation of PAH metabolites into quartiles for analysis may increase the risk of multiple comparisons and false-positive findings; Although FDR correction was applied, the quartile-based analysis is still susceptible to multiple comparison error and false positives; this should be considered in interpretation. Second, the use of self-reported oral health status, rather than clinical assessment, may introduce recall bias or outcome misclassification, which could affect the accuracy of the findings. Additionally, the short biological half-lives of PAH compounds limit the reliability of single urinary metabolite measurements as indicators of long-term exposure. Furthermore, the external validity of these findings is confined to middle-aged and older populations, given the enrollment criteria requiring participants to be at least 45 years of age. Although this focus is justified by the higher disease burden in this group, the relationships between PAH exposure, TG-related indices, and oral health may differ in younger populations because of variations in physiology, exposure patterns, and lifestyle factors. Finally, although the models were adjusted for a wide range of covariates, residual confounding from unmeasured factors may persist. Notably, more granular determinants of personal exposure to atmospheric contaminants could not be obtained, such as individual time-activity patterns, microenvironmental pollution levels in domestic or occupational settings, or the use of protective equipment. Additionally, other unmeasured factors, including genetic susceptibility, oral hygiene practices, and access to dental care, represent potential sources of residual confounding. Therefore, future studies should employ longitudinal designs, incorporate clinical oral health assessments, and utilise repeated biomarker measurements to better establish causality and improve the accuracy of exposure and outcome evaluation.
Conclusion
This study demonstrated that specific PAH metabolites (2-NAP and 1-OHP) are significantly associated with an elevated risk of oral diseases in adults aged ≥ 45 years. This association is partly mediated by disruptions in lipid metabolism and the promotion of insulin resistance, with obesity exacerbating the adverse effects of 2-NAP. These findings have immediate clinical relevance. For patient care, clinicians should incorporate an assessment of PAH exposure risk into the evaluation of middle-aged and older adults, particularly those with obesity. This can be achieved by integrating targeted questions on environmental and occupational exposure histories into routine health assessments. Identifying high-risk individuals through this approach would enable earlier and more tailored oral health surveillance and preventive strategies. From a public health perspective, the results provide robust evidence for policies aimed at reducing environmental PAH exposure to improve population oral health.
Supplementary Information
Supplementary material 1.
Supplementary material 2.
Supplementary material 3.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Choi H, Kim CS. Polycyclic Aromatic Hydrocarbons from Fine Particulate Matter Induce Oxidative Stress and the Inflammatory Response in Human Vocal Fold Fibroblast Cells. Oxid Med Cell Longev 2021, 2021:5530390.10.1155/2021/5530390 PMC 835746634394826 · doi ↗ · pubmed ↗
- 2Ladeira LLC, Nascimento GG, Leite FRM, Alves-Costa S, Barbosa JMA, Alves CMC et al. Obesity, Insulin Resistance, Caries, and Periodontitis: Syndemic Framework. Nutrients 2023, 15(16):3512.10.3390/nu 15163512 PMC 1045848237630703 · doi ↗ · pubmed ↗