Outcomes of Alcohol Septal Ablation vs Transaortic Septal Myectomy in Elderly Patients With Obstructive Hypertrophic Cardiomyopathy
Tedy Sawma, Hartzell V. Schaff, Sina Danesh, Youssef Shahin, Steve R. Ommen, Joseph A. Dearani, Mackram F. Eleid, Jeffrey B. Geske

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
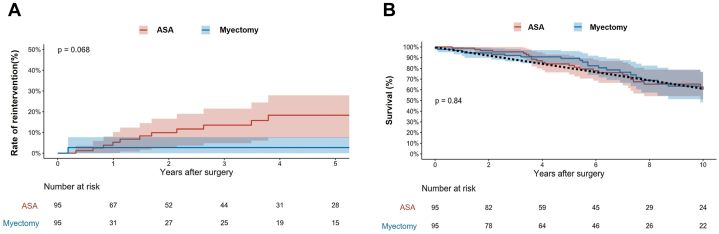 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiomyopathy and Myosin Studies · Cardiovascular Function and Risk Factors · Cardiovascular Conditions and Treatments
Obstructive hypertrophic cardiomyopathy is increasingly recognized in elderly patients.1^,^2 In patients with obstructive symptoms refractory to maximal medical therapy, septal reduction therapy, whether through alcohol septal ablation (ASA) or surgical septal myectomy, is indicated.3 ASA is often preferred for symptomatic patients who are considered to be at increased risk for surgery, and this includes many older patients. However, in high-volume-experienced centers, operative risks of septal myectomy are minimal (<1%) and long-term outcomes are well-established, even among older patients.2^,^4 There are few studies that compare outcomes of ASA vs myectomy in the elderly.5 The present investigation examines short- and long-term outcomes of septal reduction via ASA or septal myectomy in patients 75 years or older.
Methodology
The Mayo Clinic Institutional Review Board in Rochester, Minnesota, approved the study on November 26, 2024. All patients 75 years or older who underwent first-time ASA or transaortic septal myectomy between 2000 and 2024 were included. Patients with previous septal reduction therapy, those undergoing apical myectomy, and those with severe aortic stenosis or concomitant surgical procedures were excluded. The final study cohort consisted of 281 patients, of whom 119 underwent ASA and 162 myectomy.
Comprehensive resting 2-dimensional transthoracic Doppler echocardiography was performed in all patients preoperatively. Endpoints of the study were long-term survival, trends of residual maximal left ventricular outflow tract (LVOT) gradients, and the need for reintervention by ASA or myectomy.
Due to differences in baseline characteristics, propensity scores were generated and used to match patients in a 1:1 ratio. Matching variables included age, sex, body mass index, NYHA functional class, cerebrovascular disease, recent atrial fibrillation, renal failure, diabetes, hypertension, coronary artery disease, beta-blocker use, maximal LVOT gradient at presentation, and ejection fraction (Figure 1A). The Kaplan-Meier method and competing risk analysis were used to generate the curves for long-term survival and the rate of reintervention. To assess trends of residual LVOT gradients, a linear mixed-effect model was used with adjustment for propensity scores. Time was fitted in the model using natural splines to allow for nonlinear effects, and plots were generated with 95% CI. All analyses were performed on R software (version 4.4.2).Figure 1. Rate of Reintervention and Long-Term Survival Among Elderly Patients Undergoing ASA vs Septal Myectomy(A) Cumulative incidence curve illustrating the incidence of reintervention among patients undergoing alcohol septal ablation (ASA) vs septal myectomy. (B) Kaplan-Meier curve illustrating long-term survival among patients undergoing ASA vs septal myectomy.
Results
Prior to matching, patients undergoing ASA were older than those undergoing myectomy (79 years vs 77 years; P < 0.001) and more likely to be female (78% vs 65%; P = 0.015). Following propensity matching, 95 patients undergoing ASA were perfectly matched on all baseline characteristics to 95 patients undergoing myectomy. The median age of the matched group was 78 years (IQR: 76-80) (P = 0.4), and 70.5% were females (P = 0.62). Median septal thickness was 19 mm (17-22) (P = 0.86), and maximal LVOT gradient at presentation was 81 mm Hg (64-107) (P = 0.68).
Median volume of injected alcohol was 1.5 mL (1-1.8). Infused coronary arteries included the first septal perforator in 68 patients (35.6%), the second septal perforator in 10 (5.2%), both the first and second in 7 (3.7%), and the third septal perforator in 4 (2.1%).
Operative mortality was 0% in the ASA group and 1% (1 patient) in the myectomy group. Complete heart block necessitating permanent pacemaker implantation developed in 22 patients (23.2%) undergoing ASA and 10 (10.5%) undergoing myectomy (P = 0.02).
Survival in both cohorts was comparable to a U.S. age- and sex-matched general population (Figure 1B), and there was no significant difference in survival between the matched groups (P = 0.84).
Median maximal LVOT gradient prior to discharge was 25 mm Hg (5-61) in the ASA group and 5 mm Hg (5-9) in the myectomy group (P < 0.001). Differences in LVOT gradients persisted in late follow-up (Figure 1C). In the ASA group, 11 patients needed reintervention, 8 through surgical myectomy, and 3 through ASA. In the surgical group, 2 patients underwent repeat septal myectomy. The long-term rate of reintervention was higher in the ASA group (P = 0.06) (Figure 1D).
Discussion
Both ASA and surgical myectomy can be performed with low procedural risk at specialized hypertrophic cardiomyopathy (HCM) centers, regardless of patient age at presentation.2^,^5^,^6 This is reflected by the minimal operative mortality seen in this cohort of obstructive hypertrophic cardiomyopathy patients ≥75 years. Complete heart block requiring pacemaker insertion was 2-fold higher in the ASA group than in the myectomy group, and this is consistent with previous studies.7
An important finding of this study is that long-term mortality rates were comparable between the 2 groups and similar to that of a sex- and age-matched population. Notably, in a younger study group, Cui et al reported that while the risk of death is similar over the first 3 years following either ASA or myectomy, survival subsequently favors myectomy.8 For elderly patients, such as those in our cohort >75 years, the potential benefit of surgical myectomy on late survival seen in younger patients may be less important than the risk and impact of the procedure on quality of life. This again emphasizes the importance of an experienced multidisciplinary HCM team when evaluating treatment options.
Interestingly, LVOT gradient relief is more complete after septal myectomy than ASA at both early and late follow-up. This is further reflected by the relatively higher rates of reintervention observed in patients undergoing ASA compared to myectomy (P = 0.06). Lack of statistical significance likely reflects insufficient statistical power (small sample size).
In conclusion, both ASA and surgical myectomy are safe and effective options for septal reduction therapy in elderly patients with refractory obstructive symptoms. Surgical myectomy provides more complete relief of LVOT gradients but early and long-term clinical outcomes are generally similar with the 2 therapies.
Funding support and author disclosures
This work has been supported by the Tsai Family. The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Canepa M.Fumagalli C.Tini G.Temporal trend of age at diagnosis in hypertrophic cardiomyopathy: an analysis of the international sarcomeric human cardiomyopathy registry: an analysis of the international sarcomeric human cardiomyopathy registry Circ Heart Fail 132020 e 00723010.1161/CIRCHEARTFAILURE.120.007230 PMC 749748232894986 · doi ↗ · pubmed ↗
- 2Sawma T.Schaff H.V.Juarez-Casso F.Clinical features and postoperative outcomes in elderly patients undergoing septal myectomy for hypertrophic cardiomyopathy J Thorac Cardiovasc Surg 1702024532541.e 43938941610.1016/j.jtcvs.2024.09.050 · doi ↗ · pubmed ↗
- 3Ommen S.R.Ho C.Y.Asif I.M.2024 AHA/ACC/AMSSM/HRS/PACES/SCMR guideline for the management of hypertrophic cardiomyopathy: a report of the American heart association/American college of cardiology joint committee on clinical practice guidelines J Am Coll Cardiol 832024232424053872764710.1016/j.jacc.2024.02.014 · doi ↗ · pubmed ↗
- 4Alashi A.Smedira N.G.Popovic Z.B.Characteristics and outcomes of elderly patients with hypertrophic cardiomyopathy J Am Heart Assoc 102021 e 01852710.1161/JAHA.120.018527 PMC 795545033506683 · doi ↗ · pubmed ↗
- 5Mentias A.Smedira N.G.Krishnaswamy A.Survival after septal reduction in patients >65 years old with obstructive hypertrophic cardiomyopathy J Am Coll Cardiol 8120231051153663120410.1016/j.jacc.2022.10.027 · doi ↗ · pubmed ↗
- 6Mitchell C.Rahko P.S.Blauwet L.A.Guidelines for performing a comprehensive transthoracic echocardiographic examination in adults: recommendations from the American society of echocardiography J Am Soc Echocardiogr 3220191643028259210.1016/j.echo.2018.06.004 · doi ↗ · pubmed ↗
- 7Talreja D.R.Nishimura R.A.Edwards W.D.Alcohol septal ablation versus surgical septal myectomy: comparison of effects on atrioventricular conduction tissue J Am Coll Cardiol 442004232923321560739410.1016/j.jacc.2004.09.036 · doi ↗ · pubmed ↗
- 8Cui H.Schaff H.V.Wang S.Survival following alcohol septal ablation or septal myectomy for patients with obstructive hypertrophic cardiomyopathy J Am Coll Cardiol 792022164716553548375110.1016/j.jacc.2022.02.032 · doi ↗ · pubmed ↗